
Bhai thoda lavdu h kya ? Hard earn money se car khareed te h, ye 🤡 e100 daal dega . Price bhi nhi km hoga overall consumption ka , iss joker ka baat sunna hoga ab 🤡🤡, itna enviroment lover ho toh ev push krke charger lgana chiye tga desh bhar m
3

Someone tell tga to host another giveaway only so I see Mew not getting it for the third time
1
19


Sa mga nagppm lagina mga tga baguio,ayn my stocks na ulit tau!!!!dm sa mga availers natin jn,,
#baguiopoppers
#ilokano
#De_bolitas2600
Old account #dxbwild4u



6

Game of the year não é resumido a quem vendeu mais, é o impacto q o jogo causou na indústria naquele ano. E hogwarts legacy foi completamente esnobado, não concorreu em nenhuma categoria, o TGA fingiu q esse jogo não existia
15


@dojphofficial @pnppio HI PNP PLZ HULIHIN NIO I2NG BASTOS NA LALAKI BABAE BATA AT TGA D2 NANGULO SA TPT NG BHAY NMIN NSA OUTPOST NGPPRNIG SKN NG MSAMA NGGWA DW NG BHAY PUKPOK NG PUKPOK PRA MANGULO D2 NANGW PA D2 PLZ PKHULI D2 PUROK 12 MARTINEZ STREET BRGY COMMONWEALTH QUEZON CITY
8

I'm surprised that this wasn't in Steam's Nextfest. There's so many low effort games in it that you clearly would have stood out and gotten word of mouth easily.
Maybe your release timing was off too, since your release time was a week or two before TGA as well.
61

Coughing baby vs hydrogen bomb at TGA bevause they hate anime looking games I fear
68
Samson retweeted

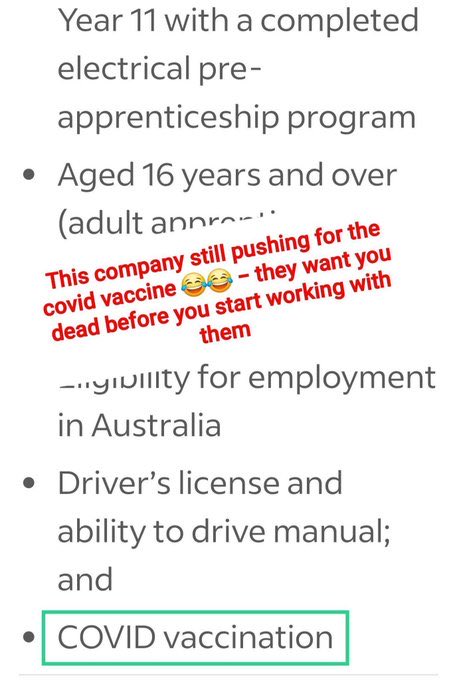
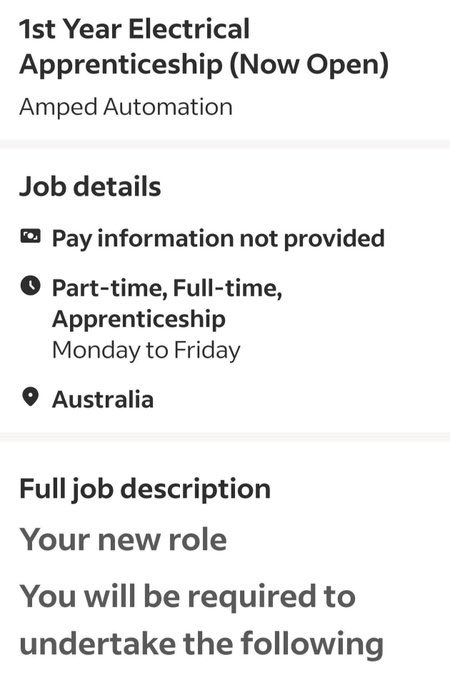
Unbelievable. Mandating a 16 year old to be jabbed. Even the TGA now say under 18s shouldn’t be vaccinated against Covid. It’s too risky.
2
9
18
326

What @OneNationAus policies don't you like❓👇🏼
1. Immigration & Borders: Cap permanent/temporary visas at ~130,000 per year (major reduction from current levels). Deport ~75,000 illegal migrants/overstayers. Eight-year waiting period for citizenship and welfare access. Deport any visa holder who commits a crime. End skilled visa and student visa rorting/backdoors. Reintroduce Temporary Protection Visas. Refuse entry from nations fostering “extremist ideologies” incompatible with Australian values (historically focused on certain Muslim-majority countries). Withdraw from UN Refugee Convention and oppose UN Global Compact on Migration. Prioritize assimilation and “Australians first.”
2. Government Spending & Waste: Bold $90 billion annual budget savings plan. Abolish Department of Climate Change and related agencies (~$30B savings). Abolish National Indigenous Australians Agency (NIAA), redirecting aid directly (~$12.5B). Review/eliminate duplication in Education and Housing departments. Reform NDIS (means-testing, reasonable support only). Cut foreign aid (~$3B). Withdraw from UN, WHO, Paris Agreement, and other international bodies. Reduce arts and multicultural program funding. Remove excessive building regulations (e.g., mandatory wheelchair compliance for all new homes).
3. Energy & Climate: End “Net Zero” policies, repeal Renewable Energy Target, and withdraw from Paris Agreement. Expand reliable baseload power: coal, gas, and nuclear (repeal nuclear ban; build reactors). Oppose subsidies for foreign-owned wind/solar. Prioritize affordable, secure energy for households, businesses, and industry over emissions targets, citing insufficient evidence for catastrophic man-made global warming.
4. Cost of Living & Tax: Halve fuel excise (temporarily). Slash electricity bills by 20% via market reforms. Raise tax-free threshold. Introduce joint income tax filing (income splitting) for couples with dependent children. Tax relief for self-funded retirees and higher pensioner earning limits. GST moratorium on building materials for new homes (up to $1M, 5 years). Reduce freight costs and other targeted relief.
5. Housing & Infrastructure: Link affordability to lower migration and reduced red tape. GST exemption on new home building materials. Review excessive government fees and building codes. Build new water infrastructure (dams) for farmers and population needs. Ban foreign ownership/sale of water rights with full disclosure. Prioritize Australian jobs in infrastructure.
6. Free Speech: Enshrine free speech in the Constitution. Oppose censorship, “hate speech” laws, and government overreach. Hold conferences and protests against speech restrictions.
7. Economy, Trade, & Jobs: Protectionist stance—review/revoke free trade agreements not in Australia’s interest; reimplement import tariffs where needed. “Australians first” for jobs; boost apprenticeships and oppose foreign labor undercutting wages. Oppose foreign ownership of agricultural land, businesses, and key assets. Move foreign multinationals to transactions-based tax system. Prioritize national economic sovereignty.
8. Health: Bolster regional medical workforce (e.g., 3-year contracts with HECS debt forgiveness). Boost Medicare rebates, crack down on fraud. Oppose COVID-19 vaccine mandates; push for Royal Commission into pandemic management. Abolish or reform TGA (mentioned in spending cuts). Mandatory photo ID for Medicare.
9. Family & Social: Pro-life stance—roll back late-term/extreme abortion laws; recognize life begins at conception; support gestational limits and conscientious objection. Family tax benefits and income splitting to support traditional families and home-schooling. Oppose “woke” policies.
10. Indigenous Affairs and Welfare: Abolish NIAA and “Aboriginal industry” intermediaries; direct assistance only. Criticism of “Close the Gap,” excessive welfare, and Native Title expansions (historical). Call for personal responsibility
23

Even within your family which problem have you solved that never occur again, nownyoi want another wet of wise people that arrcfar better than your family to solve your problem tga you cant solve. Do your bit.
6

Chapter 58: Epilepsy
1. Chapter Overview
Epilepsy is not exclusively a disease of the young. In fact, incidence rates exhibit a bimodal distribution, with the highest peak occurring in older adults (aged 65 and above). However, because the clinical manifestations of seizures in the elderly are notoriously subtle and often masked by multimorbidity, geriatric epilepsy is frequently underdiagnosed, misdiagnosed, or diagnosed late.
2. Secondary Etiology
Unlike idiopathic or genetic epilepsies prevalent in youth, new-onset epilepsy in older adults is overwhelmingly secondary to acquired structural brain insults (symptomatic epilepsy):
Cerebrovascular Disease: The leading cause of geriatric epilepsy (accounting for up to 50% of cases with a known etiology). The risk of developing an epileptogenic focus is remarkably high following an ischemic or hemorrhagic stroke.
Neurodegenerative Diseases: Particularly in the later stages of Alzheimer's disease, patients are highly susceptible to unprovoked seizures.
Other Causes: Brain tumors, metabolic disturbances (e.g., severe hyponatremia, hypoglycemia), head trauma, and CNS infections. However, up to one-third of cases remain cryptogenic (of unknown cause despite modern investigation).
3. Atypical Clinical Presentation
Seizure Semiology: Older adults rarely present with classic generalized tonic-clonic seizures ("grand mal"). The vast majority experience focal onset impaired awareness seizures (formerly complex partial seizures). These manifest subtly as sudden staring spells, unresponsiveness, purposeless automatisms (e.g., lip-smacking, picking at clothes), or transient memory lapses.
The Postictal State: This is a critical hallmark in the elderly. While younger patients may recover within hours, an older adult's postictal confusion, profound lethargy, or focal weakness (Todd's paresis) can persist for days or even up to a week. This prolonged state is routinely misdiagnosed as delirium, an acute stroke, or a sudden worsening of dementia.
4. Diagnostic and Differential Challenges
Differential Diagnosis: Clinicians must meticulously distinguish epilepsy from syncope (especially cardiogenic syncope with myoclonic jerks, frequently mistaken for a convulsion), Transient Ischemic Attacks (TIAs), delirium, and Transient Global Amnesia (TGA).
Investigations: Routine Electroencephalograms (EEGs) have lower sensitivity in older adults; a normal EEG does not rule out epilepsy. High-resolution MRI is indispensable for identifying underlying structural lesions (e.g., silent infarcts or tumors).
5. Principles of Pharmacotherapy and the Polypharmacy Dilemma
Threshold for Treatment: Because the recurrence risk is exceedingly high and even a single generalized seizure can result in devastating falls, fractures, or cardiopulmonary compromise in a frail body, Antiseizure Medications (ASMs) are typically initiated after the first unprovoked seizure in older adults.
Initiation and Titration: The cardinal rule is "Start low, go slow." The aging brain is exquisitely sensitive to neurocognitive side effects; rapid titration easily provokes cognitive slowing, dizziness, and ataxia (leading to catastrophic falls).
Drug Selection and Interactions: Given ubiquitous polypharmacy, traditional enzyme-inducing ASMs (like phenytoin and carbamazepine) must be actively avoided. They severely disrupt the metabolism of vital cardiovascular and anticoagulant medications. Moreover, carbamazepine and oxcarbazepine carry a high risk of inducing severe hyponatremia. Newer-generation ASMs (e.g., levetiracetam, lamotrigine) are the preferred first-line agents due to their favorable pharmacokinetic profiles and lack of significant drug-drug interactions.
—Brocklehurst’s Textbook of Geriatric Medicine and Gerontology

1
15
40
第58章:癫痫
1. 章节概述
癫痫并非只是年轻人的疾病。事实上,癫痫的发病率在整个人群中呈“双峰”分布,而老年期(65岁及以上)的发病率是所有年龄段中最高的。然而,由于老年人发作的临床表现极具隐蔽性,加之老年人群中普遍存在多重共病,老年期癫痫常常被漏诊、误诊或延迟诊断。
2. 继发性病因学
与年轻人中常见的特发性或遗传性癫痫不同,老年人新发癫痫绝大多数是由于大脑获得了某种结构性损伤(继发性/症状性癫痫):
脑血管疾病:是老年期癫痫最主要的原因(约占已知病因的50%)。尤其是在缺血性或出血性脑卒中之后,形成癫痫灶的风险极高。
神经退行性疾病:特别是阿尔茨海默病晚期,患者极易出现无先兆的癫痫发作。
其他原因:脑肿瘤、代谢紊乱(如严重的低钠血症、低血糖)、头部外伤及中枢神经系统感染。但仍有约三分之一的病例在现有技术下无法找到明确原因(隐源性)。
3. 临床表现的“非典型性”
发作形式:老年人较少出现典型的全身强直-阵挛发作(“大发作”)。他们绝大多数表现为局灶性发作伴意识障碍(过去称为复杂部分性发作)。这种发作常常表现为突然的凝视、反应迟钝、漫无目的的动作(如咂嘴、摸索衣物)或短暂的记忆空白。
发作后状态 (Postictal State):这是老年癫痫的一个极为关键的特征。年轻人在发作后可能几小时就能恢复,而老年人的发作后意识模糊、嗜睡或局灶性无力(Todd麻痹)可能持续数天甚至长达一周。这极易被误诊为谵妄、中风发作或痴呆症恶化。
4. 诊断与鉴别诊断的挑战
鉴别诊断:临床医生必须极其谨慎地将癫痫与晕厥(尤其是伴有肌阵挛跳动的心源性晕厥,常被误认为是癫痫发作)、短暂性脑缺血发作(TIA)、谵妄和一过性全面性遗忘症(TGA)区分开来。
辅助检查:常规脑电图(EEG)在老年人中的敏感性较低,正常结果不能排除癫痫。高分辨率核磁共振成像(MRI)对于寻找结构性病因(如微小梗死灶或肿瘤)至关重要。
5. 药物治疗原则与多重用药困境
治疗阈值:由于老年人发生第二次癫痫的风险极高,且哪怕一次全身性发作也可能导致致命的跌倒、骨折或心肺并发症,因此通常在首次明确的无诱因发作后即开始抗癫痫药物(ASMs)治疗。
起始与滴定:核心原则是**“起始剂量极低,缓慢滴定(Start low, go slow)”**。老年人对药物副作用极其敏感,极易出现认知迟缓、头晕和共济失调(导致跌倒)。
药物选择与相互作用:老年人普遍存在“多重用药”。必须极力避免使用传统的肝药酶诱导型药物(如苯妥英钠、卡马西平),因为它们会严重干扰心血管药物和抗凝药的代谢,且卡马西平和奥卡西平极易在老年人中引发严重的低钠血症。新一代抗癫痫药物(如左乙拉西坦、拉莫三嗪)因其较少的药物相互作用和更好的耐受性,已成为老年期癫痫的首选。
—Brocklehurst’s Textbook of Geriatric Medicine and Gerontology

10
80

Kohli ke bina Eng series juta tga Ind bhadwe uske baad jab se kohli team ne aya sab se India harne lagi .
3
10
きゆ retweeted

Jun 7
米国Macro Plus :6/7アップデート
QT継続のフラグによるAI判定を修正すると
WALCL小幅↑ / TGA↑ / FRP↑ → NetLiq↓がより正確な表現。
現時点は「強い上昇トレンドの中の黄色信号」4Hで安値切り上げ、VIX低下、NetLiq改善を確認してから押し目を拾いたい。


May 31

米国Macro Plus 5/31アップデート
・AIのEventNET 1W流動性:逆風で横ばい〜浅い押し目判定
・NAAIM指数も先週次点で98.39と100越えのレバレッジをかけてるのか、ポジション落としてくるか気になりますね。AAIIは先週よりBull派が若干増えた。


7
11
105
5,103


The Australian federal and state governments, their health (🙄) departments, the TGA and state media knew too because their own reporting told them so.
Jun 13

The biggest scandal of our lifetime Sen. Ron Johnson “the Covid shot adverse event cover up”
The Government knew and the US media didn’t report it.
In the UK the BBC, ITV, Sky, GB news and C4 all knew. The Times, Telegraph, Mail, Sun and Guardian knew.
Because I told them in 2022
7