
Cryptococcal meningitis, as the India ink preparation is pathognomonic for Cryptococcus neoformans.
1
1
54

C. Cryptococcal Meningitis
The India ink stain is the definitive clue here, it's pathognomonic for Cryptococcus neoformans.
Is the patient RVD positive?
1
1
43

🔥 EHA2026 | Invasive Fungal Disease After HSCT & Cellular Therapy
Prof. Varun Mehra — diagnosis beyond “one test”
🍄 EORTC/MSG criteria evolved: 2002 → 2008 → 2019
Probable invasive fungal disease requires integration of:
🧬 Host factors
🖥️ Clinical/radiological features
🧫 Mycological evidence
🧬 High-risk host factors now extend beyond classical neutropenia
Neutropenia
HSCT
SOT
GVHD
Steroids
T-cell immunosuppressive agents
BTK inhibitors
CGD / SCID and other immune defects
🧪 Mycology is improving, but interpretation is nuanced
Galactomannan has updated thresholds
Aspergillus PCR is increasingly incorporated
But biomarkers should never be interpreted without imaging host risk antifungal exposure
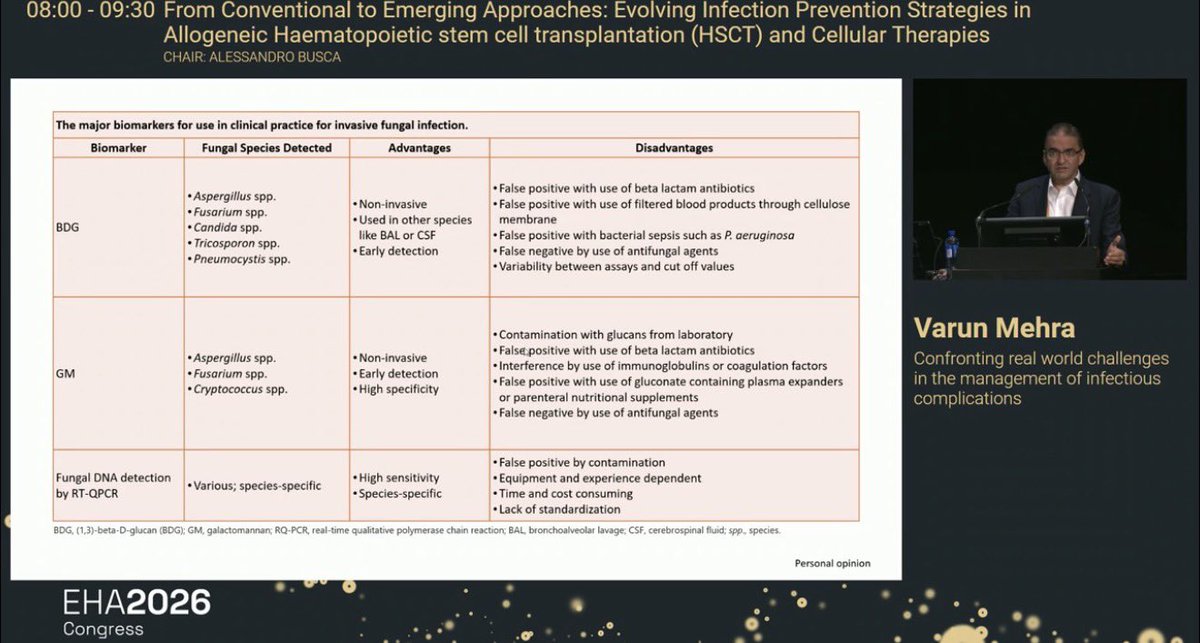
🧫 β-D-glucan: broad but imperfect
Detects signals from:
Aspergillus
Fusarium
Candida
Trichosporon
Pneumocystis
✅ Non-invasive
✅ Useful in BAL/CSF and other specimens
⚠️ False positives: β-lactams, filtered blood products, bacterial sepsis
⚠️ False negatives: concurrent antifungal therapy
⚠️ Assay variability limits cut-off reliability
🧫 Galactomannan: more specific for Aspergillus
Detects mainly:
Aspergillus
Fusarium
Cryptococcus
✅ Non-invasive
✅ Early detection
✅ Higher specificity
⚠️ False positives: glucan contamination, β-lactams, gluconate plasma expanders, nutritional supplements
⚠️ False negatives: mold-active antifungal therapy
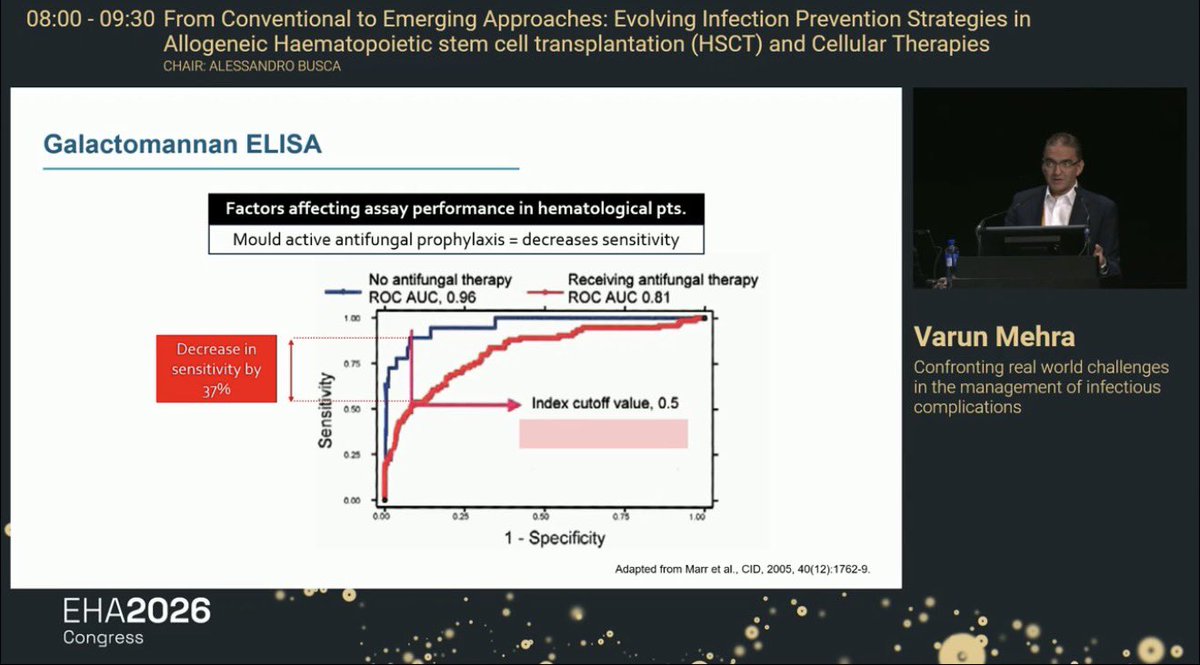
⚠️ Key galactomannan pearl
Mold-active antifungal prophylaxis can reduce GM sensitivity significantly.
Slide: sensitivity decreased by ~37% in hematology patients receiving antifungal therapy.
🎯 A negative GM does not exclude invasive aspergillosis in a patient already on mold-active prophylaxis.
🧬 Fungal PCR / RT-qPCR
✅ High sensitivity
✅ Species-specific
⚠️ Contamination risk
⚠️ Equipment/operator dependent
⚠️ Time/cost burden
⚠️ Lack of standardization remains a real-world limitation
🖥️ Radiology reflects fungal burden and disease phase
Early bronchial phase: bronchiectasis, tree-in-bud, ground-glass
Progression: nodules ± halo, consolidation
Angio-invasive phase: hemorrhage, infarction, necrosis
Late/recovery phase: air-crescent/cavitation may appear with neutrophil recovery
🫁 BAL often outperforms serum in localized pulmonary disease
BAL galactomannan may rise earlier/higher than serum when disease is airway/pulmonary localized.
Serum GM becomes more useful with angio-invasive/disseminated disease.
🧠 Clinical interpretation pearl
Do not ask: “Is GM positive?”
Ask:
Host risk?
CT pattern?
BAL vs serum?
On mold-active prophylaxis?
Neutropenic or recovering neutrophils?
Culture/PCR/histology available?
Clinical trajectory?
🎯 Practical takeaway
✅ IFD diagnosis is probabilistic, not binary
✅ EORTC/MSG criteria combine host imaging mycology
✅ Mold-active prophylaxis reduces biomarker sensitivity
✅ BAL testing is critical when serum markers are negative but CT is suspicious
✅ Histology/culture remains decisive when feasible
✅ Early antifungal decisions should not wait for perfect proof in high-risk HSCT/CAR-T patients
📚 Source: EHA2026 Congress slides — From Conventional to Emerging Approaches: Evolving Infection Prevention Strategies in Allogeneic HSCT and Cellular Therapies; Prof. Varun Mehra. Slide-cited references include Donnelly et al., Clinical Infectious Diseases 2019, Marr et al., Clinical Infectious Diseases 2005, and Stanzani et al., Current Fungal Infection Reports 2016.
#EHA2026 #HSCT #AlloHSCT #CellularTherapy #InvasiveFungalDisease #IFI #Aspergillosis #Galactomannan #BetaDGlucan #FungalPCR #InfectionPrevention #Hematology #KFSHRC #ESH #DrChokriBenLamine


1
165

7 y/o Cam was safely brought in after being spotted with severe conjunctivitis affecting both eyes. With nasal congestion also present, our vet team have sent off bloods to check for cryptococcus. He has begun treatment. Support our NRKH expansion: ow.ly/qB3J50Zb05c
1
3
37
271

Jun 12
Anyone paying attention to my cryptococcus theorizing should check this out.
pmc.ncbi.nlm.nih.gov/article…
1
5
198
ซีซี retweeted

Jun 11
เคล็ดลับไล่นกพิราบถาวร ฉบับไม่บาปและปลอดภัย🐦⬛🩶
นกพิราบ=พาหะเชื้อราอันตราย (Cryptococcus neoformans) เสี่ยงติดเชื้อ ;
⚠️ โรคคริปโตคอกโคสิส
⚠️ โรคเยื่อหุ้มสมองอักเสบ
⚠️ โรคปอดอักเสบ
มาดู 5 สิ่งที่นกพิราบกลัวที่สุด เพื่อไล่ให้อยู่หมัด !
-แสงสะท้อน: แขวนแผ่นซีดีเก่า/ฟอยล์ ให้แสงแยงตานก
-ที่เกาะไม่มั่นคง: ติดตั้งหนามกันนก หรือทาเจลไล่นก/จาระบีให้ลื่น
-กลิ่นฉุน: วางลูกเหม็น หรือฉีดน้ำส้มสายชู
-สัตว์นักล่า: วางตุ๊กตานกฮูก/งูปลอม (ต้องขยับเปลี่ยนมุมบ่อยๆ)
-เสียง/คลื่นรบกวน: ใช้เครื่องไล่นกอัลตราโซนิก หรือแขวนโมบายกระดิ่ง
💡 Tip ป้องกันระยะยาว:
-รีบเช็ดล้างขี้นกทันทีเพื่อลบฟีโรโมน (กลิ่นเรียกพวก)
-งดให้อาหารเด็ดขาด !!!!
-ขึงตาข่ายกันนกตรงระเบียง ป้องกันได้ 100%
cr. Thairath Online ,FB: Sikarin Hospital
#วิธีไล่นกพิราบ #ทริคดูแลบ้าน #สุขภาพ


4
9
10
253

Jun 11
21. A recently diagnosed HIV-positive man presents with fever and cough. The chest
radiograph shows bilateral perihilar interstitial infiltrates and apical ground-glass
shadowing. The most likely causative microorganism is?
What is the most likely diagnosis?
(a) Cryptococcus neoformans
(b) Mycobacterium tuberculosis
(c) Pneumocystis jirovecii
(d) Candida albicans
(e) Toxoplasmosis
#MedX #Radres
2
2
3
148
GLASS_PhD retweeted

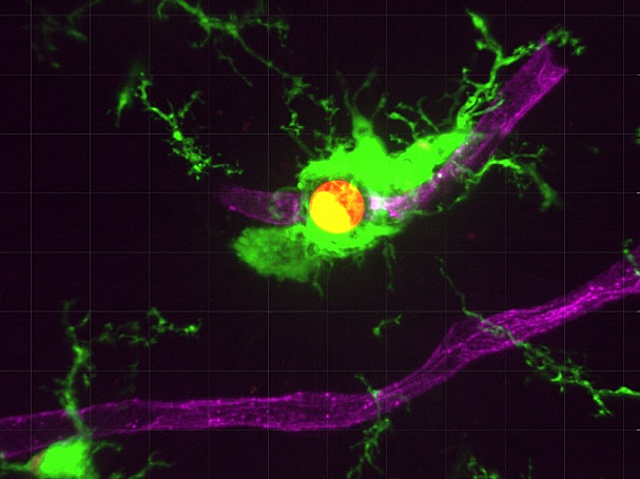
Brain capillary-infecting fungus Cryptococcus neoformans is detected by microglia through the vessel walls
📷 Chenxu Feng, Ge Wang & Yixuan Wang et al, @sjtu1896 in @PLOSBiology
➡️ bpod.org.uk/archive/2026/6/8 with @AntDLewis
6
12
867
monkey king retweeted

Jun 8
Cryptococcus neoformans is a fungus naturally found in soil and decaying wood. Because telephone poles are made of treated wood, they provide a perfect home for the fungus to grow.
Cryptococcus neoformans eats radiation using melanin, a dark pigment.
"RADIOSYNTHESIS" is a thing.
1
2
98

🧠🔬 In an HIV-positive patient presenting with fever, focal neurological deficits, and multiple intracerebral mass lesions, the leading differential is cerebral toxoplasmosis until proven otherwise.
📌 Top differentials: 1️⃣ Cerebral toxoplasmosis – most common cause of ring-enhancing brain lesions in advanced HIV (especially CD4 <100).
2️⃣ Primary CNS lymphoma – important mimic; often solitary or few lesions, frequently periventricular.
3️⃣ Tuberculoma/CNS tuberculosis – particularly relevant in endemic regions.
4️⃣ Fungal abscesses (Cryptococcus, Aspergillus) or pyogenic brain abscess.
5️⃣ Less likely: progressive multifocal leukoencephalopathy (PML) if lesions are non-enhancing.
🔍 Immediate workup: ✅ CD4 count and HIV viral load
✅ Toxoplasma IgG serology
✅ Contrast-enhanced MRI with DWI/MRS if available
✅ Blood cultures and TB evaluation as clinically indicated
✅ Avoid lumbar puncture initially if there is significant mass effect or raised ICP
💡 Practical approach: If imaging shows multiple ring-enhancing lesions involving the basal ganglia/corticomedullary junction in an HIV patient, many clinicians would start empiric anti-toxoplasma therapy and reassess clinically and radiologically within 10–14 days.
⚠️ Failure to improve should raise strong suspicion for Primary CNS Lymphoma, warranting further evaluation with PET imaging, CSF EBV PCR (if safe), or stereotactic brain biopsy.
Excellent case—this is one of those classic scenarios where toxoplasmosis vs primary CNS lymphoma becomes the pivotal diagnostic challenge. 🩺🧠✨
1
3
463