
10h
Niezmiennie #DodajemyEnergii naszym wioślarkom i wioślarzom 💪 To był weekend pełen energii i rywalizacji na najwyższym poziomie! 🚣️🏆 Zobaczcie jak 6 i 7 czerwca na poznańskiej Malcie najlepsi polscy wioślarze rywalizowali podczas Enea Mistrzostw Polski Seniorów oraz Enea Mistrzostw Polski Masters. 🎥 #PremieraEnei 👇
Sportowe zmagania uzupełniała także nasza strefa aktywizacji, gdzie na odwiedzających czekały m.in. ergometry wioślarskie, warsztaty edukacyjne poświęcone odnawialnym źródłom energii, interaktywne symulatory VR oraz strefa relaksu.
Cieszymy się, że jako sponsor tytularny mogliśmy być częścią tego wydarzenia. Gratulujemy wszystkim zawodnikom osiągniętych wyników i dziękujemy za emocje, które przez dwa dni towarzyszyły rywalizacji na torze! 💙 #EneaMuremZaWiosłami
1
1
85

Our colleagues are attending ESC Preventive Cardiology 2026 in Ljubljana, Slovenia.
This congress brings together the latest scientific insights and innovations in preventive cardiology, a valuable opportunity to exchange knowledge.
#Cardiology #Ljubljana #ESC2026 #Ergometry


2
58

Apr 17
Ergometry test: optimal
Home pressure check, optimal
Have one more test next week and this is done.- “white coat syndrome“ is likely.-
Thanks for your caring and you support 🫶.- see you in a few days.-
Apr 15

Went for a check-up and the doctor told me my blood pressure was high.
I looked at him and said: “Have you heard of cryptocurrencies?” 😂
Now I have to do a 24-hour blood pressure monitor and some extra tests to check if it’s real or just “white coat syndrome.”
So for the next week I’ll be chilling and avoiding stress just in case.-
Im a pretty healthy guy so probably nothing but I must follow doctor orders…
see you after im done with the check, take care :).-
13
1
79
11,336

Mar 15
Batyr też miał ambitne plany🤣 Mam pomysł dla Czarnka, pisowskiego aktywu i ich wyborców - posadzić ich na ergometry lub rowery stacjonarne i podłączyć ich do jakiś generatorów prądu niech je zasilają pracą swoich mięśni. Ile pożytku z tego będzie. Czarnek w końcu schudnie 😉
2
31

2
173

Feb 8
The future of funding metabolic health: why the @vo2account exists
The latest bioenergetic data show a systemic collapse in human energy production: fat oxidation has declined by ~60% across age groups, glycolysis fails early under stress, and immune surveillance (particularly NK cell function) becomes energetically exhausted well before disease is diagnosed. This is not a clinical anomaly—it is a population-level shift that traditional healthcare, insurance, and fitness systems were never designed to detect or correct.
As metabolic capacity deteriorates, disease becomes longer, more complex, and more expensive, while recovery becomes slower and less predictable. Health and life insurers are structurally constrained to react only once diagnoses or events occur, by which point metabolic resilience is already lost and costs are locked in. Preventive funding at the level required to restore mitochondrial function, fat oxidation, and substrate flexibility is simply not viable within insurance risk pools.
This creates a new funding gap—and that gap is where the VO₂ Account operates.
The VO₂ Account is a health-banking product that treats metabolic capacity as a measurable, financeable asset, rather than an unpriced biological assumption. Using objective bioenergetic data (CPET, FatMax, RER dynamics, stroke volume response, longitudinal ECG signals), the VO₂ Account quantifies metabolic default risk early, before disease manifests. Capital is then deployed proactively to restore the energy systems that determine immune competence, recovery capacity, and long-term functional health.
Critically, when life insurers pay out critical illness or dreaded disease claims, those funds do not sit idle or dissipate through fragmented care. Instead, they flow into the VO₂ Account as working capital, dedicated to lifelong preservation and restoration of energy production. This includes home-based medical-grade ergometry, serial CPET to guide dosing, continuous ECG monitoring, and targeted nutritional strategies to rebuild mitochondrial efficiency and substrate flexibility.
Over time, this model reshapes health funding itself. Banking becomes the infrastructure layer for metabolic resilience, insurers remain focused on risk pooling and claims, and medicine shifts from reactive disease management to energy-system rehabilitation. Actuarially, this stabilizes long-tail risk by shortening disease duration, improving recovery trajectories, and preserving immune surveillance—outcomes that cannot be achieved once metabolic collapse is advanced.
In the future, health will not be funded around diagnoses. It will be funded around energy capacity.
The VO₂ Account is the first structure designed to do exactly that—turning bioenergetic data into capital allocation, and capital into sustained metabolic health.
2
1
11
1,733

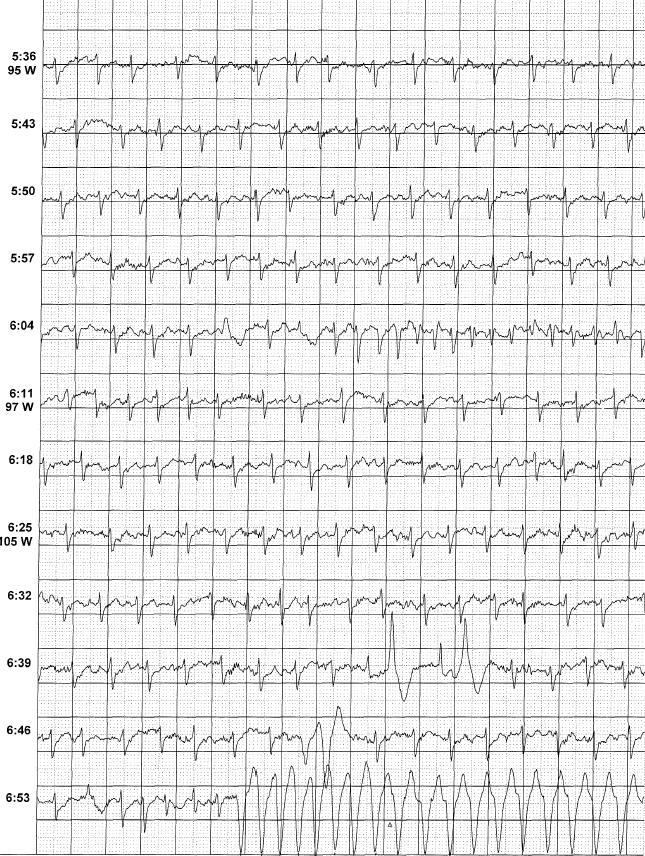
6 Dec 2025
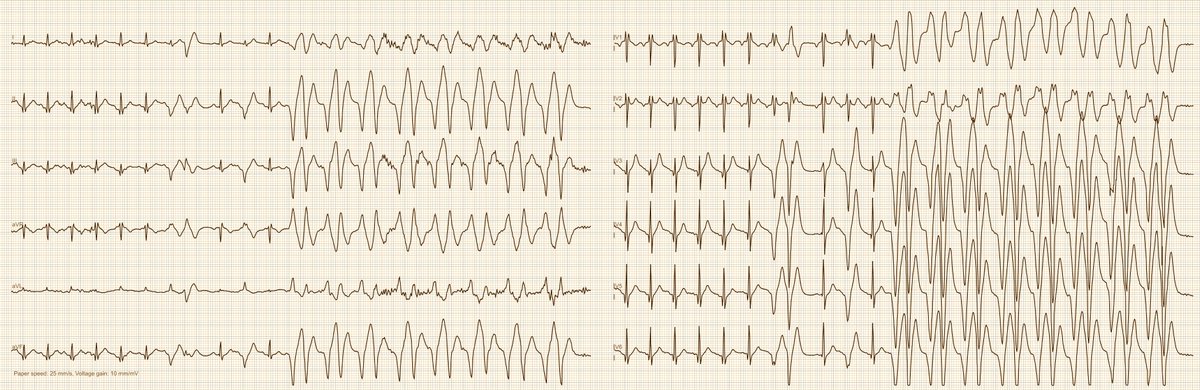
Palpitations during the recovery phase of a bicycle ergometry test. Green = heart rate. What do you see in the ECG?

2
3
12
2,517

2 Dec 2025
MITOCHONDRIAL RESCUE: THE SUPPLEMENT STRATEGY THAT ACTUALLY WORKS
You can't fix broken mitochondria with one magic pill. Anyone telling you otherwise is selling snake oil. But there's a supplement strategy that actually works because it targets multiple pathways simultaneously. Not theory. Published data.
When mitochondria fail, you get a cascade of problems. Electrons backflow through the respiratory chain, creating reactive oxygen species that damage DNA, proteins, and lipids. ATP production tanks.
The cell tries to compensate by cranking out more mitochondria, but eventually gets overwhelmed. You need exogenous support because your endogenous antioxidant systems can't keep up.
Most people peddle single supplements. CoQ10. Vitamin E. Creatine. Pick your favorite. But that's like trying to fix a car by only changing the oil. Multiple pathways are broken. You need multiple fixes.
The research is clear. Four compounds together, creatine, CoQ10, alpha-lipoic acid, and vitamin E, outperform any single ingredient. In muscular dystrophy mice, this combination beat prednisone, the only FDA-approved drug. When you combined the cocktail with prednisone, the results were even better. That's not additive. That's synergistic.
Here's what actually happened in the clinical trial. Sixteen patients with confirmed mitochondrial disease, MELAS, MERRF, Kearns-Sayre, CPEO, the whole lineup. Two months on the cocktail, two months on placebo, crossover design so everyone got both. The code was held by an external party. No way to rig the results.
CoQ10 levels went up. That's expected. But the real story is what happened to the biomarkers. DNA damage dropped. Lactate, which spikes when mitochondria can't function, decreased significantly. Lipid peroxidation, a marker of oxidative damage, improved. Every single biomarker of mitochondrial dysfunction moved in the right direction.
The critics said it was all CoQ10. So another trial was done, this time with CoQ10 alone at very high doses, 600 milligrams twice daily. Thirty patients. Same rigorous design. MR spectroscopy, lactate measurements, oxidative stress markers, everything.
Results? Nothing. Zero improvement in mitochondrial disease markers. A tiny bump in cycle ergometry performance, which means almost nothing. The multi-ingredient approach worked. The single ingredient didn't. Case closed.
The mechanism makes sense. If you have a complex three defect, for example, cytochrome B mutation, you need compounds that bypass the blockage. CoQ10, succinate, and riboflavin can partially do this. But you also need antioxidants to mop up the free radicals that accumulate from electron backflow. Vitamin E for membranes. Lipoic acid for the redox couple. Creatine to maintain ATP stores when oxidative phosphorylation fails.
One supplement hits one target. Multiple supplements hit multiple targets. This isn't complicated.
Now let's talk about body composition because this matters more than people realize. BMI is garbage. A DEXA scanner or caliper measurement tells the real story. People who look underweight by BMI are often obese by actual body fat percentage. Shrink your muscle, keep your fat, and suddenly you're 47 percent body fat while your doctor thinks you need to eat more.
In mitochondrial disease and muscular dystrophy, decreased activity leads to muscle loss and fat gain. The worst possible combination. You need to carry extra weight with compromised energy production. Plus, obesity itself causes secondary mitochondrial dysfunction. You're pouring gasoline on a fire.
Exercise is the gold standard for improving mitochondria, building muscle, and losing fat. Nothing beats it. But can supplements enhance what exercise does without blunting the benefits?
The answer is yes, but you have to be careful. Vitamin E and vitamin C together completely prevent the benefits of exercise. Published data. So any supplement strategy has to be tested with exercise, not just in sedentary conditions.
Seven ingredients emerged from extensive mouse model testing. Green tea, green coffee, forskolin, CLA, black tea extract, plus the mitochondrial core of CoQ10, alpha-lipoic acid, vitamin E, creatine, and beetroot. This combination was called Trim7.
In obese mice on a high-fat diet, Trim7 alone worked almost as well as exercise. But here's the key finding. When you combined Trim7 with exercise, the benefits doubled. The supplement didn't blunt exercise. It amplified it.
The mechanism? White adipose tissue, the fat you pinch under your belly, turns into a metabolic furnace. PGC1-alpha, the master regulator of mitochondrial biogenesis, goes up. Complex four activity increases. Lipid oxidation ramps up. UCP1 in brown adipose tissue uncouples mitochondria so they burn more energy. Inflammation drops.
A fatty liver expert tested Trim7 independently. Not paid. Not part of the company. Just skeptical. He completely reversed fatty liver disease in mice. Body fat dropped. Cholesterol dropped. PCSK9, a target for cholesterol drugs, decreased. The liver went from fat-infiltrated to nearly normal.
The human trial included 60 overweight men and women. Three months on Trim7 or placebo. Just basic diet and exercise advice, like you'd get from any family doctor. COVID hit during the trial, so some people became even less active and gained weight. But the groups were treated identically except for the supplement.
More people on Trim7 lost weight. Fatty liver markers dropped 26 to 28 percent. But here's what matters most: no loss of muscle mass. First strategy to show fat loss without muscle loss in the absence of structured exercise. Add exercise, and the results get better.
The core mitochondrial cocktail, backed by over 20 years of clinical use, is CoQ10, alpha-lipoic acid, vitamin E, and creatine. If you have complex one deficiency, add riboflavin. PDH deficiency, add thiamine.
Newer compounds show promise. Niacin derivatives are being studied, though high-dose NAR failed in phase three trials. Beetroot improves mitochondrial efficiency. Urolithin A from pomegranates is under investigation. But the core cocktail remains the foundation.
Practical implementation matters. Start with one supplement every few days. Add the next. Take everything with food, never on an empty stomach. Vitamins and minerals evolved to come in with food. Taking them isolated causes gastric distress and poor absorption.
Measure outcomes. Heart rate going up stairs. Lactate levels. Plasma amino acids. GDF-15. Body composition scales with bioelectric impedance cost $130 and track fat versus muscle reasonably well. If you're trying something, track whether it's working.
The doses are straightforward standard. CoQ10, Alpha-lipoic acid, Vitamin E, Creatine monohydrate. These aren't exotic compounds. They're available everywhere.
For weight loss and mitochondrial enhancement, add forskolin, beetroot extract, green tea, and green coffee bean extract. The full Trim7 formulation if you want the exact combination from the trials.
This isn't one-size-fits-all. Complex one deficiency needs riboflavin. PDH needs thiamine. MELAS needs arginine. But the core principle holds: multiple pathways broken means multiple fixes required.
The research is published. The mechanisms are understood. The clinical outcomes are documented. Twenty years of patient use with government funding in Ontario based on randomized controlled trial data.
You want to rescue your mitochondria? Stop looking for magic bullets. Use the multi-ingredient strategy that targets oxidative stress, ATP depletion, electron transport chain dysfunction, and inflammatory signaling simultaneously. Add exercise because nothing beats it. Track your outcomes so you know what's working.
That's how you actually fix mitochondrial dysfunction.
Everything else is noise.
This is no medical advice.
17
56
311
18,737

gm @PGC1a_RB
Some food for thought
Chris Masterjohn raises a thoughtful and commonly debated point in the longevity/training community: if the primary goal of zone 2 (low-intensity steady-state) cardio is to increase mitochondrial density and efficiency in skeletal muscle, why limit that stimulus to mostly the legs with running or cycling when you could distribute it across more of the body with rowing or boxing?
Where Masterjohn Is Correct
Mitochondrial biogenesis and density increases in skeletal muscle are overwhelmingly local/muscle-specific rather than systemic. The primary signaling pathways (PGC-1α, AMPK, p38 MAPK, etc.) are activated by metabolic stress inside the contracting muscle fibers themselves — Ca²⁺ flux, ADP/AMP ratios, redox changes, mechanical load, etc. If a muscle isn’t meaningfully recruited, it receives little to no direct mitochondrial stimulus for new mitochondria.
•Leg-dominant activities (cycling, running, inclined walking) → primarily increase mitochondrial density in the quads, hamstrings, glutes, calves (and to a lesser extent the hip flexors/core stabilizers).
•Upper-body muscles (shoulders, lats, arms, upper back) get almost nothing direct from pure cycling/running.
•Rowing recruits ~80–85% of muscle mass (legs back arms core) → more total muscle gets the mitochondrial stimulus.
•Properly controlled low-intensity boxing (slow shadowboxing or light bag work) recruits arms, shoulders, rotational core, and some legs via footwork → even broader recruitment, especially rotational/oblique muscles that are almost completely neglected in linear cardio.
Studies comparing large-muscle-mass vs small-muscle-mass exercise (e.g., two-leg vs one-leg cycling, or cycling vs arm leg ergometry) consistently show greater acute metabolic disturbance and larger training-induced mitochondrial adaptations when more muscle mass is active, even at the same relative intensity. Elite cross-country skiers or rowers often show extremely high mitochondrial density in both upper and lower body because they train the whole body.
So Masterjohn’s core criticism is physiologically sound: if your explicit goal is “mitochondria in as many muscles as possible,” full-body or upper-body-inclusive modalities are objectively superior to pure legs-only.
Where the Argument Is Overstated or Incomplete
The vast majority of people doing zone 2 are not trying to maximize mitochondrial density across every single muscle fiber in the body. The primary health and performance goals of zone 2 are:
1Improve fat-oxidation efficiency and metabolic flexibility (systemic).
2Increase lactate clearance capacity (partly systemic — lactate produced in legs can be shuttled to and oxidized by heart, liver, brain, and even inactive muscle mitochondria).
3Build capillary density and aerobic enzyme activity in the working muscle (local, but legs are ~50–60% of muscle mass, so still huge total effect).
4Improve central cardiovascular factors (stroke volume, plasma volume, cardiac output) — these are largely systemic and don’t care which muscles are moving.
5Allow high weekly volume with low fatigue/interference with strength training.
For pure health/longevity (not sport-specific performance), legs-only zone 2 still captures the overwhelming majority of the benefit because:
•Legs represent the largest muscle mass → biggest absolute mitochondrial gain.
•It’s far easier to accumulate 3–6 hours/week strictly in zone 2 on a bike or treadmill without local arm/shoulder fatigue forcing you out of the zone.
•Elite runners and cyclists (who almost exclusively train legs) have some of the highest measured mitochondrial densities and fat-oxidation rates on the planet — clearly legs-only is sufficient for world-class adaptations.
4
5
505
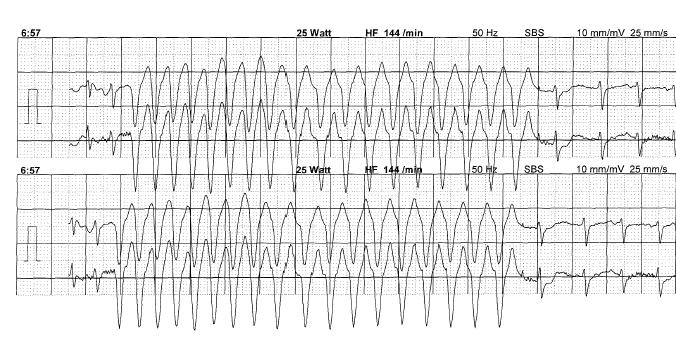
8 Nov 2025
Not often seen 😀 A 25-year-old man reports severe palpitations during physical exertion; he once lost consciousness during a 10 km run. Here is an excerpt from the bicycle ergometry test at 125 W load. Probable diagnosis?
18
7
66
11,254
12 Oct 2025
In addition, I would perform an ergometry test.
1
2
354

7 Oct 2025
Efficacy of arm crank ergometry on individuals with spinal cord injury: a systematic review of randomized controlled trials tinyurl.com/bddswvcf #icurehab #A2Fbundle
1
2
382

18 Sep 2025
Together with our partner MGC Diagnostics, colleagues Martin Hommes & Jan Willem Wisselink are showcasing Lode’s reliable and innovative ergometry solutions.
📍 Booth #215
🤝 Let’s connect!
#Rehabilitation #MedicalTechnology #Ergometry #Lode #AACVPR #Florida


1
2
90

Przez najbliższe dni seniorki i seniorzy z całej stolicy będą rywalizować w aż 13 dyscyplinach - od pływania, biegania i nordic walking, przez tenis i ergometry wioślarskie, aż po szachy, brydża i strzelanie z łuku.
#Warszawa #StolicaWolnegoCzasu @RKaznowska @AKTYWNAWARSZAWA




1
2
2,672
4 Sep 2025
Watch how Dr. Smedema & team use the Lode Angio Imaging ergometer to enable exercise echocardiography with optimal heart visualization, comfort & accuracy. Reliable. Reproducible. Indispensable.
👉lode-ergometry.com/product/a…
#Ergometry #radiology #Cardiology #Imaging #SouthAfrica
3
37

Podczas tegorocznych targów MSPO w Kielcach p. Anna Kwiatkowska i p. Mariusz Urbaniak przekazali ergometry wioślarskie weteranom.🤝
#MSPO2025 #Kielce
@MON_GOV_PL




2
5
9
3,408

16 Aug 2025
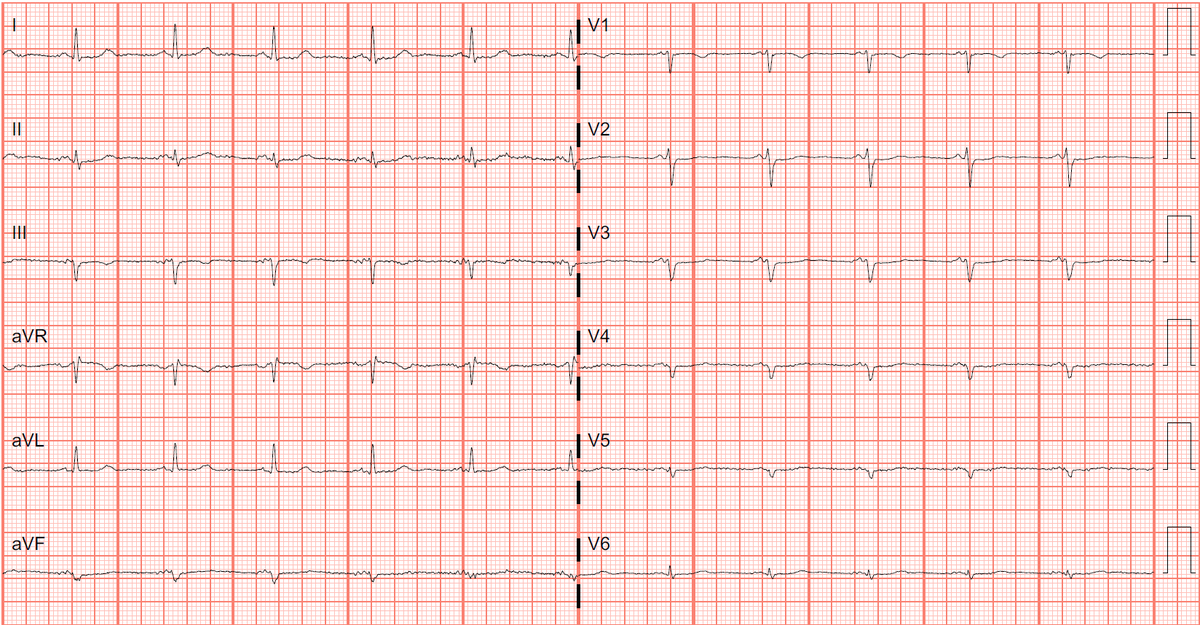
69yo female
Dyspnea on exertion
TTE showed moderate-severe MR
Dx?
1st ECG baseline, 2nd ECG on Ergometry
@ecgandrhythmRoe
@EcgOxford
@DrRazi4
@PendellM
@RobertHermanMD
@Arron_Pearce_
@ECGwithReid
@EM_Resus
@PMcardioBot
#ECG #CardioTwitter #MedTwitter #MedX
4
2
9
856

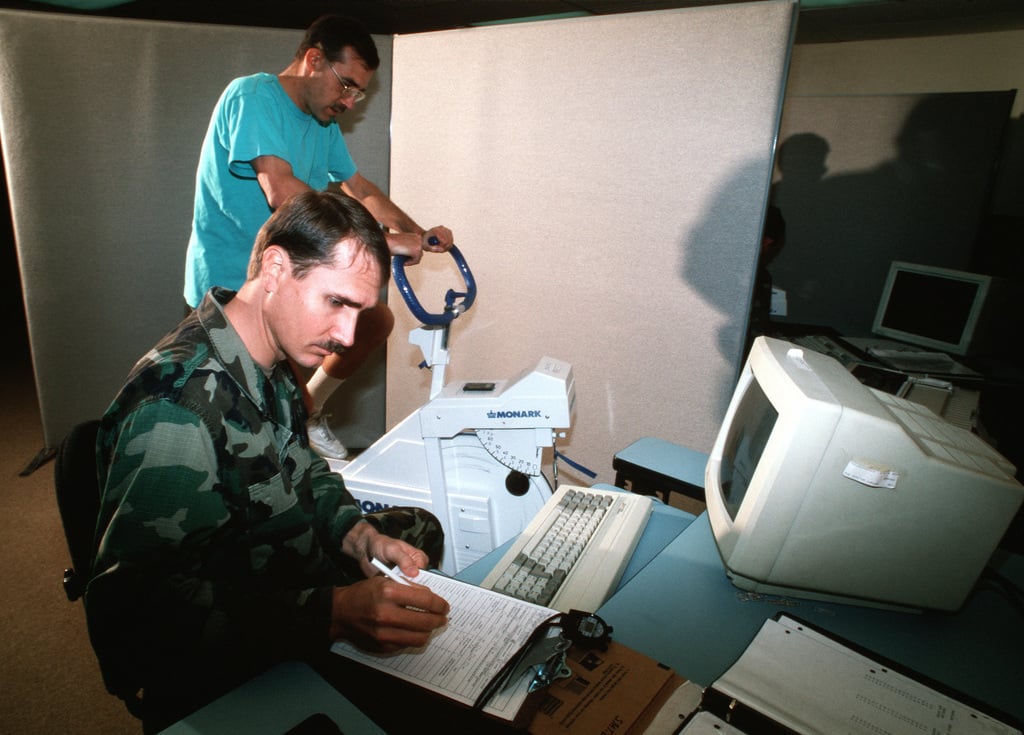
8 Aug 2025
Old enough to remember a few years of a "cycle ergometry" test because the 1.5mi run was killing Airmen.
There was a metronome to keep you from fucking it up by overspeeding the pedaling.
2
9
248

21 Jun 2025
Today’s Daily Dose ☕️: Critical care 🥼🩺
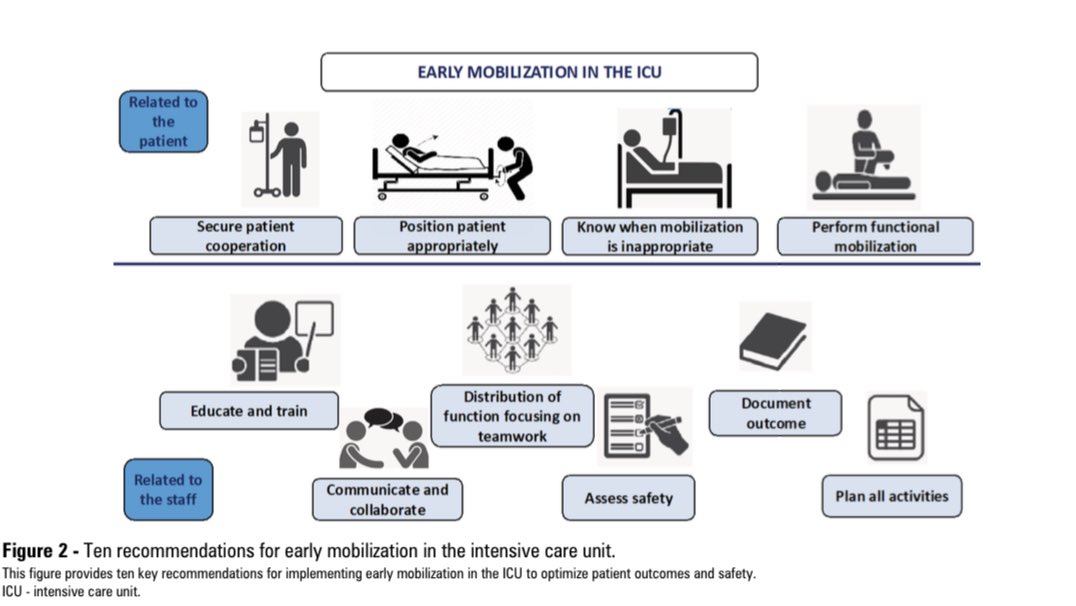
Early mobilization of critical care patients
🔎 Intro 🏥📚🧠
Several complications arise from prolonged bed rest in the ICU, including muscle weakness, impaired physical function, and neurocognitive and psychiatric symptoms collectively termed post–intensive care syndrome (PICS) 🛌🧠💊. Acute illness often precipitates ICU-acquired weakness (ICUAW), affecting both peripheral and respiratory musculature, and occurs in up to 25% of critically ill patients, correlating with increased in-hospital morbidity, mortality, and long-term disability 📊⚠️📝. Mobilization—encouraging active movement and out-of-bed activities—is a core component of the “ABCDEF” bundle and, when initiated within 72 hours of ICU admission with concurrent nutritional support, significantly reduces mechanical ventilation duration and hospital length of stay ⏱️🥗🚴
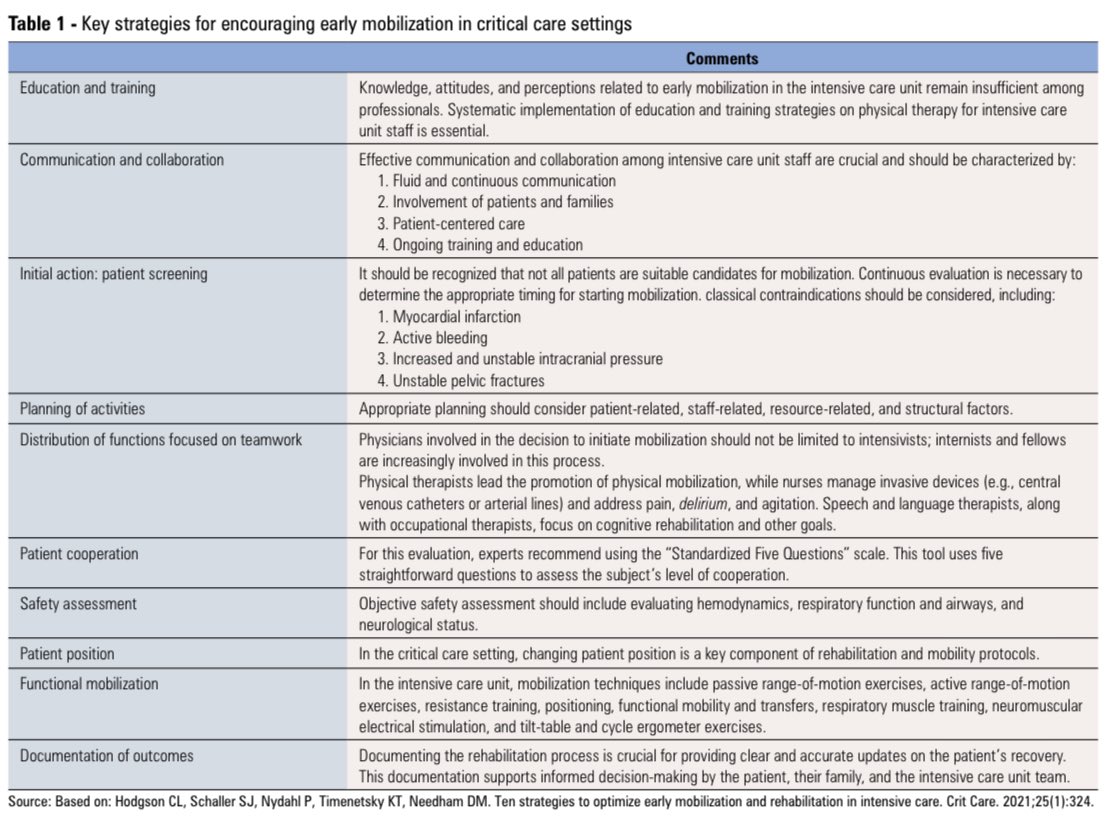
🩺📚 Education and Training 🎓👩⚕️
Effective early mobilization hinges on comprehensive education for ICU staff, yet surveys show only 2.5% of nurses and 16.8–52.3% of healthcare workers demonstrate adequate knowledge and positive attitudes towards mobilization 🔢📉👩🏫. Strategies include:
🎯 Structured curricula on physical therapy modalities and ICUAW prevention.
✔️ Simulation-based workshops with mentorship programs to reinforce guidelines.
☑️ Regular interprofessional debriefs and feedback loops to sustain competency and confidence.
✅ Embedding mobilization goals into daily rounds and care plans to foster a culture of mobility.
🛡️🔍 Initial Action: Patient Screening 🩸🩺
Daily screening protocols assess hemodynamic, respiratory, neurological, and metabolic stability to identify candidates and contraindications such as myocardial infarction, active bleeding, unstable intracranial pressure, and pelvic fractures 💔💉🚨. Balanced against risks of desaturation, hypotension, and device dislodgement, up to 1% of mobilizations result in serious adverse events, underscoring the importance of rigorous pre-mobilization evaluation and individualized risk–benefit analysis 📋⚖️.
🤝👥 Distribution of Functions Focused on Teamwork 💪🏥
Multidisciplinary collaboration is vital, with roles including:
✔️ ICU physiotherapists leading exercise prescription and progression.
☑️ Nurses managing invasive lines, sedation, and agitation control.
✅ Speech and language therapists and occupational therapists targeting cognitive rehabilitation and functional goals.
👉 Shared decision-making and clear communication streamline mobilization plans and optimize resource utilization.
🗓️📝 Planning of Activities ⚙️🔄
Activity plans progress stepwise:
🎯 From passive range-of-motion and neuromuscular electrical stimulation in sedated or non-cooperative patients.
✔️ To active transfers, sitting, and standing with assistance.
☑️ To ambulation and cycle ergometry as patient tolerance and strength improve.
✅ Session intensity, frequency, and duration tailored to individual tolerance with ongoing reassessment and adjustments documented in the ICU Mobility Scale and other validated tools.
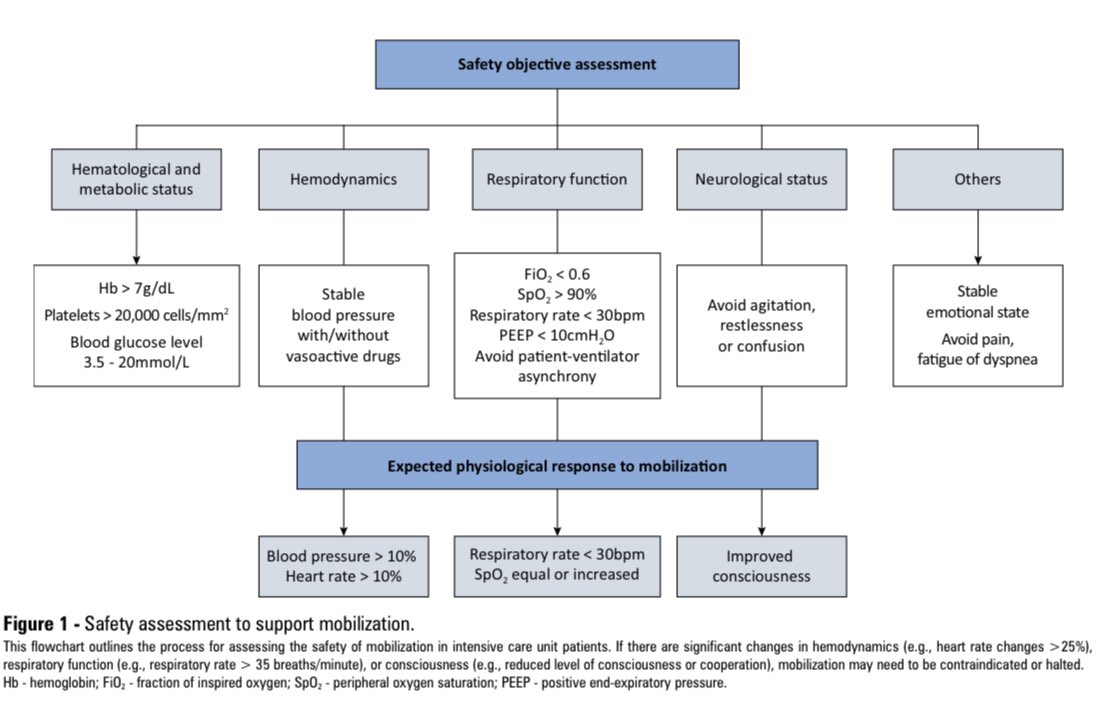
⚙️🛡️ Safety Objective Assessment 📊🚨
Key thresholds for safe mobilization include:
🎯 FiO₂ < 0.6 and PEEP < 10 cmH₂O to ensure adequate oxygenation without excessive ventilatory support.
✔️ SpO₂ ≥ 90%, heart rate and blood pressure changes < 20% from baseline to maintain hemodynamic stability.
☑️ Hemoglobin > 7 g/dL, platelets > 20 000/mm³, and blood glucose 3.5–20 mmol/L.
✅ Avoidance of agitation, pain, ventilator asynchrony, and need for rescue therapies, with immediate medical team review if thresholds are exceeded.
🚴📈 Functional Mobilization 🏃♂️🔄
Functional exercises—including assisted walking and activities of daily living simulation—complement passive and active range-of-motion work, resistance training, respiratory muscle training, and tilt-table exercises, promoting early independence and mitigating muscle atrophy and ventilator-associated complications.
1
6
14
1,242