
Do you know someone with Parkinson's disease?
This is your opportunity to help them and advance medical research by participating in a clinical trial with CMAX.
Eligible participants will be paid for their time.
Find out more: hubs.la/Q04k_98p0

Just because CMax says it is NO WHERE in the Bible does not make this statement true. God's Word is Truth (John17:17). If it is Truth, then EVERYTHING, and I mean EVERYTHING is subject to it. All men, traditions, institutions, etc are subject to man's sin - His Word isn't.
12


Yazi abantu on these streets ve wild imagination. When recess starts Makhimba gets transferred back to Qalabusha coz the defence has not made any application for him to remain at CMax. The 2nd issue, is that Gininda was in the dock for 2 weeks & the defence failed to damage any of his testimony. You can all twerk about G but some of us even remember Mnisi Manikiniki losing his composure coz of G’s answers. Bringing Q was a disaster for the defence. They must also bring Makhubo, Brig Buthelezi, Kelly, Longwe & permanently kill their own case.
21

What gets buried in the “first oral anabolic” commercial framing is the underlying biology challenge: Entera’s N-Tab® platform must achieve systemic absorption of PTH(1-34), a 34-amino-acid peptide, at plasma concentrations sufficient to drive anabolic bone remodeling. Today’s Late-Breaking Oral at ENDO 2026 confirms that for $ENTX, the formulation transition from multi-tablet to single tablet does not compromise that threshold.
🦴 Single-tablet EB613 achieved AUC, Cmax, and Tmax comparable to both the multi-tablet Phase 2 formulation and subcutaneous Forteo® (teriparatide), with comparable calcemic response and PTH(1-84) suppression across all three arms in a Phase 1 crossover study of 15 healthy participants, confirming full pharmacological equivalence of the simplified formulation.
globenewswire.com/news-relea…
Teriparatide’s mechanism is well-characterized: intermittent PTH(1-34) exposure triggers net osteoblast-mediated bone formation by transiently upregulating anabolic signaling, while pulsatile rather than continuous administration avoids the catabolic shift associated with sustained PTH elevation. The critical pharmacological requirement for any oral formulation is not just reaching systemic circulation, it is producing the sharp pulsatile Cmax that separates anabolic from catabolic PTH effect. Today’s data, showing comparable Cmax and Tmax for single-tablet EB613 versus Forteo® with a slightly shorter duration of exposure consistent with prior Phase 1 results, suggests the N-Tab® delivery system is preserving the essential pulsatile PK signature through the oral route.
The Phase 2 clinical foundation is solid: published in JBMR 2024, 161 postmenopausal women with osteoporosis, all biomarker and BMD endpoints met. EB613 2.5 mg produced dose-proportional increases in bone formation markers, reductions in bone resorption markers, and significant gains in lumbar spine, total hip, and femoral neck BMD at six months. The September 2025 ASBMR data added 3D-DXA analysis showing increases in integral and trabecular volumetric BMD, cortical thickness, and cortical surface BMD at the total hip and femoral neck, with cortical improvements described as comparable to published injectable teriparatide data. Today’s bridging study confirms the simplified single-tablet formulation carries those properties forward unchanged into the Phase 3 candidate.
The regulatory pathway is 505(b)(2), with Forteo® as the reference listed drug. FDA gave written agreement in July 2025 that BMD is an acceptable primary endpoint, the single most important regulatory gate for the Phase 3 design. The planned study is multinational, randomized, double-blind, placebo-controlled, in 750 postmenopausal women with osteoporosis, with primary endpoint: percentage change in total hip BMD from baseline to month 12. An extension study is also planned to evaluate 24 months of EB613 monotherapy and a 12-month EB613 followed by anti-resorptive sequence.
The epidemiological context is large: more than 2 million osteoporotic fractures annually in the US, with 20 to 24% of hip fracture patients dying within one year. Every approved anabolic therapy requires injection; a clinically equivalent oral tablet would directly address the adherence and prescriber-uptake barriers that suppress anabolic adoption today. The clinical read that will resolve the central thesis is the 12-month total hip BMD endpoint in Phase 3; secondary 3D-DXA cortical bone data will carry additional weight given the ASBMR 2025 signal, and FDA’s near-term response to the March 2026 protocol submission is the gate that determines when patient enrollment can begin.
_
Paid Ad via #WallStWire: This account is operated by Wall Street Wire. Entera Bio Ltd. or a related party has paid Wall Street Wire for ongoing promotional services. Full compensation and paying party disclosure: wallstwire.ai/disclosures. Our content is not financial advice.
32

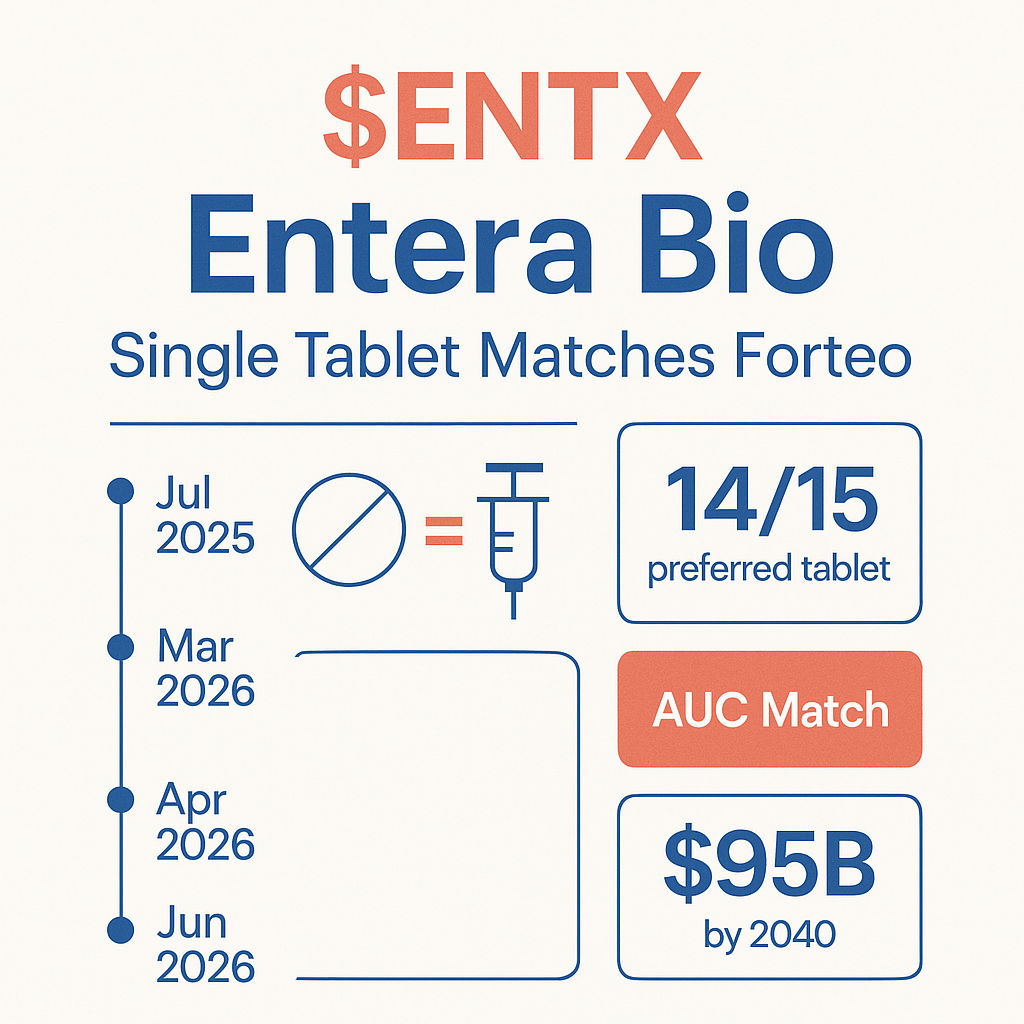
What does it take to replace a daily injection with a once-a-day pill for a chronic disease affecting one in three women over age 50? This week at ENDO 2026, $ENTX provided a clinical answer.
Osteoporosis drives more than 2 million fractures annually in the United States, and total medical costs are projected to rise from $57 billion in 2018 to $95 billion by 2040. Three anabolic treatments are approved: Forteo®, Tymlos®, and Evenity®. All require injections. All are used in a fraction of eligible patients. The route of administration is a documented barrier to adherence and prescriber uptake.
Today’s Phase 1 data, presented as a Late-Breaking Oral at the Endocrine Society’s annual meeting in Chicago, shows that Entera’s single tablet EB613 delivers comparable AUC, Cmax, and Tmax to both the multi-tablet version that succeeded in Phase 2 and to subcutaneous Forteo®. Pharmacodynamic comparability was also confirmed. Safety was clean. And all 15 trial participants preferred daily oral EB613 over the daily injection, with 14 of 15 preferring the single tablet over the multi-tablet format.
globenewswire.com/news-relea…
The next update from Entera will reveal whether FDA has accepted the Phase 3 protocol submitted in March 2026. That response, described as expected imminently in the company’s Q1 2026 filing, sets the timeline for enrolling 750 patients in the first registrational study of an oral anabolic for osteoporosis.
_
Paid Ad via #WallStWire: This account is operated by Wall Street Wire. Entera Bio Ltd. or a related party has paid Wall Street Wire for ongoing promotional services. Full compensation and paying party disclosure: wallstwire.ai/disclosures. Our content is not financial advice.
23

After a decade of being told you cannot absorb a peptide through the gut at therapeutically meaningful concentrations, $ENTX turned up at ENDO 2026 with Phase 1 data showing a single oral PTH(1-34) tablet matched the AUC of the injectable gold standard. The argument about whether the platform works is now settled.
🦴 Single-tablet EB613 matched Forteo AUC, Cmax, and Tmax in Phase 1 crossover study.
📊 14 of 15 participants preferred single tablet; 15/15 preferred oral over daily injection.
🏛️ Phase 3 protocol submitted to FDA in March 2026; written feedback expected imminently.
💰 BVF Partners invested $10M in April 2026, with up to $14.5M more via warrant exercise.
📅 Cash runway through Q1 2027; Phase 3 design: 750 patients, 12-month BMD primary endpoint.
globenewswire.com/news-relea…
What makes today’s data strategically decisive is the trajectory it completes. In July 2025, FDA gave Entera written agreement that BMD is an acceptable primary endpoint for Phase 3. In September 2025 at ASBMR, Phase 2 data demonstrated EB613 improved both trabecular and cortical bone at six months, with cortical gains explicitly compared to injectable teriparatide. In March 2026, Entera submitted a full Phase 3 protocol for 750 patients. In April 2026, BVF, a specialized healthcare fund, committed $10 million with warrants for up to $14.5 million more. Today’s bridging data closes the loop: the single tablet going into Phase 3 is pharmacokinetically indistinguishable from the multi-tablet that succeeded in Phase 2.
That is not an administrative detail. It matters because Entera is using a 505(b)(2) regulatory pathway that references FDA’s approval of Forteo® (teriparatide, approved 2002). The Phase 3 is not an exploratory study asking whether oral PTH works. It is a confirmatory study asking whether this formulation, in this patient population, produces the BMD improvement that Phase 2 demonstrated and that two decades of teriparatide literature supports. A narrower scientific ask means a structurally lower trial design risk profile than a typical first-in-class Phase 3.
The harder question is commercial reach. Osteoporosis is medicine’s most underprescribed large market. Over 2 million fractures annually in the US. Costs rising to $95 billion by 2040. Three approved anabolics, all injectable, all used in a minority of eligible patients. Today’s patient preference data (100% of participants chose oral, 14/15 chose single tablet over multi-tablet) is not a registrational endpoint, but it speaks directly to the adoption thesis: patients want this if it works.
The immediate inflection is FDA’s response to the March 2026 protocol submission. Entera characterized that response as expected imminently in the May 2026 quarterly update. A clean acceptance without clinical hold would allow enrollment to begin within months, converting today’s scientific validation into Phase 3 execution. That is when this story moves from data readouts at medical society meetings to patient randomization.
globenewswire.com/news-relea…
_
Paid Ad via #WallStWire: This account is operated by Wall Street Wire. Entera Bio Ltd. or a related party has paid Wall Street Wire for ongoing promotional services. Full compensation and paying party disclosure: wallstwire.ai/disclosures. Our content is not financial advice.
31

This morning at ENDO 2026 in Chicago, 15 healthy participants answered the central question in Entera Bio’s Phase 3 preparation: can a single oral tablet match the pharmacokinetic profile of a daily subcutaneous injection?
The Phase 1 bridging study (NCT05965167), with data presented as a Late-Breaking Oral at the Endocrine Society’s annual meeting, says yes. $ENTX’s single tablet EB613 showed comparable Cmax, Tmax, and total systemic exposure (AUC) to the multi-tablet formulation Entera used in its successful 161-patient Phase 2 study. The AUC also proved comparable to subcutaneous Forteo® (teriparatide, Eli Lilly), the FDA-approved injectable that has been the anabolic standard since 2002.
Pharmacodynamic markers matched too. Comparable calcemic effects and suppression of endogenous PTH(1-84) were recorded across all three treatment arms. Safety was consistent with Forteo®, with no drug-related serious adverse events. Patient preference: 14 of 15 participants preferred the single tablet over the multi-tablet formulation, and all 15 preferred a daily oral pill over a daily injection.
That last point matters for Phase 3 enrollment and, ultimately, commercial adoption. Every approved anabolic for osteoporosis requires injections. Entera’s entire thesis is that oral administration changes the uptake equation. Today’s data closes the formulation gap between the Phase 2 multi-tablet candidate and the simpler single tablet that will go into Phase 3.
FDA feedback on the Phase 3 protocol, submitted by Entera in March 2026, is expected imminently per the company’s Q1 2026 report. Phase 3 is planned for 750 postmenopausal women with a 12-month total hip BMD change as the primary endpoint.
globenewswire.com/news-relea…
_
Paid Ad via #WallStWire: This account is operated by Wall Street Wire. Entera Bio Ltd. or a related party has paid Wall Street Wire for ongoing promotional services. Full compensation and paying party disclosure: wallstwire.ai/disclosures. Our content is not financial advice.
16
くすりやのひとりごと retweeted

Jun 13
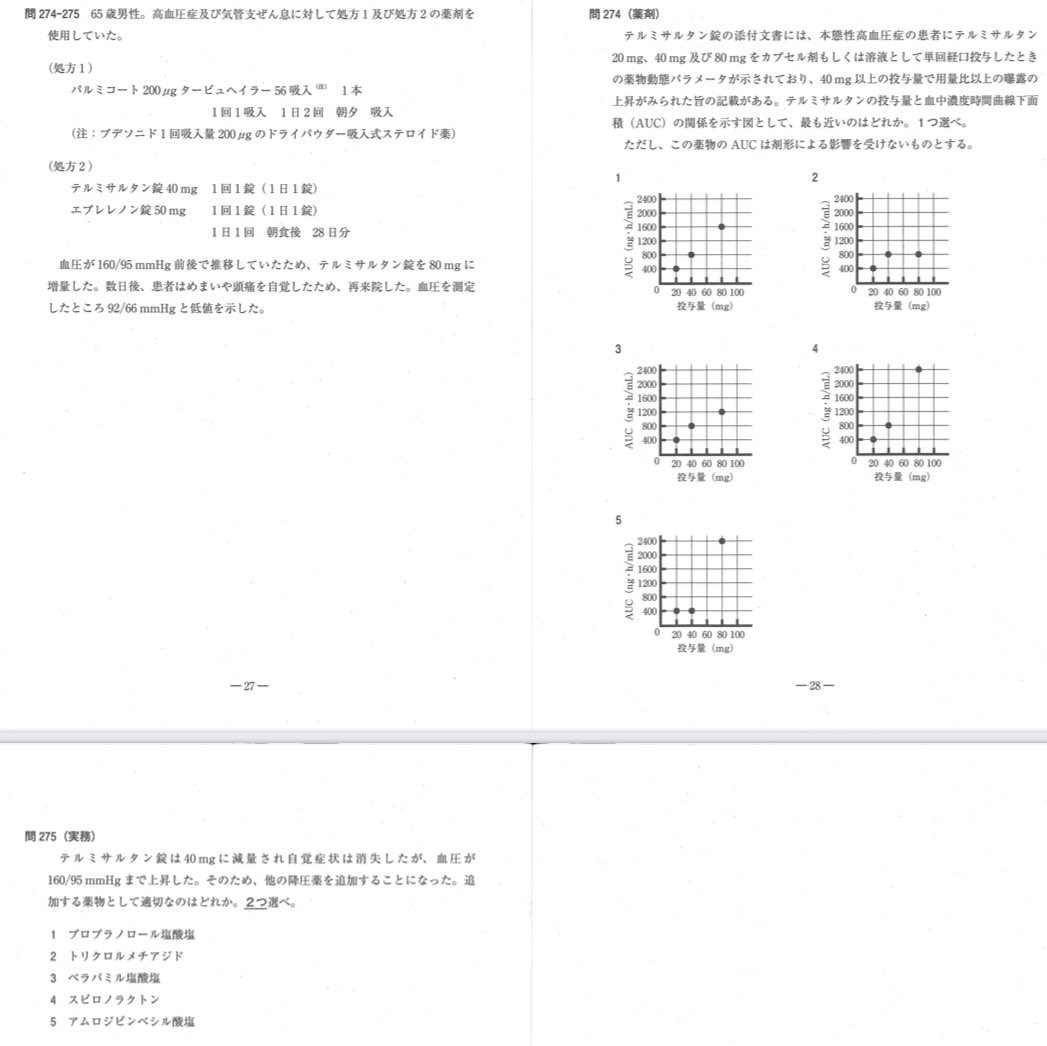
ちなみにテルミサルタン(半減期長いことで有名)の血中濃度は非線形なので40mg→80mgは2倍以上!である
じゃあ何倍か→Cmax は5倍、AUCは3倍くらい
(小腸壁での抱合能の飽和及び肝臓への分布の飽和によるもの)
でも、40mgから80mgへ増量しても日中のピーク時の血圧はそこまで大きく下がりません。
じゃあ80mgの良さは??
→ 日中でピークの血圧を下げすぎることなく、この長い半減期の恩恵を最大限に引き出し、翌朝まで強力にRAAS(レニン・アンジオテンシン・アルドステロン系)を抑制し続けることができます。
早朝🟰1日の中で脳卒中や心筋梗塞といった致死的な心血管イベントが最も起こりやすい「魔の時間帯」をカバー
「テルミサルタン80mg→翌朝の最も危険な時間帯まで、RAAS抑制の分厚いバリアを残しておける」と解釈できるかもしれません
また、降圧効果は用量依存ではないが、アルブミン尿の改善(腎保護)は用量依存
23 Feb 2025

よし おいさんが解説してやるわ
前半はテルミサルタンの非線形とか知らなくとも解ける
日本語できますか問題
問274
めまい頭痛と実際の数値から過降圧、
問題文にテルミの効果が用量と比例していない→右肩上がりあげぽよカーブになるはず
答えは4
問275
✅喘息ある→プロプラノロール使いたくないなあ (⚠️喘息あっても心不全HFrEFならカルベジロール良い、ビソプロロールもβ1選択的ブロックでベター)
✅トリクロルメチアジド→まあいいんじゃない
✅ベラパミル→なんでやねん!脈落とすんか
受験生落とすんか?カルシウム拮抗剤違い狙いかしら
✅スピロラクトン→エプレレノン使っているのでカリウム爆上げ禁忌
✅アムロジピン→まあいいんじゃない
答え2、5
#薬剤師国家試験110回
2
15
164
22,153

An open invitation to every ED drug manufacturer in the market.Join our next fed-state clinical study.No pitch. No marketing. Just science.Here is what the published literature shows:Sildenafil taken with food: peak plasma concentration decreases by 29%. Time to onset delayed by 60 minutes. Statistically significant. Peer-reviewed. Not disputed.That is Pfizer's own data. Published in the British Journal of Clinical Pharmacology. Available to every company in this space.Here is what our data shows:Clinical studies demonstrated rapid absorption, with measurable sildenafil detected in the bloodstream within 5 minutes and therapeutic plasma levels typically reached within 10 to 20 minutes. Unlike conventional sildenafil tablets, HEZKUE maintained favorable pharmacokinetics even after food intake, helping to overcome the well-documented food effect associated with traditional ED therapies.In the fed-state crossover study, mean Cmax for HEZKUE was 488 ng/mL. Conventional sildenafil tablets under identical conditions: approximately 350 ng/mL. Fed or fasted. No meaningful difference in absorption.HEZKUE's liquid formulation uses buccal and esophageal absorption, bypassing the gastric breakdown that slows every tablet on the market.Published. Peer-reviewed. Journal of Sexual Medicine. Oxford University Press. Authors from Mount Sinai, University of Michigan, and Ludwig Maximilian University of Munich.We ran the fed study. We published the results. Now we are asking the rest of the industry to do the same.Aspargo is conducting the next phase of fed-state absorption research for sildenafil oral spray. We are formally inviting every manufacturer in this category to submit their formulation for parallel testing under identical fed-state conditions.Same protocol. Same patients. Same meal. Same lab.One study. Every formulation. Published results.If your product performs in the real world, prove it. We will publish whatever the data shows. Ours included.This is what patient-first actually looks like. Not a tagline. A clinical protocol.If you represent one of these companies and you want to participate, or if you are a clinician, researcher, or patient advocate who believes this study should exist, reach out directly.The patients already ran the experiment. Millions of times. In their own homes. Without knowing the results were never designed to match their lives.It is time we ran it properly.Read the published data here: academic.oup.com/jsm/article… more about HEZKUE: hezkuedirect.com

46

Hafif nemliyken Dikmen’de şu 931. caddeyi Honda Civic ve Cmax ile zikzak yapa yapa çıkmıştım.

1
82

Jun 14
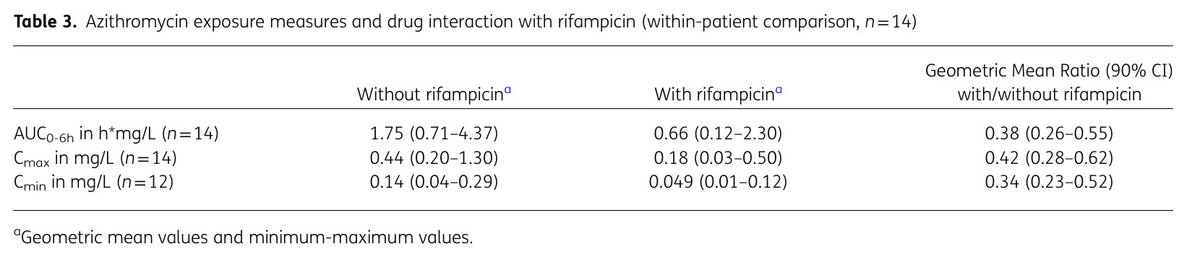
NTM治療におけるRFP曝露とAZM血中濃度の影響 - Journal of antimicrobial chemotherapy (2026)
・RFP併用時にAZMのAUC0–6hが62%, Cmaxが58%, Cminが66%低下した
・アウトカムとの明確な関連は示されず
academic.oup.com/jac/article…

6
382

Jun 14
O CMAX..... O CMAX TOCOU IN MY MIND!!!!
ALI EU FUI PROS KRL KKKKKK
1
29

