
OBGYN consultant, MD, MSc, PhD 🇨🇭interested in Endometriosis and Reproductive surgery, Editorial Board Member BMC Women’s Health
Joined November 2020
- Tweets 128
- Following 213
- Followers 107
- Likes 445
27 Photos and videos






Kalaitzopoulos Dimitrios Rafail retweeted

Feb 15
WESINAR: Discover key insights and themes from ESHRE 2025,.
23 Feb 2026 | 10:00am PST | 7:00pm CET
Moderator: Dimitrios Kalaitzopoulos
Speakers: Connie Rees, Anna Stepniewska, Laura Benaglia
👉 Register: tinyurl.com/pshk6xvm
#WESinar #Endometriosis
@DKalaitzopoulos

2
2
96
Kalaitzopoulos Dimitrios Rafail retweeted

29 Nov 2025
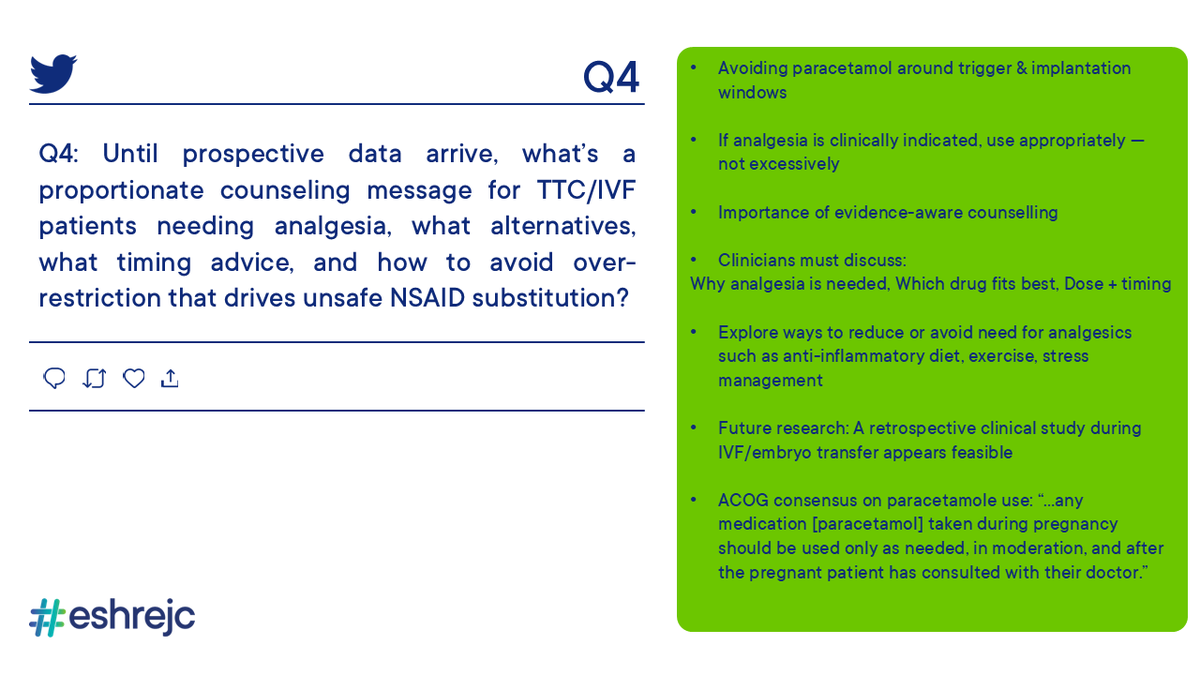
Summary of que 4⃣ moderated by @DKalaitzopoulos
#ESHREjc
28 Nov 2025

Q4: #ESHREjc Until prospective data arrive, what’s a proportionate counseling message for TTC/IVF patients needing analgesia, what alternatives, what timing advice, and how to avoid over-restriction that drives unsafe NSAID substitution? @ESHRE
6
4
525
Kalaitzopoulos Dimitrios Rafail retweeted

28 Nov 2025
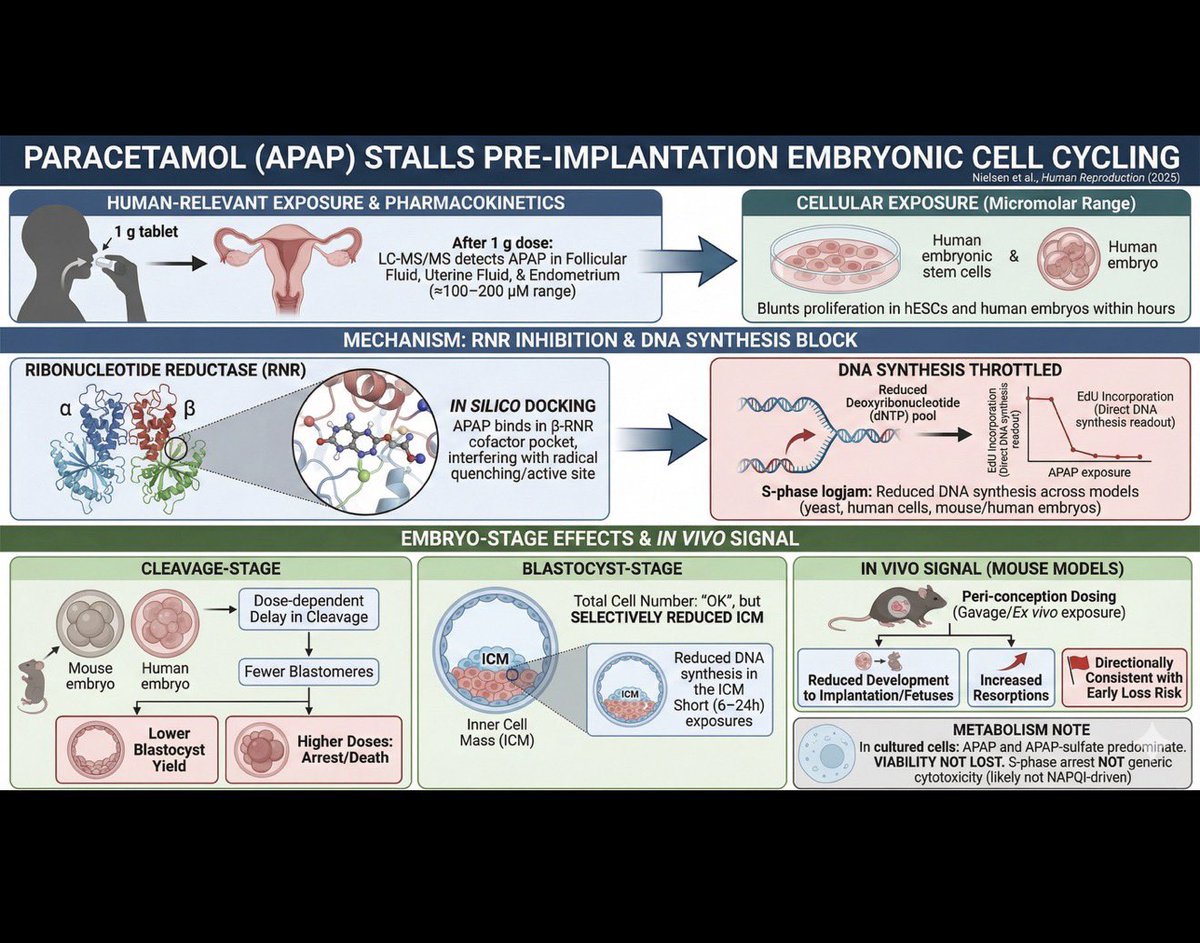
Over the next 24h will be engaging in discussion for a very common medication and its effect in embryological outcomes #ESHREjc 👇🏻

This edition’s paper is “Paracetamol (N-acetyl-para-aminophenol) disrupts early embryogenesis by cell cycle inhibition” published in our science journal Human Reproduction 👩🎓
🔗doi.org/10.1093/humrep/deaf1…
#ESHREjc
1
2
100
Kalaitzopoulos Dimitrios Rafail retweeted

28 Nov 2025
🚨Q1 #ESHREjc The study finds that APAP delays cleavage-stage divisions, while blastocysts keep total cells but show reduced ICM and DNA synthesis. What do these stage-specific vulnerabilities imply for implantation and embryo competence?
@ESHRE
11
5
8
519
Kalaitzopoulos Dimitrios Rafail retweeted

27 Nov 2025
1/ This #ESHREjc we are discussing how a common analgesic Acetaminophen (APAP) may interfere with pre-implantation embryo development.
Study in focus: doi.org/10.1093/humrep/deaf1…
A tweetorial to get you up and ready for tomorrow.
#ESHREjc @ESHRE
2
7
12
459
Kalaitzopoulos Dimitrios Rafail retweeted
25 Nov 2025
🚨 Could a common painkiller disrupt the earliest stages of human embryo development?
Join us for the next #ESHREjc
🗓️ 28–29 November
⏰ 17:00 CET start
📍 on @ESHRE
🔗 doi.org/10.1093/humrep/deaf1…
🌟 @juliauraji, Thanos Papathanasiou & David Kristensen

1
4
10
910

28 Sep 2025
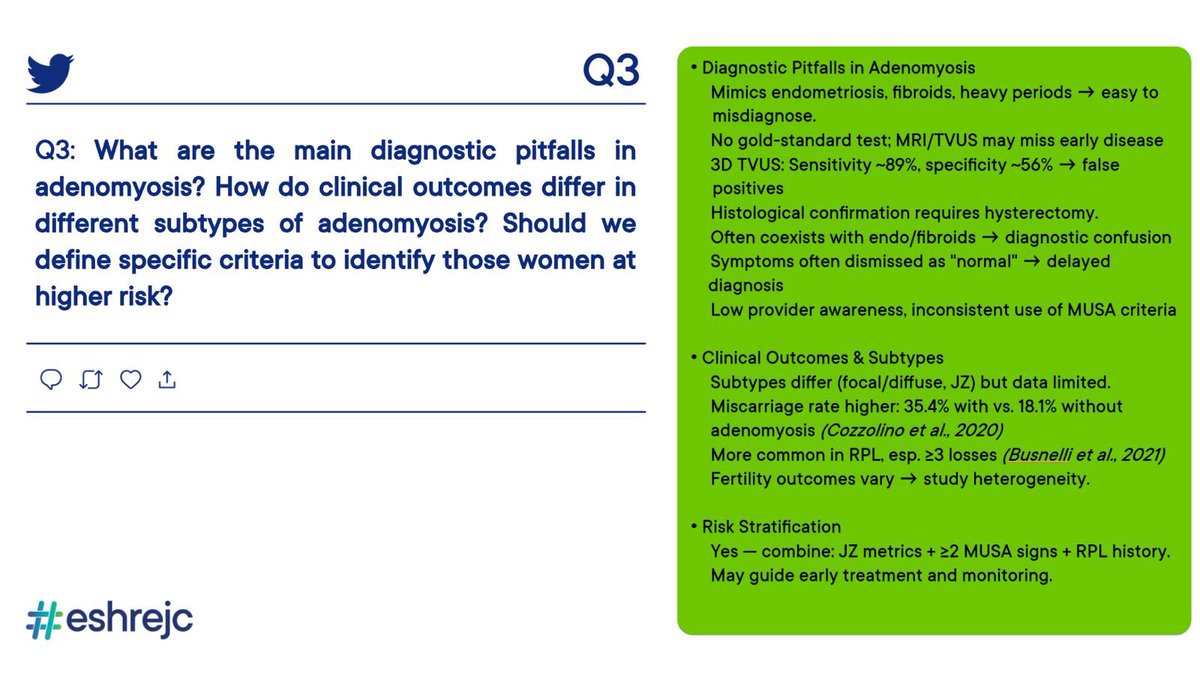
Q3 on diagnostic pitfalls in adenomyosis and clinical outcomes in subtypes of adenomyosis #eshrejc
By @GLiperis
26 Sep 2025

Q3: What are the main diagnostic pitfalls in adenomyosis? How do clinical outcomes differ in subtypes of adenomyosis? Should we define specific criteria to identify those women at higher risk? #ESHREjc @CatenaUrsula
@AlexQuaas
7
6
897
28 Sep 2025
Q4 on “ideal” setting of IVF
#eshrejc
By @NoemiSalme30386
26 Sep 2025

Q4: Moving into the “ideal” setting of IVF.
✨LBR after multiple ET reach 60–70% in women <35 years….
🔎to what extent can the remaining failure be explained by uterine factors? could this account for the entire 30–40%? Or are we missing something else? #ESHREjc

5
7
1,301
28 Sep 2025
Q2 on the role of diagnostic criteria of uterine anomalies
By @AttilioDGM7
26 Sep 2025

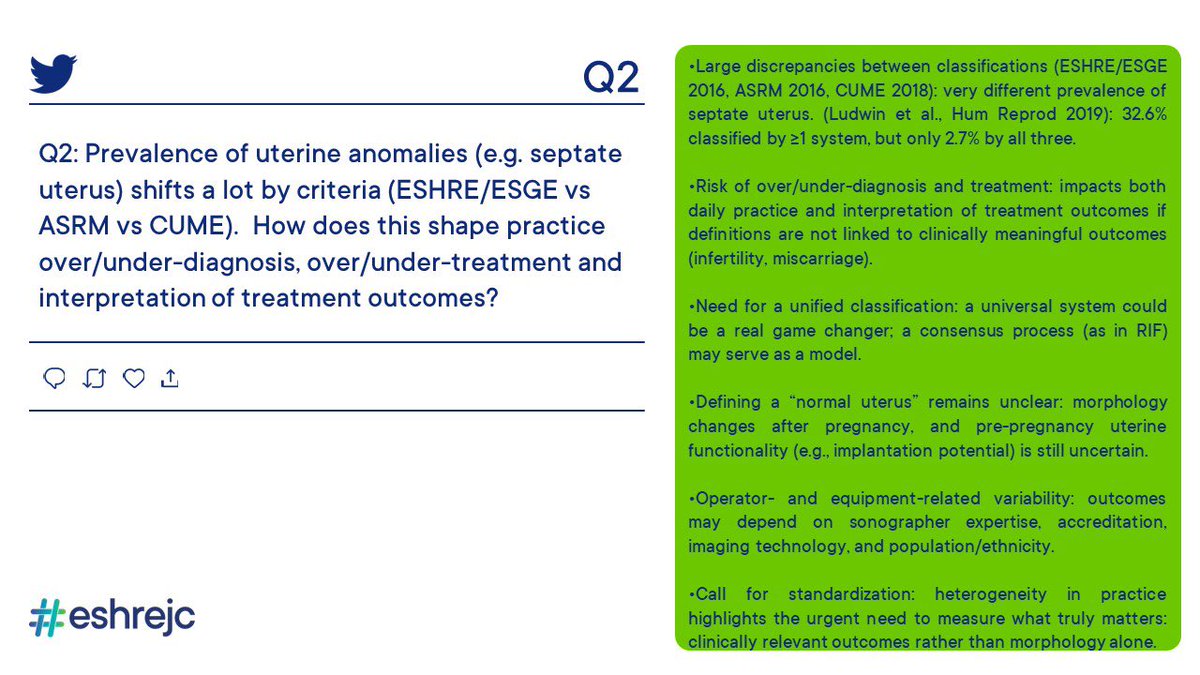
🚨Q2:
Prevalence of uterine anomalies (e.g. septate uterus) shifts a lot by criteria (ESHRE/ESGE vs ASRM vs CUME).
👉🏼How does this shape practice over/under-diagnosis, over/under-treatment and interpretation of treatment outcomes?
#ESHREJC

4
7
891
28 Sep 2025
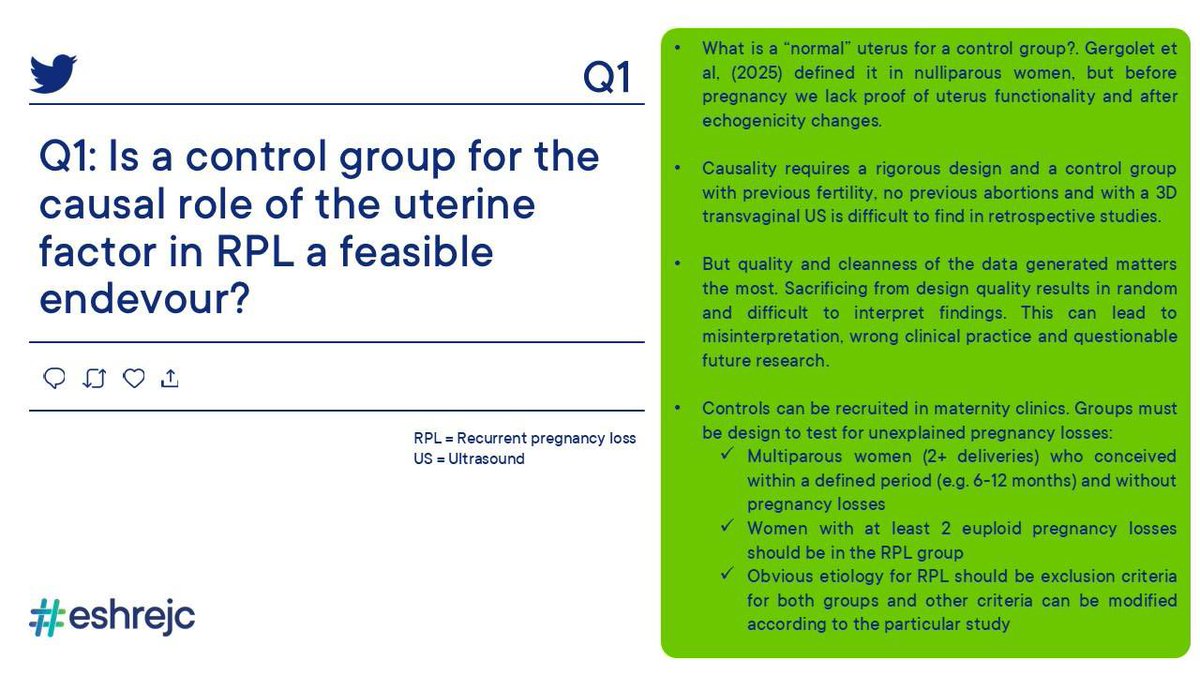
Q1 on control group for the role of uterine factor in RPL #eshrejc
By @juanjo_fraire
26 Sep 2025

Q1: To demonstrate a causal role of the uterine factor on RPL, a control group of 👭is needed with
-previous fertility
-no previous abortions
-with a 3D transv US
Is this a feasible endevour? Can causality be inferred even if diagnostic guidelines are heterogeneous? #ESHREjc
4
4
675

Many thanks to all participants 🙌 and to @DKalaitzopoulos and his team for leading this great edition of the #ESHREjc
1
5
8
406
Kalaitzopoulos Dimitrios Rafail retweeted

26 Sep 2025
Adenomyosis is a “shades of gray” rather than “black and white” condition so it is challenging to establish association vs causation and clinical relevance.
1
1
4
67
Kalaitzopoulos Dimitrios Rafail retweeted

27 Sep 2025
Should we define high-risk criteria?
Yes — combining:
Quantitative JZ metrics.
Number of MUSA features (≥2 direct signs).
Clinical phenotype (primary RPL, multiple losses).
This could identify women most likely to benefit from early interventions or closer monitoring.
1
3
70
Kalaitzopoulos Dimitrios Rafail retweeted

26 Sep 2025
Q4: Moving into the “ideal” setting of IVF.
✨LBR after multiple ET reach 60–70% in women <35 years….
🔎to what extent can the remaining failure be explained by uterine factors? could this account for the entire 30–40%? Or are we missing something else? #ESHREjc
2
5
8
1,199
Kalaitzopoulos Dimitrios Rafail retweeted
26 Sep 2025
Q3: What are the main diagnostic pitfalls in adenomyosis? How do clinical outcomes differ in subtypes of adenomyosis? Should we define specific criteria to identify those women at higher risk? #ESHREjc @CatenaUrsula
@AlexQuaas
16
9
10
1,704
Kalaitzopoulos Dimitrios Rafail retweeted
26 Sep 2025
🚨Q2:
Prevalence of uterine anomalies (e.g. septate uterus) shifts a lot by criteria (ESHRE/ESGE vs ASRM vs CUME).
👉🏼How does this shape practice over/under-diagnosis, over/under-treatment and interpretation of treatment outcomes?
#ESHREJC
4
5
8
1,684
This edition’s paper is “The importance of the ‘uterine factor’ in recurrent pregnancy loss: a retrospective cohort study on women screened through 3D transvaginal ultrasound” published in our science journal Human Reproduction 👩🎓
🔗 doi.org/10.1093/humrep/deae1…
#ESHREjc
1
5
7
285
Kalaitzopoulos Dimitrios Rafail retweeted
26 Sep 2025
Interesting point 👀.
A control group with prior fertility, no miscarriages, and 3D US would be valuable to test the uterine factor’s causal role in RPL.
👉 The challenge is recruitment, plus heterogeneous diagnostic guidelines make causal inference tricky.
#ESHREJc
3
4
495
Kalaitzopoulos Dimitrios Rafail retweeted

26 Sep 2025
Q1: To demonstrate a causal role of the uterine factor on RPL, a control group of 👭is needed with
-previous fertility
-no previous abortions
-with a 3D transv US
Is this a feasible endevour? Can causality be inferred even if diagnostic guidelines are heterogeneous? #ESHREjc
9
3
7
1,347