
Decades of prayers (miracles happened / witnesses) vs a MF prostatic patin un P raciste et très negrophobe aiguillé 15 aveugles soumis à un texte qui commence « WTP » pfff
1
20

Men often turn to herbal remedies to manage lower urinary tract symptoms (LUTS) linked to benign prostatic hyperplasia (BPH), often without discussion with a clinician. A review of the evidence suggests that while some plant-based medicines may offer modest symptom relief, their benefits are inconsistent, and important questions about their effectiveness persist. mdsc.pe/43t365R

1
2
7
759
DrNadaSalma⚕ retweeted

May 19
1️⃣5️⃣Urology (benign prostatic hyperplasia)
🧡Quick Overview of BPH
🧡Medications from A-Z
💎Brands pictures
💎MOA
💎Doses
💎Labeled and off label uses
💎Counselling points
💎AEs
💎CIs
💎Special populations
💎Storage
👏🏻👏🏻😍😍
1
1
212

First, look for root causes leading to chronic prostatitis such as persistent infections, sitting for long periods of time day after day, and riding a bike for an extended duration (30 miles). If symptoms are alleviated by taking NSAIDs, that is an inexpensive way to quickly tell. Obviously, NSAIDs are not a long-term solution. Also, if you have BPH and are taking decongestants or consuming too much alcohol, these too can cause an inflammatory reaction with increased pain while urinating. Scroll further below for more on the negative effects of pseudoephedrine on the prostate.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Inflammation-Driven Pathway (per Grok):
Chronic inflammation in the prostate can create an environment that promotes cellular changes potentially leading to cancer over time:
Persistent inflammation and oxidative stress: Ongoing inflammation (from unresolved infection, immune response, pelvic floor issues, or other triggers) leads to repeated production of reactive oxygen species (free radicals). These cause DNA damage, mutations, and cell turnover.
Proliferative Inflammatory Atrophy (PIA): This is a key intermediate lesion. PIA involves atrophic (shrunken) prostate glands with high cell proliferation amid inflammation. It is frequently found near areas of prostate cancer and is considered by some researchers a possible "precursor" or risk lesion where damaged cells may progress to high-grade prostatic intraepithelial neoplasia (HGPIN) and eventually adenocarcinoma.
Molecular pathways: Inflammation activates signaling like NF-κB, which promotes cell survival, proliferation, angiogenesis (new blood vessels for tumors), and inhibits apoptosis (programmed cell death). Cytokines (e.g., IL-6) and immune cells (macrophages, T-cells) can further drive this pro-cancer environment.
Immune dysregulation: Shifts in T-cells (e.g., Th17, Treg imbalance) and other immune responses seen in chronic prostatitis may contribute to a tumor-friendly microenvironment.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Pseudoephedrine (per Grok): Found in a combination cold/allergy meds is a sympathomimetic decongestant that primarily stimulates alpha-adrenergic receptors. This helps shrink nasal blood vessels to reduce congestion, but it has notable effects on the prostate and urinary tract, especially in men with prostate issues.
Main Impact on the Prostate: Tightens smooth muscle in the prostate, bladder neck, and urethra: This increases resistance to urine flow (bladder outlet obstruction). It can worsen lower urinary tract symptoms (LUTS) such as: Difficulty starting urination (hesitancy), Weak urine stream, Incomplete bladder emptying, and Frequent or urgent urination.
In severe cases, acute urinary retention (inability to urinate, which may require catheterization).
Particularly problematic in Benign Prostatic Hyperplasia (BPH/enlarged prostate): Many sources strongly advise men with BPH to avoid pseudoephedrine because it can "swell" or constrict the prostate area and push borderline symptoms into a crisis. Symptoms often improve after stopping the drug.
Age factor: Effects tend to be more pronounced in men over 50, even if they have no prior urinary symptoms. Studies show increases in International Prostate Symptom Score (IPSS) and post-void residual urine volume after use.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Anecdotal:
Five years ago, my T-Levels dropped considerably. I tried T injections and my PSA score nearly doubled in 6-months and put me over a “4” which is the proverbial line. I immediately stopped the injections. My urologist convinced me to get an MRI and a prostate biopsy (which I personally do not recommend and will never do again).
My MRI was negative, but a single biopsy (out of 14) showed some irregular cells. My advice: do the MRI with contrast first. If there is no visible mass, then stop! Puncturing the prostate up to 16x is like looking for a needle in a haystack, and it is not healthy. You can bleed for up to two weeks. God only knows what this procedure does to the prostate. Also, there is nothing doctors can do, including focal therapy, until there is a “mass” large enough to target. And lastly, all modern medicine wants to do is treat "symptoms" instead of root causes. We all know the profit motive at play here. For now, get into "surveillance mode" with quarterly PSA screenings and an annual MRI with contrast.
The most important thing you can do today is to stop sitting for prolonged periods, reduce alcohol along with acidic foods and drinks, and transition to a diet that is rich in anti-inflammatory foods, roots, herbs, and nutraceuticals.
Over the past 9 months, I have tried the Ivermectin/Mebendazole protocol developed by The Wellness Company. The good news is that my PSA score stabilized (at 6.2) and has not risen during this time. Right now, there's just no way to clinically determine cause and effect. I am going to try a higher dosage to see if it will lower my score. Ivermectin has powerful anti-inflammatory properties, and I will continue to use it until clinically proven otherwise.
Another anecdotal piece of evidence that I found helpful was traction and cold therapy - especially in the lumbar region. I use a combination of lower back stretches, inversion table, and a lumbar traction device along with a flexible ice pack. Before you spend the money, fill a 1qt. freezer bag with ice, lay flat and place the ice in the area of L1 and L2. Try to tolerate it for up to 15 minutes or until the area is numb. Do this up to 3x in a day. If there is any type of nerve impingement affecting the prostate, you will get short term pain relief and a much stronger urine flow. Then consider adding devices and/or chiropractic treatment to your therapy regimen. Also, the cold will reduce swelling in prostate and that alone will provide temporary relief. This is another area where cause and affect are difficult to clinically prove.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Key Details on Prostate Innervation (per Grok):
Sympathetic innervation (controls smooth muscle contraction, e.g., during ejaculation): Originates from the thoracolumbar spinal cord, specifically the last few thoracic segments (often T11–T12) and upper lumbar segments (L1–L2). Preganglionic fibers exit the spinal cord at these levels, travel via the sympathetic chain and lumbar splanchnic nerves, and converge in the superior hypogastric plexus. They then continue as hypogastric nerves to the inferior hypogastric plexus (pelvic plexus), which directly supplies the prostate.
That's all for now.
14
Davis retweeted

14h
Tadalafil isn't just for ED 💯
Major use: Benign Prostatic Hyperplasia (BPH) - relieves urinary symptoms like frequent urges & weak flow. (Also approved for Pulmonary Arterial Hypertension).
One pill, multiple wins 🔥💯
1
1
6
818


Tadalafil 20 mg (the active ingredient found in medications like Cialis). Tadalafil is a prescription medication primarily used to treat erectile dysfunction (ED) and symptoms of benign prostatic hyperplasia (enlarged prostate).
1
56

They don’t know exactly why but it helps with non-prostatic bladder problems as well.
1
11

Jun 13
A Short Term Act That Creates Long Term Benefits. 📈 Temporary Prostatic Urethra Expander for BPH/LUTS Shows Durable Results. 🇺🇸
.
.
medpagetoday.com/meetingcove… #urology #urologyxy #BPH #continence #incontinence #menshealth #prostate TkU @medpagetoday for sharing.
1
31

Jun 13
9. Beyond Erectile Dysfunction
Tadalafil is also prescribed for:
1. Benign prostatic hyperplasia (BPH)
2. Pulmonary arterial hypertension (under different dosing and brand names)
Because it relaxes smooth muscle and improves blood flow in different parts of the body.
1
2
2,741
👊🏻 me retweeted

6 Sep 2024
Adams favorite way to cum. The orgasm induced through deep prostatic massage is thought to be different from direct penile stimulation. Although penile stimulation orgasms are associated with 4–8 pelvic muscle contractions, prostatic massage orgasms are associated with 12 contractions. Prostatic massage orgasms are thought to be more intense and diffuse than penile stimulation orgasms, but they require time and practice @Adamscunt

2
103
915
123,423

Jun 13
POST VOID URINE
1/22 Post-void residual (PVR) urine is the volume remaining in the bladder immediately after micturition. It is a marker of bladder emptying efficiency, not a diagnosis.
2/22 Elevated PVR occurs when the bladder cannot empty adequately. Mechanisms: 1) outlet obstruction, 2) impaired detrusor contractility, 3) neurologic dysfunction, 4) functional causes.
3/22 Bladder outlet obstruction causes:
• BPH
• Urethral stricture
• Bladder neck obstruction
• Prostate cancer
• Large bladder stone
• Pelvic organ prolapse
4/22 Detrusor underactivity causes:
• Aging bladder
• Diabetic cystopathy
• Chronic overdistension
• Postoperative retention
• Long-standing obstruction
• Idiopathic detrusor failure
5/22 Neurogenic causes:
• Spinal cord injury
• Cauda equina syndrome
• Multiple sclerosis
• Parkinson disease
• Stroke
• Diabetic autonomic neuropathy
6/22 Drug-induced retention causes:
• Anticholinergics
• Antihistamines
• Tricyclic antidepressants
• Antipsychotics
• Opioids
• Sympathomimetics
7/22 Typical presentation:
• Weak stream
• Hesitancy
• Straining
• Intermittency
• Incomplete emptying
• Frequency
• Nocturia
• Recurrent UTI
8/22 Severe chronic retention may present with:
• Overflow incontinence
• Bilateral hydronephrosis
• Renal dysfunction
• Recurrent sepsis
• Large painless palpable bladder
9/22 Key differential: BPH.
History:
• Progressive voiding symptoms
• Enlarged prostate on DRE
Investigations:
• PSA
• Uroflowmetry
• PVR
• Ultrasound
10/22 BPH treatment:
• Tamsulosin: α1A blockade → relaxes prostatic smooth muscle.
• Silodosin: highly selective α1A antagonist.
• Alfuzosin: α1 antagonist.
11/22 BPH progression reduction:
• Finasteride: inhibits type II 5α-reductase.
• Dutasteride: inhibits type I and II 5α-reductase.
Effect: ↓ DHT → prostate shrinkage.
12/22 BPH procedures:
• TURP
• Bipolar TURP
• HoLEP
• ThuLEP
• Aquablation
• Simple prostatectomy
Choice depends on gland size and anatomy.
13/22 Urethral stricture clues:
• Thin stream
• Spraying
• Recurrent instrumentation history
Investigations:
• RGU
• MCU
• Cystoscopy
14/22 Urethral stricture treatment:
• Optical internal urethrotomy (OIU)
• Excision and primary anastomosis urethroplasty
• Buccal mucosal graft urethroplasty
Definitive treatment is usually urethroplasty.
15/22 Neurogenic bladder clues:
• Neurologic symptoms
• Diabetes
• Spinal pathology
Investigations:
• MRI spine
• Urodynamics
• EMG when indicated
16/22 Neurogenic retention treatment:
• Clean intermittent catheterization (CIC)
• Suprapubic catheter
• Sacral neuromodulation
• Intradetrusor botulinum toxin in selected dysfunction patterns
17/22 Detrusor underactivity diagnosis requires urodynamics. PVR alone cannot distinguish poor contraction from obstruction.
18/22 Urodynamic findings:
• Low detrusor pressure
• Poor flow
• Large residual volume
These suggest impaired bladder contractility.
19/22 Acute urinary retention is an emergency.
Immediate management:
• Foley catheterization
• Suprapubic cystostomy if urethral access fails
Then investigate the cause.
20/22 Important investigations after finding elevated PVR:
• Urinalysis
• Urine culture
• Serum creatinine
• PSA (when indicated)
• Ultrasound KUB
• Uroflowmetry
• Cystoscopy
• Urodynamics
21/22 Red flags:
• Hydronephrosis
• Rising creatinine
• Recurrent retention
• Recurrent UTI
• Hematuria
• Neurologic deficits
These require expedited workup.
22/22 Clinical pearl: Elevated PVR is not a prostate diagnosis. The same bladder scan finding may represent BPH, urethral stricture, diabetic cystopathy, spinal cord disease, medication effect, or irreversible detrusor failure. The next step is determining which mechanism is responsible.
59

Jun 13
Let’s interject some real facts so we can eliminate “the stupid”
Grok
“The X post claims Biden’s metastatic prostate cancer was a hoax and states he only has BPH (benign prostatic hyperplasia), accompanied by a short video clip of Biden with question marks overlaid.
• In May 2025, Biden’s office announced a diagnosis of aggressive prostate cancer with Gleason score 9 that metastasized to his bones; he has since started hormone therapy and radiation, as reported by medical centers including Michigan Medicine and Stanford.
• Biden had a documented history of BPH treatment years earlier, but this common benign condition can coexist with cancer and does not invalidate the 2025 metastatic diagnosis confirmed across multiple independent sources. “
Jun 6

Metastatic prostrate cancer was a total hoax. Biden has BPH a benign enlarged prostrate. Just another lie 🤥
1
1
284
Chidambara .ML. retweeted

Jun 12
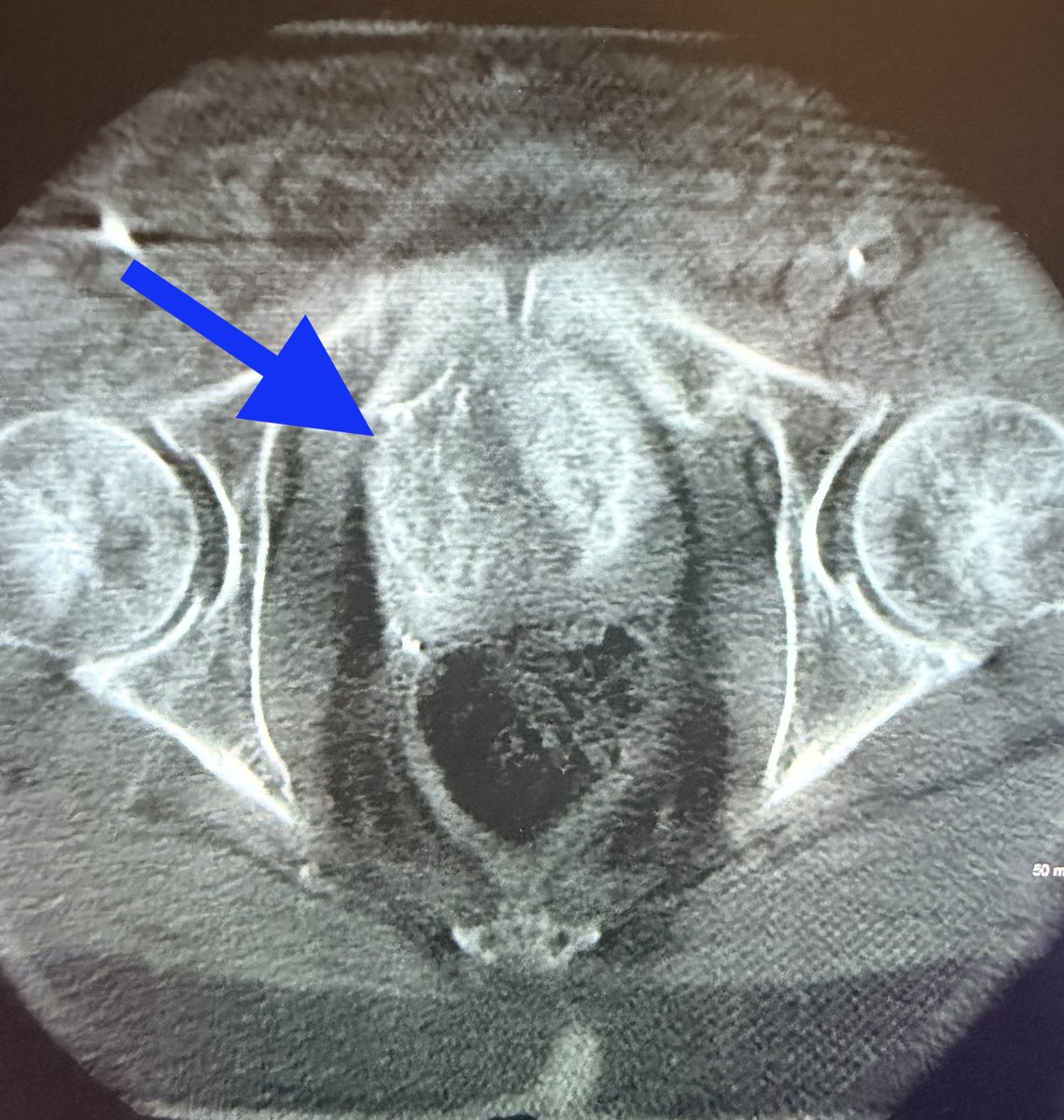
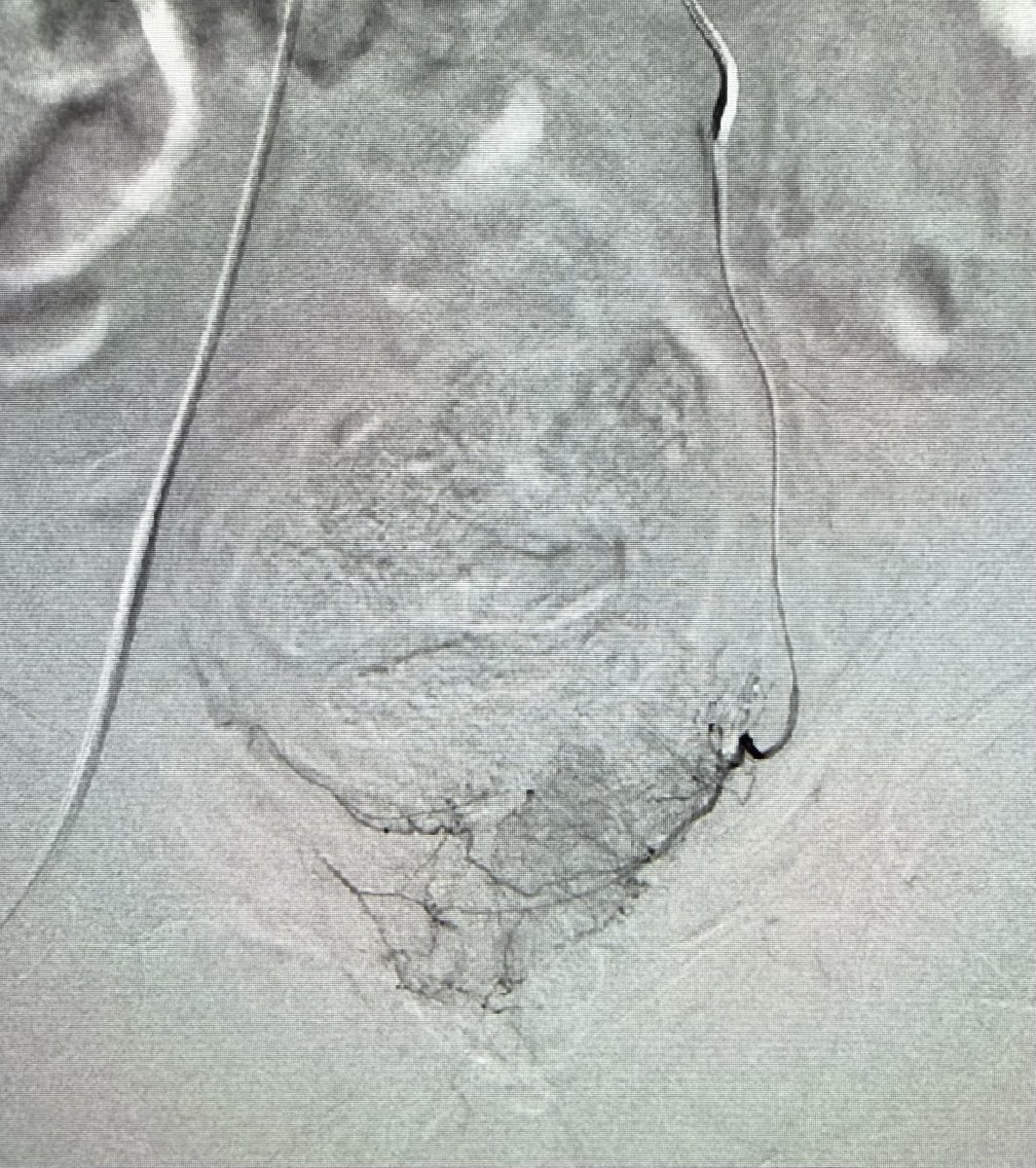
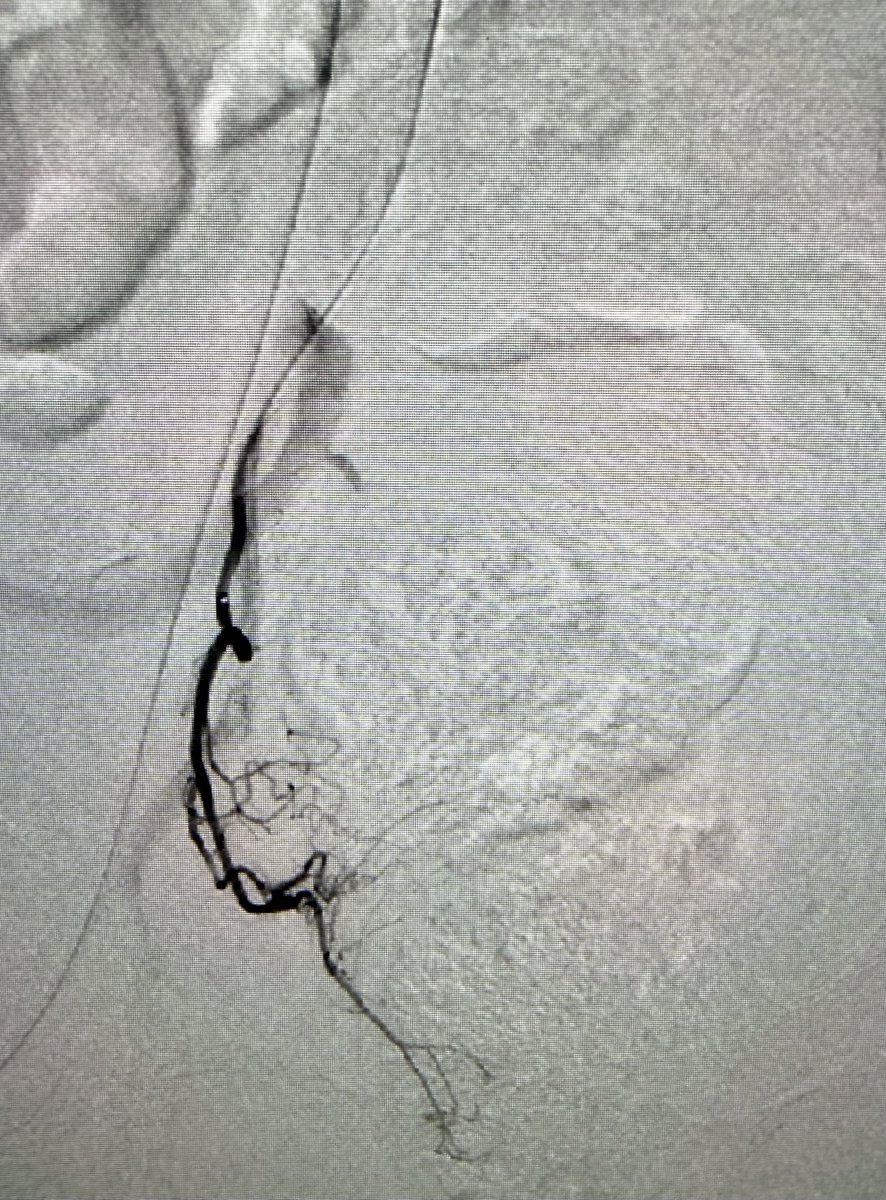
Prostatic artery embolization for symptoms of enlarged prostate. IPSS 28. 45 minute outpatient procedure with minimal down time and high success rates. #iRad

1
1
18
1,299

Answer: TURP 🚻⭐
★ TURP stands for transurethral resection of the prostate ✂️
★ It relieves bladder outlet obstruction from benign prostatic hyperplasia 🚰
★ The resectoscope removes prostatic tissue through the urethra, not an open incision 🔎
★ Common indications include retention, recurrent UTIs, stones, or refractory symptoms 📌
★ Watch for bleeding, retrograde ejaculation, and TUR syndrome after surgery ⚠️
★ Alpha blockers help symptoms, but TURP is the classic procedural answer 🩺
#USMLE #Urology #MedEd
Find more such high-yield points: oncourse.onelink.me/xW0t/ins…
1
1
493

The low 5mg dose is also very effective for prostatic symptoms of urinary frequency, urgency, & nocturia.
It improves sleep with fewer nighttime bathroom trips, & doesn’t have the negative sexual side effects of 5α-reductase blockers, or the hypotension effects of α1 blockers.
1
1
1,302

Jun 12
📣 New Podcast! "Natural Methods for Managing Benign Prostatic Hyperplasia" on @Spreaker #benignprostatichyperplasia #bph #healthawareness #lycopene #menshealth spreaker.com/episode/natural…

6

Jun 12
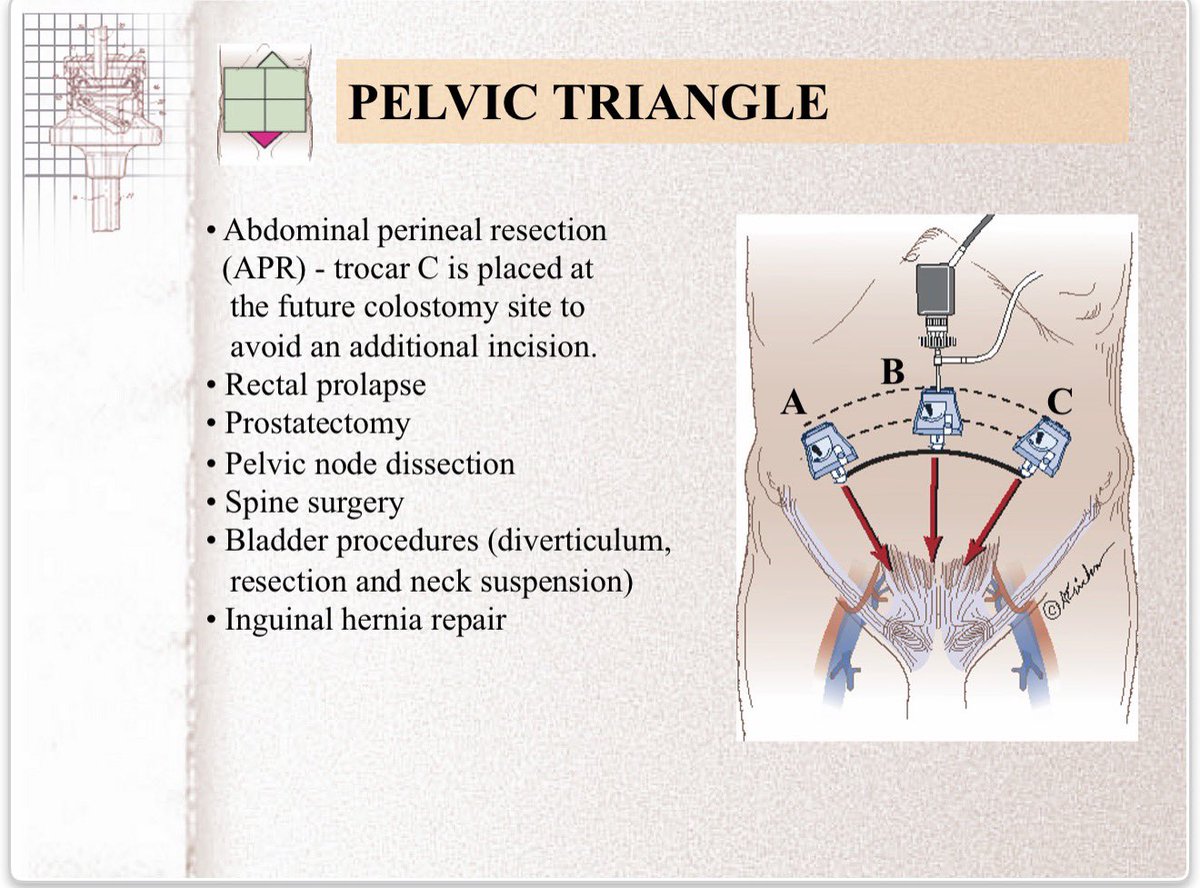
Trocar placement for laparoscopic abdominal procedures: a simple standardized method
George S Ferzli et al. J Am Coll Surg. 2004 Jan;198(1):163-73.
doi: 10.1016/j.jamcollsurg.2003.08.010.
PMID: 14698326
George S Ferzli , Abe Fingerhut
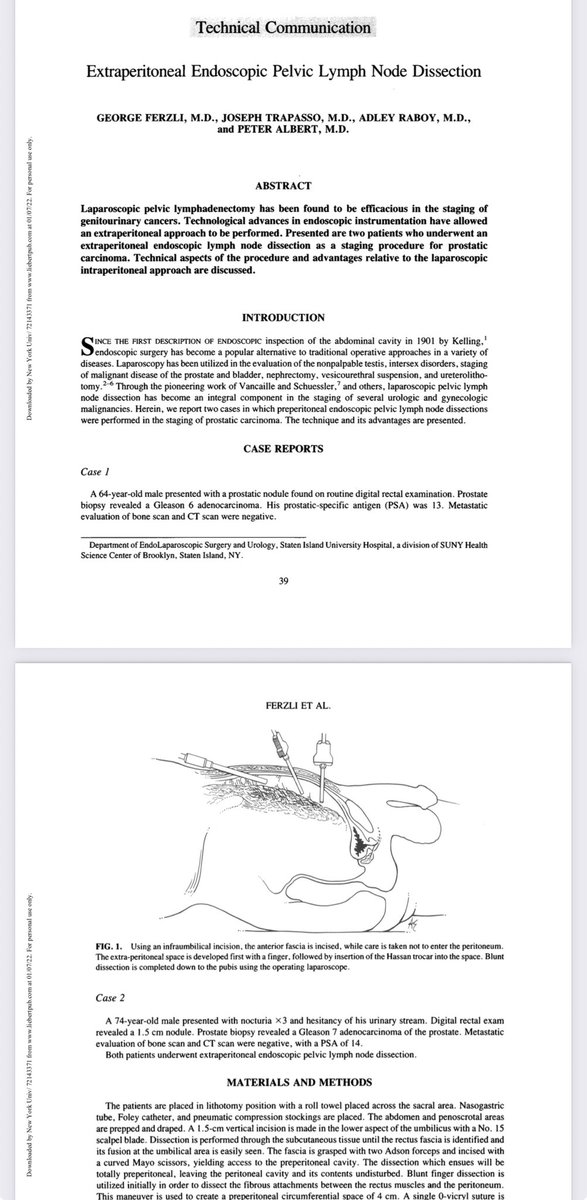
Extraperitoneal endoscopic pelvic lymph node dissection vs. laparoscopic lymph node dissection in the staging of prostatic and bladder carcinoma
G Ferzli et al. J Laparoendosc Surg 1992 Oct;2(5):219-22.
doi: 10.1089/lps.1992.2.219.
G Ferzli 1, A Raboy, D Kleinerman, P Albert
PMID: 1421539
Extraperitoneal endoscopic pelvic lymph node dissection.
Ferzli, G., Trapasso, J., Raboy, A., & Albert, P. (1992). Extraperitoneal endoscopic pelvic lymph node dissection. Journal of laparoendoscopic surgery, 2(1), 39–44. lnkd.in/eHW2jGEn
PMID: 1533548
#LaparoscopicSurgery #RoboticSurgery #GeneralSurgery #SurgicalSafety #MedEd #SurgicalEducation #SurgEd #MISurgery #SoMe4Surgery #urology

17
77
3,591