

18h
"It's just a gallbladder."
Also
"Patient not stable enough for decompressive flex sig. Suggest surgery."
1
13
1,446

En los albores del s. XXI y a través de The Authority, Ellis fue uno de los responsables del advenimiento del decompressive storytelling en el cómic comercial USA. Con Global Frequency, sin tanto éxito, busco la reivindicación de la grapa como unidad narrativa válida en si misma.

1
34

Jun 13
as a mom, I encourage mandatory decompressive time outs for yourself no matter how smooth the day going.
10

Jun 13
Good observation. These findings are postoperative. The treating team initially interpreted the case as a large MCA infarction and performed decompressive craniectomy. The temporal bone defect and subcutaneous emphysema are expected postoperative findings.
4
77

Jun 11
詳細はこちら。
👉Seven- to 10-year outcome of decompressive surgery for degenerative lumbar spinal stenosis
🔗journals.lww.com/spinejourna…
1
1
41

Jun 10
🍄 Mushroom cap sign.
Represents transcalvarial brain herniation through a craniectomy/skull defect, producing a characteristic mushroom-shaped appearance on CT. Most commonly seen after decompressive craniectomy for severe cerebral edema, trauma, or malignant infarction.
2
234

Tracheostomy post-craniectomy skull defect (sunken flap). The scalp contour strongly suggests previous decompressive craniectomy. 🔍🧠


81
Tracheostomy post-craniectomy skull defect (sunken flap). The scalp contour strongly suggests previous decompressive craniectomy. 🔍🧠
1
82

🧠Intracranial pressure management is not “give mannitol and hyperventilate.”
It is a structured prevention of secondary brain injury.
Recent PubMed indexed literature reinforces a tiered approach: protect oxygenation, ventilation, venous drainage, perfusion pressure, temperature, sodium, seizures, sedation, and then escalate to hyperosmolar therapy, CSF drainage, surgery, and advanced multimodal monitoring when needed (Viarasilpa et al., 2024).
First principles matter. Head elevation 30 to 45°, neutral neck position, avoidance of hypoxia, hypotension, fever, seizures, hyponatremia, excessive suctioning, coughing, and ventilator dyssynchrony may be as important as rescue osmotherapy.
Hyperosmolar therapy remains central. Common rescue doses include mannitol 20 percent at 0.5 to 1 g/kg/DOSE IV over 5 to 15 minutes, or hypertonic saline such as 3% NaCl 150 mL over 10 to 30 minutes, or 23.4% NaCl 30 to 60 mL in selected severe crises (Viarasilpa et al., 2024). A 2024 meta analysis found that hypertonic saline and mannitol both reduce ICP, with similar mortality and neurological outcomes, although hypertonic saline may have longer effect duration and shorter ICU stay (Karamian et al., 2024).
Ventilation must protect both lung and brain. Avoid hypoxemia and severe hypercapnia. PaCO₂ around 35 to 38 mmHg is often targeted during ICP crisis; BRIEF hyperventilation may be a bridge in impending herniation, not a chronic strategy (Viarasilpa et al., 2024).
Hemodynamics are brain therapy. CPP is usually targeted around 60 to 70 mmHg in severe TBI, but newer data support individualized CPP guided by autoregulation and multimodal monitoring when available (Bögli et al., 2025).
Refer urgently to neurosurgery when there is mass lesion, hematoma, hydrocephalus, refractory ICP, herniation syndrome, deteriorating pupils, or need for EVD or decompressive surgery.
Always ask yourself, is the brain perfused, oxygenated, decompressed, electrically controlled, and still salvageable?
#ICU #NeurocriticalCare #TBI #IntracranialPressure #CPP #HypertonicSaline #Mannitol #MechanicalVentilation #Neurosurgery #CriticalCareReferences
Bögli, S. Y., Donnelly, J., Ercole, A., et al. (2025). Cerebral perfusion pressure targets after traumatic brain injury: A reappraisal. Critical Care, 29, 192. doi.org/10.1186/s13054-025-0…
Karamian, A., Seifi, A., & Lucke-Wold, B. (2024). Comparing the effects of mannitol and hypertonic saline in severe traumatic brain injury patients with elevated intracranial pressure: A systematic review and meta-analysis. Neurological Research, 46(9), 883–892. doi.org/10.1080/01616412.202…
Viarasilpa, T., Mayer, S. A., & Francoeur, C. L. (2024). Managing intracranial pressure crisis. Current Neurology and Neuroscience Reports, 24, 873–883. doi.org/10.1007/s11910-024-0…
1
12
34
1,471


Jun 9
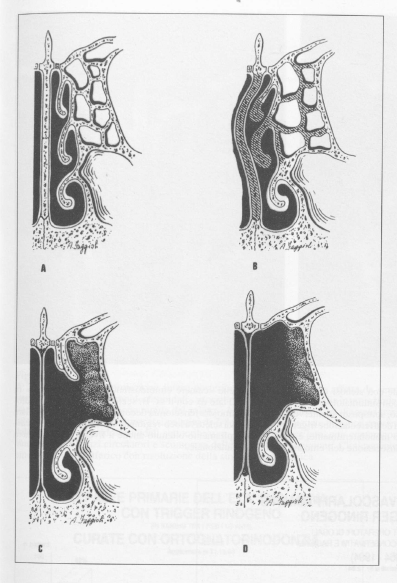
"Functional" neurovascular decompressive surgery of cranial rhino- base in headaches with rhinogenic triggering eurekamag.com/research/045/0…
Acta Otorhinolaryngologica Italica 16(3): 254-260
1996
ISSN/ISBN: 0392-100X
PMID: 9027202
10
Dr Celestino Gutiérrez González MD 🇪🇸🍏🇻🇪 retweeted
📢 Study Spotlight: Decompressive colonoscopy may be the more effective first-line intervention for ACPO after failed supportive therapy: gastroendonews.com/a/SjgBAA/… #colonoscopy #gastroenterology

4
8
506
Dr Ihab Suliman retweeted

Jun 9
Head injury with decompressive craniotomy tracheostomy
1
1
2,871

Osawele Emmanuel retweeted

SURGICAL ROOM SEASON 1 • EPISODE 5: Decompressive Craniectomy and Haematoma Evacuation
1
3
18

Jun 7
สัญญาณโรคกระดูกสันหลัง แบบไหนควรผ่าตัด? เปิดเทคนิคผ่าแผลเล็ก ลดเจ็บ
.
โรคกระดูกสันหลัง เป็นปัญหาสุขภาพที่ส่งผลกระทบต่อคุณภาพชีวิตอย่างมาก แต่ยังมีผู้ป่วยจำนวนไม่น้อยที่กังวลเกี่ยวกับการผ่าตัด เนื่องจากเชื่อว่าอาจเกิดภาวะแทรกซ้อน เจ็บปวด เสี่ยงต่ออัมพาต หรือใช้เวลาฟื้นตัวนาน ซึ่งในปัจจุบัน ด้วยเทคโนโลยีทางการแพทย์ที่มีการพัฒนาอย่างต่อเนื่อง การผ่าตัดโรคกระดูกสันหลังจึงมีเทคนิคและเครื่องมือใหม่ ๆ ที่ทำให้การผ่าตัดมีความปลอดภัย และไม่ได้น่ากลัวอย่างในอดีต
.
ประเภท และเทคนิคการผ่าตัดกระดูกสันหลัง
.
การผ่าตัดแบบดั้งเดิม (Open Surgery) เป็นการผ่าตัดเปิดแผลขนาดใหญ่ แพทย์จะมองเห็นรอยโรคชัดเจน มีการเข้าถึงกระดูกสันหลังโดยตรง เหมาะกับโรคที่มีความซับซ้อน เช่น กระดูกสันหลังคดหรือโก่งมาก
.
การผ่าตัดแบบแผลเล็ก (Minimally Invasive Spine Surgery: MISS) ใช้เทคโนโลยีการผ่าตัดผ่านกล้อง ทั้งนี้ การผ่าตัดแผลเล็กผ่านกล้องยังมีการใช้เครื่องมือที่แยกย่อยลงไป เช่น
📷การผ่าตัดหมอนรองกระดูกสันหลังแบบใช้กล้องจุลทรรศน์ (Microscopic Lumbar Microdiscectomy) เพื่อการขยายภาพบริเวณที่ทำการผ่าตัด เหมาะกับผู้ป่วยหมอนรองกระดูกทับเส้นประสาท หรือโพรงประสาทตีบแคบ
📷การผ่าตัดหมอนรองกระดูกทับเส้นประสาทด้วยวิธีส่องกล้อง (Full-Endoscopic Lumbar Discectomy: FED) โดยใช้กล้องเอนโดสโคป จึงให้แผลขนาดเล็กเพียง 5-1 ซม. ช่วยลดการบาดเจ็บของเนื้อเยื่อข้างเคียงได้ดี
📷การผ่าตัดเชื่อมข้อกระดูกสันหลัง (Spinal Fusion) เพื่อเพิ่มความมั่นคงในผู้ป่วยที่มีภาวะกระดูกสันหลังเคลื่อน หรือหมอนรองกระดูกและข้อกระดูกสันหลังเสื่อม ซึ่งทำได้ในหลายเทคนิค เช่น การผ่าตัดเชื่อมข้อทางด้านหลังแบบแผลเล็ก (MIS TLIF) เชื่อมข้อทางด้านข้าง (OLIF) และเชื่อมข้อทางด้านหน้า (ALIF)
.
การผ่าตัดขยายโพรงเส้นประสาท (Decompressive Laminectomy) เป็นการตัดกระดูกหรือเนื้อเยื่อที่กดทับเส้นประสาทออก เพื่อบรรเทาอาการปวดหรืออ่อนแรง
.
การผ่าตัดใส่โลหะยึดตรึงกระดูก (Percutaneous Screw Fixation) ด้วยการใส่สกรูหรืออุปกรณ์โลหะผ่านแผลเล็กเพื่อยึดตรึงกระดูกสันหลังให้มั่นคง
.
การฉีดซีเมนต์เสริมกระดูก (Percutaneous Vertebral Augmentation) เพื่อเพิ่มความแข็งแรงของกระดูกสันหลังที่ยุบหรือหักจากภาวะกระดูกพรุน
.
อ่านต่อ : pptv36.news/1WNC
.
#ผ่าตัดกระดูกสันหลัง #โรงพยาบาลพญาไทพหลโยธิน #BDMS #yourtrustedhealthcarenetwork #เรื่องสุขภาพเราเชี่ยวชาญ #HealthBringsWealth #สุขภาพดีคือสมบัติที่ล้ำค่า #StayFitbyBDMS

1
6
976