
luiza retweeted

16h
Nada que você precise mendigar é digno de estar na sua vida
71
64
5,468

The predictions made by this blogger about the market are remarkably precise.
La cripta de Corvus retweeted

💜🔨 Floral Judgment
Yuni lunges forward with a powerful thrust from her Petunia Hammer.
Steady, precise, and devastating —
judgment delivered in a single strike.
#GardenSouls #IndieGame #GameDev #Roguelite #インディーゲーム #ゲーム開発 #ローグライト #独立游戏 #游戏开发
2
5
30
387

Um, isn't the precise goal to 'change how children access and experience the digital world'???

This announcement reflects legitimate concerns about children's safety online, but a ban of this scale would change how children access and experience the digital world. The UK Government must ensure that any decisions are informed by children themselves and by independent experts.
We are concerned that a blanket ban may look protective on paper, but instead pushes children into less regulated spaces, where they are less likely to seek help when something goes wrong. Children growing up in poverty are likely to be among those most affected.
If ministers want to make the online world safer, the answer is not simply keeping children off platforms. The focus must be on providing better support for parents by making platforms safer by design, tackling addictive and high-risk features such as stranger contact, live streaming, nudification tools and unsafe AI systems, so that children are not exposed to harm online.


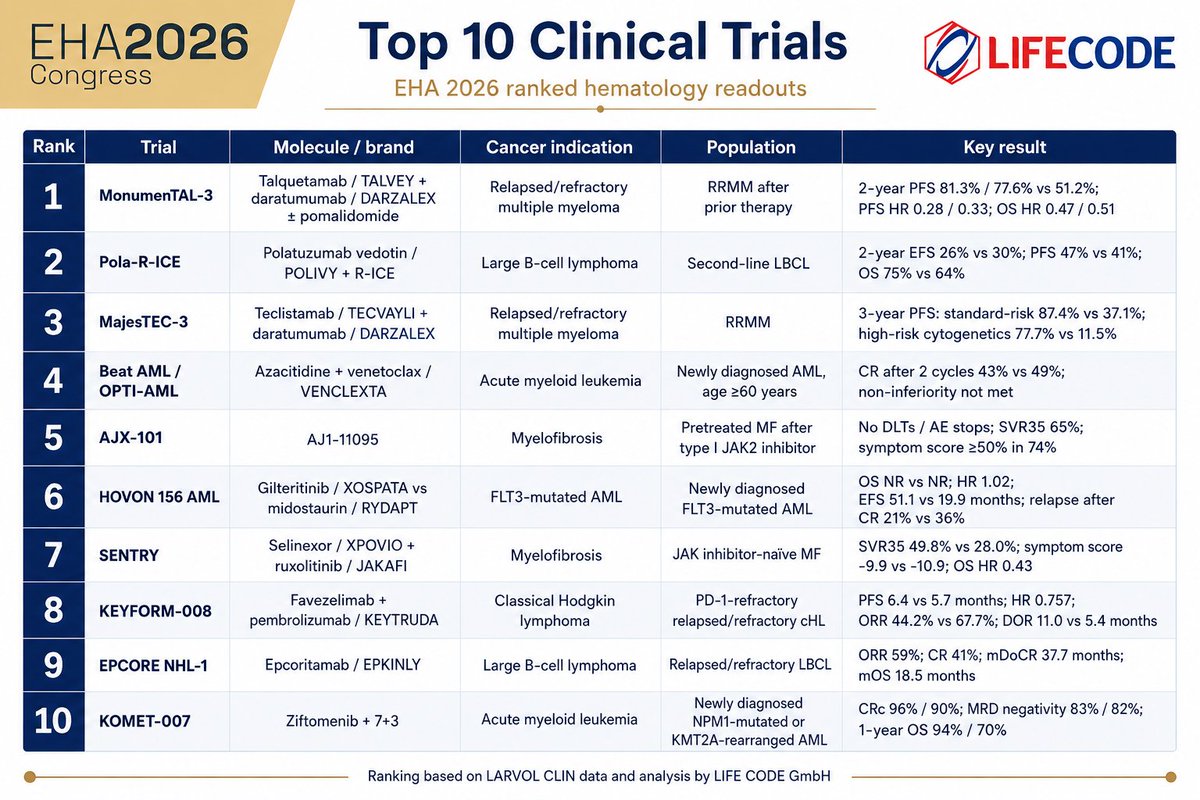
#EHA2026 @EHA_Hematology has just wrapped up in Stockholm. The congress delivered a strong set of hematology readouts across multiple myeloma, lymphoma, myelofibrosis and acute myeloid leukemia.
I used @LARVOL CLIN data to identify the ten most exciting trial results discussed by oncologists on X. Here they are:
MonumenTAL-3: talquetamab plus daratumumab in relapsed/refractory multiple myeloma
MonumenTAL-3 was arguably the most important multiple myeloma readout at EHA 2026. Talquetamab plus daratumumab, with or without pomalidomide, was tested in relapsed/refractory multiple myeloma and showed a strong benefit versus daratumumab, pomalidomide and dexamethasone.
Two-year progression-free survival was 81.3% with talquetamab, daratumumab and pomalidomide, 77.6% with talquetamab and daratumumab, and 51.2% in the control arm. The PFS hazard ratios were 0.28 and 0.33 respectively. Overall survival also favoured the talquetamab-containing arms, with OS hazard ratios of 0.47 and 0.51.
The strategic message is clear: GPRC5D-directed bispecific therapy is moving earlier in the myeloma pathway. This raises important sequencing questions against BCMA-directed bispecifics, CAR-T therapy and other emerging combinations.
Pola-R-ICE: polatuzumab vedotin in second-line large B-cell lymphoma
Pola-R-ICE tested whether adding polatuzumab vedotin to R-ICE could improve outcomes in second-line large B-cell lymphoma.
The all-comer result was not a clean win. At two years, event-free survival was 26% with Pola-R-ICE versus 30% with R-ICE. However, progression-free survival was 47% versus 41%, and overall survival was 75% versus 64%.
This is the kind of readout where the headline does not tell the whole story. The trial does not establish a broad new standard for all patients, but the PFS and OS signal may remain relevant in selected patient groups. From a forecasting perspective, the key issue will be whether any subgroup signal is strong enough to influence real-world treatment behaviour.
MajesTEC-3: TECVAYLI plus DARZALEX in relapsed/refractory multiple myeloma
MajesTEC-3 delivered one of the clearest efficacy signals in relapsed/refractory multiple myeloma.
Teclistamab plus daratumumab produced a striking three-year PFS benefit versus standard daratumumab-based regimens. In standard-risk patients, three-year PFS was 87.4% versus 37.1%. In patients with high-risk cytogenetics, three-year PFS was 77.7% versus 11.5%.
This is a very strong signal for moving BCMA-directed bispecific therapy earlier in the myeloma pathway. The clinical question is increasingly shifting from “does it work?” to “how should we sequence it?” Infection management, outpatient feasibility and competition with CAR-T therapy will be central to will be central to adoption.
Beat AML / OPTI-AML: venetoclax duration in newly diagnosed AML
Beat AML / OPTI-AML addressed a highly practical question in older patients with newly diagnosed AML: can venetoclax exposure be shortened from 28 days to 14 days when combined with azacitidine?
The answer was not straightforward. Complete remission after two cycles was 43% with the 14-day venetoclax schedule versus 49% with the 28-day schedule. Non-inferiority was not met.
This matters because venetoclax-based AML therapy is widely used, and schedule optimization has major implications for cytopenias, infections, hospital burden and quality of life. The trial suggests that shortening therapy may be attractive in practice, but should not be assumed to preserve efficacy across all patients.
AJX-101: type II JAK2 inhibition in pretreated myelofibrosis
AJX-101 is an early but important signal in myelofibrosis. AJ1-11095 is a first-in-class type II JAK2 inhibitor being evaluated in patients previously treated with type I JAK2 inhibitors.
The EHA data showed no dose-limiting toxicities or adverse event-related discontinuations. Spleen volume reduction of at least 35% was seen in 65% of patients, while symptom score improvement of at least 50% was reported in 74%.
These are still early-phase data, but the mechanism is strategically interesting. The programme aims to address incomplete pathway suppression after conventional JAK inhibition. Durability, anemia effects and randomized validation will be crucial, but this is clearly a programme to watch.
HOVON 156 AML: gilteritinib versus midostaurin in frontline FLT3-mutated AML
HOVON 156 AML compared gilteritinib with midostaurin in newly diagnosed FLT3-mutated AML eligible for intensive therapy.
The trial missed its primary overall survival endpoint. Median OS was not reached in either arm, with a hazard ratio of 1.02. Event-free survival was 51.1 months versus 19.9 months, while complete remission was 79% versus 83%. Relapse after complete remission was lower with gilteritinib, at 21% versus 36%.
The result is strategically important because gilteritinib is a highly active later-line FLT3 inhibitor. However, superiority over midostaurin in frontline intensive therapy was not demonstrated. This reinforces how difficult it can be to replace an established standard, even with a mechanistically attractive next-generation agent.
SENTRY: selinexor plus ruxolitinib in JAK inhibitor-naïve myelofibrosis
SENTRY tested selinexor plus ruxolitinib in JAK inhibitor-naïve myelofibrosis.
The combination significantly improved spleen volume reduction. SVR35 was 49.8% with selinexor plus ruxolitinib versus 28.0% with ruxolitinib alone. The overall survival hazard ratio was 0.43. However, the symptom score result was less convincing, with -9.9 versus -10.9.
This is a classic myelofibrosis development dilemma: a strong spleen signal, but a more complicated positioning question if symptom improvement is not clearly differentiated. The commercial narrative will depend on whether longer follow-up can support a broader disease-modification argument.
KEYFORM-008: favezelimab plus pembrolizumab in PD-1-refractory Hodgkin lymphoma
KEYFORM-008 evaluated favezelimab plus pembrolizumab versus chemotherapy in relapsed/refractory classical Hodgkin lymphoma after PD-1 exposure.
The combination improved PFS numerically, with median PFS of 6.4 versus 5.7 months and a hazard ratio of 0.757. ORR was lower than chemotherapy, at 44.2% versus 67.7%, but duration of response was longer, at 11.0 versus 5.4 months.
Scientifically, this is an interesting signal for LAG-3 plus PD-1 biology after PD-1 failure. Commercially, the result is less straightforward. A modest PFS difference, lower response rate and programme-level development decisions all complicate the read-through.
EPCORE NHL-1: EPKINLY in relapsed/refractory large B-cell lymphoma
EPCORE NHL-1 added another important data point for epcoritamab in relapsed/refractory large B-cell lymphoma.
The trial showed an objective response rate of 59%, a complete response rate of 41%, median duration of complete response of 37.7 months, and median overall survival of 18.5 months.
These are meaningful data in a heavily pretreated lymphoma population. The key strategic point is that CD3xCD20 bispecific antibodies are now firmly established as part of the lymphoma innovation landscape. The next phase will be about combinations, earlier-line use, treatment duration and differentiation versus CAR-T therapy.
KOMET-007: ziftomenib plus 7 3 in newly diagnosed AML
KOMET-007 delivered striking early data for ziftomenib combined with intensive 7 3 chemotherapy in newly diagnosed AML with NPM1 mutation or KMT2A rearrangement.
Composite complete remission rates were 96% in NPM1-mutated AML and 90% in KMT2A-rearranged AML. MRD negativity was 83% and 82% respectively. One-year overall survival was 94% in NPM1-mutated AML and 70% in KMT2A-rearranged AML.
This is still early, non-randomized data, but the signal is impressive. Menin inhibitors are becoming one of the most interesting targeted therapy classes in AML, particularly in molecularly defined populations. The next question is whether randomized phase 3 data can confirm the magnitude and durability of benefit.
Several patterns stand out.
First, EHA 2026 reinforced the continued movement of highly active therapies into earlier treatment settings. This was particularly visible in multiple myeloma, where both MonumenTAL-3 and MajesTEC-3 point to earlier use of bispecific antibody combinations.
Second, sequencing is becoming one of the central strategic questions in hematology. In myeloma and lymphoma, clinicians increasingly have to choose between bispecific antibodies, CAR-T therapy, antibody-drug conjugates and established targeted combinations. The forecast is therefore no longer only about market share within a line of therapy, but about treatment order, eligibility, logistics and duration.
Third, AML is becoming more molecularly defined. HOVON 156, Beat AML / OPTI-AML and KOMET-007 all show different aspects of this evolution: targeted FLT3 inhibition, optimization of venetoclax-based therapy, and the emerging role of menin inhibition in NPM1-mutated and KMT2A-rearranged AML.
Fourth, myelofibrosis remains a field where spleen response, symptom benefit, anemia, survival and disease modification all need to be balanced carefully. AJX-101 and SENTRY both produced interesting signals, but both will need further validation before their full commercial relevance becomes clear.
Overall, EHA 2026 showed a hematology landscape that is becoming more precise, more competitive and more complex.
The strategic question is no longer simply whether a drug works. It is where it fits, how early it can move, how it sequences with adjacent modalities, and whether the clinical signal is strong enough to change real-world treatment behaviour.
That is where forecasting becomes difficult — and interesting.
© Robert F. Siegmund, PhD MBA | Life Code GmbH
I deliver strategic insights and product forecasting models to biopharma companies. Reach out to me!
1
3


The Khokhly burned down the drone workshop on Dovzhenko
To be more precise, we burned it down, and Ukrainian journalists kindly provided objective monitoring.
In the photo of the ruins of the Dovzhenko film studio, a shelf with wings for the FP-2 drone is clearly visible. Interesting decorations they have there.
Bravo to the intelligence service! A medal to the agents!


1
25

Swords were mostly used by upper caste kshtriyas, now we're becoming a progressive country (Bhim republic to be precise) so army will Carry on lower caste tradition of carrying Lathi (Making everyone sanghi lathait).
1
2

1. Labeling book value as confusing is an interesting idea, congratulations on refuting the history of investment.
2. What is bullshit? Be precise.
3. Where did I label anything "good or bad"?
4. What metric do you propose for assessing the common equity ownership of the Bitcoin stack?
4. Saylor acknowledges CEBE implicitly in many ways now. Why would he engage with "bullshit" as you term it?
2
5

Nothing proves it harder that you don't know jack shit than spamming me with some boomer Facebook post.
It's not like you know anything about these individual items, or how precise the item is represented.
1
1
6

Vice President Vance says the Iran deal was signed digitally on Sunday, though precise details are not known.
Follow live updates: cnn.it/4em2FPM

418
224
1,158
302,543

GoBull trading insight
Spain to Finish Last in Group H at 2026 World Cup?
My trading view: World Cup group stage results depend on draw luck, in-game performance, and other variables, making precise prediction difficult. Fundamentl asset. gobull.ai/feed?tab=signals #GoBull
19
Mayank Mishra retweeted

- This married woman met her former school friend on 8 February,Propose Day, to be precise. She went with him to a hotel room, where they had sex.
- When the man later began extorting her, she filed the usual “Sherni” complaint, claiming he had spiked her drink and so on.
- She is clearly a drug addict too,just look at the conversation, where she casually says “ladne ki aadat hai na.” This was no innocent encounter; it was an affair. There is no way they will abandon their cash cow.
- Are Hindu men so doomed that they will still accept such women?

Wife of an Armed Force was drugged, gang-raped, filmed by Ayyaz Taj Madare and Ameen Shaikh on the pretext of land deal in Nagpur.
Blackmailed, extorted lakhs, forced to drink Halal liquid, chant Islamic verses, converted by Hazrat Maulana in Chhindwara, MP, "nikah" to Ayyaz and forced to eat Gau-mans!
Two arrested, Maulana absconding. Husband filed FIR.
31
149
1,191
80,254

Let me share and anecdote.
Last week I bought Claude premium then I decided to cancel and ask for a refund. I thought it was weird to send an email to them as per instructions, I was like I doubt they will respond. Well I did and in one minute I got an email back from the FIN agent, professional, precise, fast. I was like wtf. This is the future. Anthropic should just sell this to everyone instead of their sub...
Well today I found out FIN is actually a separate company and @Benioff is buying them. I went and bought more $CRM stock.
6


Porque talvez, eu nunca deixei de sentir.
E talvez, vc seja sim essa pessoa
E talvez, só talvez, ninguém precise complicar nada ao nosso redor dessa vez.
3

Não que você precise saber da minha vida pessoal, mas eu estou de férias do meu trampo, afinal trabalhei mais de 2 anos de segunda a sexta sem férias, ela também trabalha btw, diferente de ti que pelo visto só sabe comer e ganhar peso e ficar falando groselha sobre One Piece na
1
6

discussion for emphasis—it's understandable shorthand. More precise charges could also include actual bodily harm (ABH), common assault, robbery/theft (for the equipment), or public order offences like violent disorder if the threshold for a larger disturbance is met. 2/
2
