People Who Dread Eating Insects Often Like It More Than They Expect, Brain and Heart Data Show | Ben Sullivan, ScienceBlog
The electrodes go on first. Eight of them, pressed into a snug cap over the scalp, plus a couple more clipped to the fingers to catch the heart’s faint electrical chatter. Then a researcher in a lab in central Portugal slides a small brown bar across the table and says, simply, that the volunteer is about to eat a protein bar. What the volunteer does not always know is that the bar is made from insects. And what nobody in the room knows yet is that the body is about to give a rather different answer than the mouth will.
That gap, between what people say about eating bugs and what their nervous systems do, is the thing Andreia Ferreira set out to measure. A PhD candidate at the University of Beira Interior, she and her colleagues wanted to get underneath the survey responses, where the polite no often lives.
The premise is hardly frivolous. With the global population heading past nine billion by mid-century and protein demand climbing with it, insects keep coming up as a low-footprint alternative to meat: less land, less water, fewer greenhouse gases, and a respectable load of iron, zinc and calcium per bite. The European Union recognized them as a novel food back in 2018, and you can now buy crickets, locusts and mealworms (frozen, dried, or milled into powder) across the bloc. The catch has always been the human one. Westerners, the research kept finding, are put off. Disgust, supposedly, does the blocking.
So the team built an experiment to watch the disgust happen. Or not.
What the Body Said
Thirty-eight adults, none of whom had ever knowingly eaten an insect, sat through a tasting wired up to an electroencephalography headset and an electrocardiogram. They each ate two bars, one insect-based and one ordinary cereal, both flavored with apple and cinnamon so the contest was reasonably fair. The kit recorded brain waves and heart rate before, during and after each mouthful. Some volunteers were told the truth about what they were chewing. Others were told the insect bar was just cereal, a small deception designed to separate the body’s reaction from the mind’s expectations.
The heart gave it away. Beats per minute climbed during the insect bar in a way they didn’t for the cereal, a signature the team reads as arousal, the body sitting up and paying attention. The brain agreed: more activity in the bands tied to attention and visual processing, the neural equivalent of leaning in for a closer look. Crucially, this happened even when people had no idea they were eating insects. The response, in other words, wasn’t a story the volunteers were telling themselves about bugs. It was something more immediate than that.
“The findings were very surprising,” Ferreira said. “This was really an unexpected result as literature said to us that consumers tend to reject these novel foods. The results show us the relevance of tasting experiments on promoting this new alternative.”
Then came the part that genuinely complicates the textbook. After tasting both bars, the volunteers were asked a blunt question: which did you prefer, the insect or the cereal? More of them chose the insect bar. In two of the four subgroups, roughly nine in ten picked it, including, awkwardly for tidy interpretation, several people who had been misled about which bar was which and still ended up praising the one made of bugs. The earlier work in this area, a 2017 study that watched people cook with mealworms, had logged anxiety and something close to an urge to flee. This time the urge to flee never showed up.
None of which means the disgust isn’t real. It is, and it arrives right on cue, in the second or two before the bar reaches the lips. The team’s argument is narrower and, perhaps, more useful: disgust may not be the thing that actually decides the matter.
Surprise, Not Squeamishness
Dig into the pre-tasting survey and a different culprit emerges. Awareness was strikingly thin. Fewer than half the participants knew insect foods were even for sale in Portugal, only 8 per cent had ever spotted them on a shelf, and a mere 3 per cent could name a species cleared for sale (the grasshopper, mostly). The emotion that came up first, ahead of fear and well ahead of disgust, was surprise. And surprise, the researchers point out, is not a verdict. It is a startle, a reaction to novelty rather than a judgment of worth. Disgust can sink a food for good; surprise just means you didn’t see it coming.
There are reasons to hold the conclusions loosely. The sample was small, drawn from one country, and the two bars (this is the honest snag) differed slightly in texture and sweetness, so some of the brain’s interest might be down to the snack rather than the insect. The hardware was the consumer-grade sort, twitchy about chewing and chatter, which is partly why seven volunteers’ recordings had to be binned. The authors are upfront about all of it.
Still, the practical thread is hard to ignore, and it points somewhere unfashionable: not at persuasion, but at exposure. If the barrier is unfamiliarity dressed up as revulsion, then arguing with people may matter less than simply handing them a sample. Free tastings, in-store trials, the bar tucked into a familiar shape and a familiar flavor, the things marketers reach for when a product is new rather than feared. Tellingly, fretting about the planet did not predict who would try insects; in this group, sustainability concern and future appetite barely tracked at all. The pitch, Ferreira suggests, has to do more than wave the word “new” around.
For now the finding sits as a small, sharp correction to a comfortable assumption, that we know our own minds about what we will and won’t put in our mouths. The volunteers in that Portuguese lab thought they knew. Their hearts, beating a little faster over a bar they’d been taught to refuse, had other ideas.
Read more:
scienceblog.com/people-who-d…

14
10
1,697
Chuck Petras retweeted

Jun 14
Setting California’s Forests on Fire Could Cut Wildfire Smoke by a Tenth | Ben Sullivan, ScienceBlog
For a century, the strategy was simple. See a fire, put it out. It worked, in a way, right up until it didn’t. All that diligent suppression let dead wood and brush and spindly young trees pile up across forests that had evolved to burn every few years anyway, and now those forests go up not in gentle ground fires but in the kind of towering, smoke-belching infernos that turn the sky orange over cities hundreds of miles away.
So here’s an idea that sounds slightly mad: to get less smoke, light more fires. A study published on 11 June in Science puts hard numbers on that bargain for the first time, and the numbers, roughly speaking, hold up.
The researchers behind it, Iván Higuera-Mendieta and Marshall Burke of Stanford’s Doerr School of Sustainability, were chasing a question that had nagged at fire policy for years. Everyone more or less agreed that prescribed burns, deliberate low-intensity fires set under careful conditions, could tame future wildfires. The trouble is they make smoke too. So you are being asked to pollute today on the promise of cleaner air later, and nobody had worked out whether that trade actually pays.
“Part of our wildfire problem, and the air quality problem it generates, is ironically the fact that we’ve been putting out fires for a long time,” says Burke, the study’s senior author.
A Paradox With a Price Tag
The snag was data, or rather the lack of it. The American West barely does prescribed burning at scale, averaging about 44,000 acres a year against more than 866,000 acres of wildfire. You cannot study something that has hardly happened. So the team reached for a clever stand-in: patches inside real wildfires that happened to burn at low severity, which look an awful lot like what a prescribed burn does to the land.
“It’s a chicken and egg thing,” says Higuera-Mendieta, the PhD student who led the work. “How do we study prescribed burning at scale? Well, what is it trying to replicate? It’s trying to replicate low-severity fire.”
From there it was a matter of grinding through two decades of satellite imagery, building severity maps for nearly 99% of every wildfire California reported between 2000 and 2021, more than a thousand fires in all, including the monstrous 2020 Creek Fire, then matching each scorched square kilometre against a statistically similar patch that hadn’t burned. The point was to ask a counterfactual question: what would have happened to this land if the fire had never touched it?
Benefits That Drift Downwind
The answer, in conifer forests at least, was striking. A single dose of low-severity fire cut the odds of a very severe wildfire returning to that spot by 92 percent, and the protection lingered for more than ten years. Even stranger, the benefit leaked outward. Land within two kilometres of a treated patch saw its own fire risk drop by something like 43%, with faint but real effects measurable as far as five kilometres away.
“You get large benefits in the place that you treated,” Higuera-Mendieta says. “You get benefits that are maybe half as big but pretty meaningful in the nearby places that you didn’t burn. And so those are sort of ‘for free’ from an air quality perspective, because you didn’t have to burn them.”
Plug all that into a simulation of California burning 500,000 acres of conifers a year, and the smoke ledger eventually tips. In the early going, when wildfires happen to be quiet, all that deliberate burning would have bumped smoke pollution up by roughly 50%. Not a great look. But the books balance by about year four, and over a full decade cumulative smoke falls by around 10 percent, with the biggest payoffs landing in catastrophic years like 2020 and 2021. Treat the land and weigh future smoke saved against smoke spent, and the benefits beat the costs by more than five to one.
Not every landscape plays along, mind you. In shrubland, the chaparral that covers much of southern California, the protective effect faded inside four years and never clearly stopped the worst fires. There, the researchers suggest, simply keeping fire out altogether might serve communities better than courting it.
There are caveats, and the authors are upfront about them. The study doesn’t tally the asthma attacks or heart problems or early deaths that shifting smoke around might prevent, though that work is now underway. It assumes a unit of prescribed smoke harms lungs exactly as much as a unit of wildfire smoke, which nobody has really proven. And it leaves out the plain financial cost of treatment, about $170 an acre, give or take, depending on terrain. The simulations also assume managers burn more or less blindly, scattering treatments across all 20 million acres of California conifer rather than targeting the spots most likely to ignite. Burke reckons smarter aim could only improve the math.
“On average, we estimate that each individual acre you treat has an impressive benefit-cost ratio, with the largest benefits in the worst wildfire years,” Burke says. The catch, he adds, is one of sheer scale: you have to treat an enormous amount of land to move the needle at all. California’s existing goal is already roughly 500,000 acres a year, four times what currently gets done. Whether the state can light that many fires on purpose, year after year, without one escaping into the next Creek Fire, is the question the spreadsheets can’t answer.
Frequently Asked Questions
How can lighting more fires possibly mean less smoke overall?
A controlled low-severity burn clears out the dead wood and brush that would otherwise feed a catastrophic blaze. That treated land then burns far less severely, or not at all, when a real wildfire arrives, and severe fires are what produce the truly enormous smoke plumes. You pay a small smoke cost now to dodge a much larger one later. In conifer forests the study found that trade pays off within about four years.
Does the benefit really reach land that was never burned?
Yes, and that was one of the more surprising findings. Fire risk dropped by roughly 43% in unburned areas within two kilometres of a treated patch, with weaker effects out to five kilometres. Past burns seem to act as temporary fuel breaks that slow the spread of later fires, so neighbouring land gets protection without anyone setting it alight.
Would this work everywhere in California?
No. The dramatic effects showed up in conifer forests, which blanket the Sierra Nevada and much of northern California. In shrubland and chaparral the protective effect faded within four years and didn’t reliably prevent severe fires, so the researchers suggest keeping fire out of those systems may be the wiser course.
What’s the biggest obstacle to actually doing this?
Scale, mostly. The benefit per acre is large, but California would need to treat around 500,000 acres a year, about four times the current rate, to meaningfully reduce statewide smoke. There’s also the financial cost, roughly $170 an acre, and the ever-present risk that a prescribed fire escapes its bounds, as happened with the 2022 Hermits Peak Fire in New Mexico.
Read more:
scienceblog.com/setting-cali…

4
2
27
1,946
Willowtreeceltic retweeted
Jun 13
Almost Everyone Drifts Counterclockwise When They Walk, and Nobody Knows Why | Ben Sullivan, ScienceBlog
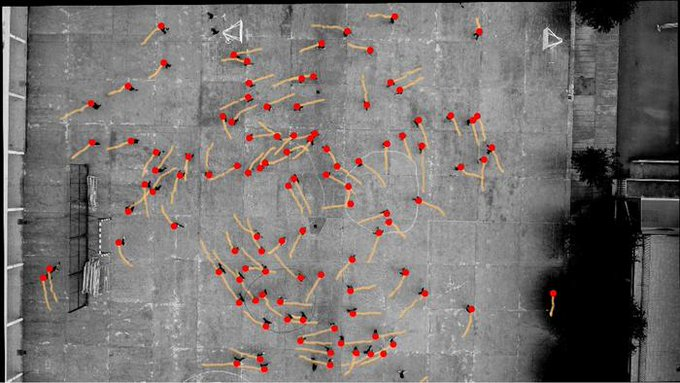
Thirty-two times out of thirty-three, the crowd turned the same way. Left. Always left, looping counterclockwise around the enclosure like water circling a drain, and the researchers watching the overhead footage hadn’t gone looking for any of it. They were trying to work out how to keep pandemic-era pedestrians two meters apart. What they found instead was a quiet, stubborn asymmetry buried in the way human beings move.
The team, working across Spain and Japan, had set up the usual sort of experiment: volunteers milling about inside a circular arena, cameras mounted overhead, software tracking every footstep. Social distancing was the goal. The spiral was an accident.
“When analyzing the experiments, my colleagues realized by chance, that in 32 out of 33 experimental trials, as people moved and turned, they noticeably preferred to turn counterclockwise,” says Claudio Feliciani, a project associate professor at the University of Tokyo who was eventually pulled into the puzzle from across the world. The numbers were hard to argue with. But numbers rarely explain themselves, and this is where the story gets genuinely odd.
Because the obvious explanations kept falling apart. You might reasonably assume people turn whichever way suits them in the moment, with no group-wide pattern at all. “This was completely unexpected as, at least instinctively, when people walk around randomly, you imagine people turn as their needs suit them with little sign of an overall preference,” says Feliciani. And yet. “There was a definite, measurable tendency for people to turn counterclockwise over clockwise, all things being equal.”
Ruling Out the Usual Suspects
Good practice, when you stumble onto something weird, is to attack it from every angle until something cracks. So that’s what they did, across five separate experimental campaigns. Culture was the first suspect, which is why the Japanese team got involved in the first place. In Spain, pedestrians passing one another tend to dodge to the right; in Japan, they drift left. Different countries, different ingrained habits. If avoidance manoeuvres were driving the spiral, the two nations should have spun in opposite directions.
They didn’t. Both went counterclockwise.
Then came the walls. Maybe the boundary of the arena was nudging people round, sort of like a marble in a bowl. So the researchers took over a hundred and seven teenagers out to a 50 by 60 metre schoolyard in Pamplona, an open space with effectively no boundary to push against, and watched them roam. The counterclockwise drift held. If anything it was cleaner. They ruled out handedness, footedness, eye dominance, sex, even group size: none of it made a meaningful dent. “It likely does not come from the eyes, because we tried to patch people’s left or the right eyes and the bias was still there,” says Feliciani. They also, gently, dismissed the more exotic theories that people kept proposing. “Some people asked us if it might be large-scale phenomena like the Coriolis force or Earth’s magnetic field, but this seems unlikely given what we have managed to point to so far.”
It Was Never a Crowd Thing
Here is the twist that reframes everything. For decades, the going assumption in crowd science has been that collective patterns, the lanes and waves and swirls you see in busy streets, emerge from people reacting to each other. The group is supposed to be more than the sum of its parts. But when the team finally sat over two hundred volunteers in an enclosure and had them walk completely alone, one at a time, the spiral didn’t vanish. The bias was right there in the solitary walker, statistically unmistakable (a Wilcoxon test put the odds of a fluke below one in a thousand). Which means the counterclockwise pull isn’t something a crowd conjures up together. Each of us, apparently, carries a faint leftward lean already, and a crowd just makes it visible.
The team even checked whether some unspoken social rule might be steering things, surveying 168 people about which way they’d expect to walk. If anything, the responses leaned the other way, toward clockwise, which is precisely the opposite of what everybody actually does. So much for politeness as an explanation.
The children are the loose thread worth tugging. In a Japanese nursery, five-year-olds set loose to run around during a music activity didn’t just drift counterclockwise, they committed to it, nearly the whole room wheeling in unison. “Of all these things, the only thing that stood out was that kids tend to have a stronger bias for the counterclockwise direction, so probably age plays a role in making the effect weaker or stronger,” says Feliciani. That hints the tendency is something we’re born with and slowly learn to override, rather than something we pick up.
So what is it? Nobody can say yet, and Feliciani is refreshingly blunt about that. The smart money is on something mechanical, baked into the body itself. “Our results may appear as a minor insignificant discovery, but in nature, most phenomena related to locomotion show that animals mostly walk without directional preference. The strong bias found in people hints to some asymmetry at the biomechanical level.” There are echoes elsewhere in the living world: ants that bear left when scouting new ground, budgerigars favouring one side through a gap, blindfolded people who, robbed of landmarks, spiral helplessly in circles thanks to some drift in their inner sense of straight-ahead.
The practical payoff could be real enough, mind you. Museums, airports, stadium forecourts, the great churning plazas of the world: design them to flow with the body’s natural lean rather than against it, and crowds might just move a little easier. Whether the bias survives the chaos of a genuinely crowded real-world space is still an open question. The next step is to zoom in on individuals and hunt for the biomechanical tell, which is fiddlier than it sounds.
Feliciani, for his part, can’t quite let go of one stray observation. “There are some interesting parallels to certain sports. Some running and driving competitions are always, but inexplicably, taken on courses that run counterclockwise.” Athletics tracks. Speed skating. Horse racing in much of the world. All of it spinning the same way we apparently want to walk. “But that’s an investigation for another time.”
Frequently Asked Questions
Do people really prefer to turn left when walking?
Yes, on average. Across five experiments in Spain and Japan, the vast majority of pedestrians showed a measurable tendency to drift counterclockwise, meaning they curved to their left, even when walking alone with no one to follow. The effect is subtle in any one person but consistent enough to show up reliably across crowds.
Is the counterclockwise bias caused by being right-handed?
Apparently not. The researchers tested handedness, footedness, and eye dominance, and none of them explained the drift. They even had volunteers walk with one eye patched and the bias stayed put. Whatever causes it sits deeper than these familiar markers of left-right asymmetry, and the precise origin is still unknown.
Why does it matter which way crowds turn?
Because crowd flow shapes how safely and comfortably we move through airports, stations, museums and public squares. If people share a built-in directional lean, planners could design circulation routes that work with it rather than against it, easing congestion. It also overturns a long-held assumption that such patterns emerge only from people reacting to one another.
Could the spin be down to Earth’s rotation or magnetic field?
Almost certainly not. People floated those ideas, but the researchers consider forces like the Coriolis effect or geomagnetism highly unlikely given the evidence. The bias shows up in single walkers indoors, points to something in human biomechanics, and seems strongest in young children, which fits an internal cause rather than a planetary one.
Read more:
scienceblog.com/almost-every…
7
1
29
4,259
Drake | Strategy retweeted
Jun 9
The Texting Flaw That Let Anyone With an Email Pose as Your Bank | Ben Sullivan, ScienceBlog
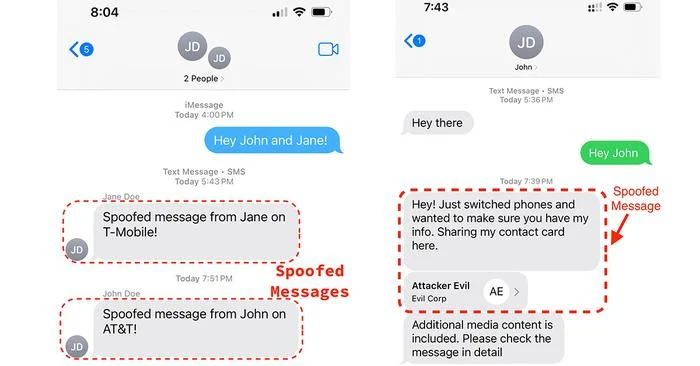
The message lands in the same thread where your bank always texts you. Same name at the top, same conversation you have scrolled through a hundred times, tucked right under last month’s fraud alert. It asks you to confirm a charge, and there is a link. Nothing about it looks off, because nothing about it is off, at least not in any way your phone is willing to show you. The sender is not your bank. The sender is someone with a laptop and an email account.
That uncomfortable scenario was, until very recently, trivially easy to pull off against most phones in the United States. A team of computer scientists at the University of California, San Diego spent months pulling apart the plumbing that carries text messages, and what they found was a gap wide enough to walk a convincing impersonation straight through.
The trouble starts with a feature almost nobody remembers asking for. Back in the early 2000s, carriers wanted to popularise texting, so they wired up gateways that let you send a text by emailing it. Email an address like a phone number at the carrier’s domain, and the message pops out the other end as an SMS. Convenient, sure. But email and text are different languages, with different rules about who sent what, and somebody has to translate between them.
That somebody is the gateway, and translation is where things get lost.
“Email and text messaging weren’t designed to work together,” says Stefan Savage, a professor in UC San Diego’s Department of Computer Science and Engineering and one of the paper’s senior authors. He reaches for an image to make the awkwardness concrete: “It’s a little bit like reading postcards to someone over the phone and needing to figure out where the sender and recipient information and the message itself are.”
And every carrier figures it out slightly differently. The team probed the gateways of the big U.S. networks, Verizon, T-Mobile, Google Fi, AT&T, and a clutch of smaller operators, treating each one as a black box and feeding it malformed email after malformed email to see what came out. Email systems do have anti-spoofing defences with names like SPF, DKIM and DMARC, and the gateways all claimed to support them. The problem was the seams. Leave one header empty here, slip a stray character there, and a message that should have been rejected sailed through wearing whatever sender name the attacker fancied.
How a Stray Character Becomes a Phone Number
The really clever part happens once that email-turned-text reaches the handset. Phones try to be helpful: they check the sender against your contacts and show you a friendly name instead of a string of digits. The researchers discovered that a carefully crafted email address could hijack that lookup. On an iPhone, an address beginning with a phone number followed by the characters “=?” gets chopped at exactly the wrong spot, and the bit left over is read as a genuine phone number. Android had its own version of the bug, where Google Messages saw an all-numeric email address, decided it must really be a number, and quietly stripped out the @ and the dot until it became one.
So an attacker does not just spoof some random email. They can make your phone believe a message came from a specific number, a five-digit short code, or even a plain word like the name of a bank.
What makes this genuinely nasty, rather than merely clever, is what phones do next. To keep your conversations tidy, messaging apps bundle everything from one contact into a single thread, whether it arrived by SMS, iMessage or anything else. Apple’s app is especially eager about this, the researchers found, merging messages across phone numbers and email addresses into one continuous conversation without flagging which channel each one came in on. Spoof the right identity and your forged message does not start a suspicious new thread. It drops into the middle of a real one. There is a small caveat for the attacker, mind you: they generally cannot see the replies, since those go to the real contact.
“There are no standards for converting emails to texts and that opens the door to all sorts of vulnerabilities,” says Sumanth Rao, the paper’s first author and a computer science PhD student at the Jacobs School of Engineering.
The technical requirements for an attacker are, frankly, depressingly modest. You need a computer that can send email, some fiddly off-the-shelf software, a domain of your own, and the victim’s phone number, which is hardly a state secret. From the number you can usually look up the carrier, and from the carrier you can look up the gateway, because the carriers publish the addresses themselves. The same researchers also showed how to dress a forged message up as a “verified” business, complete with a recognisable logo, and how to fake an entire group chat in which the attacker plays every part except the victim.
The Long Tail of a Twelve-Year-Old Bug
Some of this had been sitting in plain sight for an alarmingly long time. The iPhone parsing quirk appears in Apple’s libraries going back to at least 2012, and the Android one to around 2016. These were not freshly minted holes; they were old assumptions nobody had thought to stress-test.
The whole edifice, the researchers argue, rests on a quiet bit of faith that none of us agreed to. We assume a text is what it says it is. “People don’t realize that there’s no guarantee that text messages have integrity,” says Savage. “You can’t count on authenticity.”
Here is the better news. Before publishing, the team disclosed everything to the affected companies, and the response was unusually brisk. T-Mobile patched its gateways within a day of being told; Verizon within five. Google fixed the flaw in Google Messages and Apple fixed the iPhone parsing bug, assigning it a formal vulnerability identifier in the process. Verizon is going further and plans to switch off the ability to send texts by email altogether by the end of March 2027, a path AT&T had already taken. The industry’s standards body, the GSMA, is updating its security guidance so carriers elsewhere can tighten the same loose joints.
So the front door has been bolted, at least in the US. What the work really exposes, though, is less a single bug than a habit of building. Whenever two old systems that were never meant to talk are bolted together for convenience, the gaps in the translation become someone’s opportunity, and those gaps tend to lurk for years before anyone goes looking. The next one is probably already out there, waiting in the seam between two services nobody thought to question.
The research, “Lost in Translation: Text Message Spoofing via Email,” received a Distinguished Paper Award at the 47th IEEE Symposium on Security and Privacy.
Frequently Asked Questions
Could someone really fake a text from my bank without hacking anything?
Yes, and that was the unsettling core of this research. By emailing a carrier’s text gateway with a few deliberately malformed details, an attacker could make a phone display their message as coming from a trusted name or number, no account breach required. The major US carriers and both Apple and Google have since patched the specific flaws, but the technique worked against ordinary phones for years.
Why was a forged text able to slip into an existing conversation?
Messaging apps group everything from one contact into a single thread to keep things tidy, and they tend to trust the sender label without verifying it. Apple’s app was the most aggressive, merging messages across email and phone numbers into one conversation, so a spoofed message could appear mid-thread rather than starting a suspicious new one. That bundling is convenient, but it quietly assumes every sender is who they claim to be.
Is my phone safe now?
For the specific attacks in this study, largely yes, provided your phone is updated, since Apple, Google and the major carriers have deployed fixes. Verizon is even planning to retire email-to-text entirely by early 2027. The deeper lesson is harder to patch: similar translation gaps may exist wherever two incompatible systems have been stitched together.
How hard would this have been to actually carry out?
Surprisingly easy by the standards of serious attacks. It needed only a computer able to send email, some common software, a domain, and your phone number, which is rarely hard to find. That low barrier is exactly why the researchers treated it as urgent rather than theoretical.
scienceblog.com/the-texting-…
2
5
17
2,375
Ann Currie retweeted
Jun 8
Creatine May Wake Up the Immune Cells That Hunt Cancer | Ben Sullivan, ScienceBlog
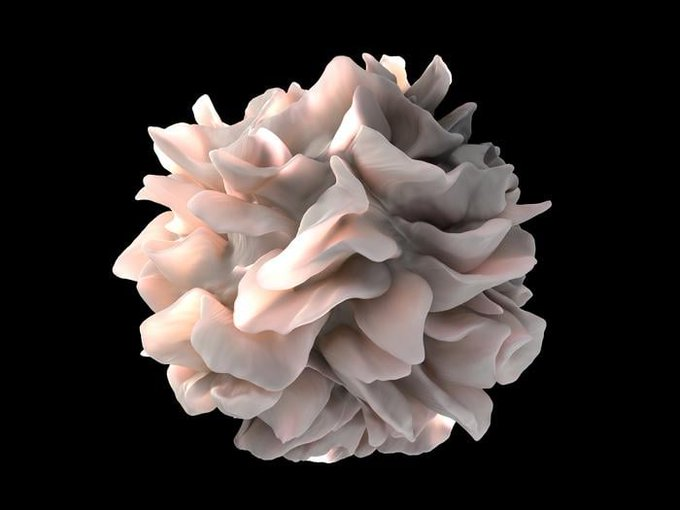
Inside a growing tumour, a dendritic cell is doing the most thankless job in the immune system. It grabs a scrap of the tumour, a telltale fragment, and carries it off to show the body’s killer T cells exactly what to attack. But it is working in hostile country. The tumour hoards nutrients, starves its neighbours, and the dendritic cell, running low on fuel, starts to flag. And a flagging dendritic cell raises a weak alarm.
What if you could keep that cell’s batteries charged? Researchers at UCLA think they have found a way, and it involves something startlingly mundane: creatine, the same white powder that athletes and bodybuilders have been scooping into their shakes for decades.
The study, published in April in iScience, builds on earlier work from the same lab showing creatine powers the killer T cells themselves. This time the team went looking one step upstream, at the cells that give those killers their orders. They started by reading which metabolic genes were busiest in dendritic cells that had pushed their way into mouse tumours. One stood out. The gene encoding the creatine transporter, the little protein that hauls creatine into a cell, was running far hotter inside tumours than in healthy tissue. The cells, it seemed, were already reaching for the stuff.
So the team took the transporter away. Dendritic cells engineered to lack it survived poorly, activated weakly, and made a feeble case to the T cells they were supposed to recruit.
Then they did the opposite. They gave mice with melanoma a daily dose of creatine, and the tumours grew more slowly. The treated animals had more of the potent antigen-presenting cells crowding into their tumours, and those cells were buzzing, churning out chemical signals that pull yet more immune reinforcements into the fight.
A battery for the immune system
Why should a muscle-building supplement do any of this? The answer is that creatine is, in a sense, a rechargeable battery. Inside the cell it shuttles high-energy phosphate back and forth, soaking up spare energy and releasing it on demand, keeping levels of ATP, the molecular currency that powers nearly everything a cell does, steady even when the surroundings turn lean. The metabolomics bore this out: creatine-fed dendritic cells held onto more ATP and kept their inflammatory machinery humming. Take the transporter away and that energy buffer collapses, and with it the signalling that tells a dendritic cell to switch on.
“Immunotherapy has shown remarkable promise, but it only works for a subset of patients,” says Lili Yang, the study’s senior author and a professor of microbiology, immunology and molecular genetics at UCLA. Most approved immunotherapies aim squarely at the killer T cells at the end of the chain, yet only roughly 20 to 40 per cent of patients respond. The thinking here is to support the whole apparatus instead, the cells that spot the threat and set everything in motion, not just the soldiers who finish the job.
“Understanding how to metabolically support dendritic cells is about supporting the entire anti-tumor response, not just the killer T cells at the end of it,” says Elliot Kang, a co-first author who worked on the study as an undergraduate in Yang’s lab.
From the gym to the clinic, maybe
The effect was not confined to mice. When the researchers treated human dendritic cells, the kind grown from blood and used to build dendritic cell cancer vaccines, creatine sharpened them up too, improving their ability to rouse human T cells against a cancer target. That hints at two rather different uses. “The potential we see here is that creatine could be used in two complementary ways: as a supplement to enhance the immune response of patients already receiving immunotherapy, and as a tool to improve the quality of dendritic cell-based vaccines before they’re administered,” says James Elsten-Brown, a co-first author and graduate student in the lab.
A note of caution, and the researchers are firm about it. This was done in cells and mice, not people. Nobody should be reading it as a reason to start dosing themselves mid-treatment, and anyone on cancer therapy should talk to their doctor before adding any supplement at all. There is a further wrinkle worth keeping in view: creatine is a ubiquitous energy metabolite, and a handful of studies suggest tumour cells can hijack it too, using it to fuel their own spread. The full picture, across immune cells and malignant ones alike, is not yet settled.
Still, creatine is cheap, and after decades of use in gym bags its safety profile is about as well documented as any supplement going. The team now hopes to work with physicians on trials that would test whether it actually helps patients on immunotherapy. The humble scoop of powder has had a long career building biceps. Its second act, it seems, might be fought somewhere far less visible, in the starved interior of a tumour, one tired immune cell at a time.
Frequently Asked Questions
How does creatine actually help fight cancer?
It does not attack tumours directly. Instead it acts as an energy buffer inside dendritic cells, the immune cells that identify a tumour and direct killer T cells to attack it. By keeping those cells supplied with ATP even in the nutrient-starved environment of a tumour, creatine helps them stay active and raise a stronger alarm, which in turn mounts a more aggressive T cell response.
Should people with cancer start taking creatine?
Not on the strength of this study. The work was done in cells and mice, not patients, and the researchers explicitly warn against drawing any medical conclusions from it. Anyone undergoing cancer treatment should consult their doctor before adding creatine or any other supplement, particularly since some research suggests tumour cells can also exploit creatine.
Why does immunotherapy only work for some patients?
Most approved immunotherapies target killer T cells directly, but only about 20 to 40 per cent of patients respond. One reason may be that the supporting cells that activate those T cells, including dendritic cells, are themselves worn down inside tumours. Energising that wider infrastructure, rather than the T cells alone, is the strategy this research points toward.
Could creatine improve cancer vaccines?
Possibly. Dendritic cell vaccines are made by growing a patient’s own dendritic cells in the lab, and these are the most common cells used in such platforms. Adding creatine during manufacturing boosted the activating power of human dendritic cells in the study, suggesting it might be used to make more potent vaccines, though this remains to be tested in clinical trials. You can read the full study in iScience .
scienceblog.com/creatine-may…
5
7
38
2,180
Jun 3
Weight-Loss Drug Semaglutide Slows Markers of Biological Aging in First Randomized Human Trial | Ben Sullivan, ScienceBlog
Inside the DNA of 84 adults living with HIV, something had shifted over eight months. Not the genetic code itself, but the chemical tags sitting on top of it, the molecular sticky notes that tell genes when to switch on and off. Half the group had spent the trial injecting themselves weekly with semaglutide, the same compound sold as Ozempic and Wegovy. And when researchers read those chemical tags at the end, the semaglutide group looked, by several biological measures, a little younger than they should have.
This is the first randomized, placebo-controlled human evidence that a GLP-1 drug might do more than shrink waistlines and steady blood sugar. It might also slow some of the molecular clockwork of aging.
The clocks in question are not the kind on your wall. They are statistical models, built from patterns of DNA methylation, those chemical marks that accumulate and rearrange as we get older. Feed a blood sample into one of these epigenetic clocks and it spits out a biological age, which can run ahead of or behind the number on your birth certificate. People with HIV tend to run ahead. Even when the virus is well controlled by antiretroviral therapy, their bodies often age faster than expected, which makes them, in a slightly grim way, a useful population for studying aging itself.
The data came from a trial that was never designed to ask this question. Its original goal was measuring fat around the abdomen.
Reading the Clocks
Researchers at the University of California San Diego and partner institutions went back to that finished trial, profiled DNA methylation in blood at the start and at week 32, and ran the numbers through a whole battery of clocks. The pattern that emerged was fairly consistent. Across measures tied to inflammation, blood, brain, heart, kidney, liver and metabolic health, the semaglutide group showed slower biological aging than the placebo group. On one widely used clock called DunedinPACE, which estimates how fast you are aging right now rather than how old you are, the pace dropped by about 9 per cent.
“We are not saying that semaglutide reverses aging or makes people younger,” said Michael Corley, an associate professor of medicine at UC San Diego School of Medicine and the Stein Institute for Research on Aging, who led the work. “What we are seeing is a signal that it may slow some of the biological processes associated with aging.”
Why would a diabetes-and-weight drug touch something as fundamental as aging? The leading explanation is unglamorous: inflammation and fat. Chronic immune activation is one of the main drivers of accelerated aging in people with HIV, and GLP-1 drugs tamp it down. They also strip away visceral and ectopic fat, the stuff that wraps around the abdomen and burrows into organs, which in turn quiets the inflammatory and metabolic signals that seem to push biological aging forward. But Corley suspects there is more going on under the bonnet. “Emerging data also suggest that GLP-1 drugs may reprogram certain cells in different organs, which could help explain why we see effects across multiple aging clocks,” he said. If that holds up, the drugs would be doing something rather deeper than simply melting fat.
The numbers in the published paper are striking on their own terms. PhenoAge slowed by nearly five years per year of follow-up; the mortality-linked PCGrimAge clock by around three; several others by smaller but statistically solid margins.
A Signal, Not a Verdict
A note of caution, though, and the authors are the first to raise it. This was a post hoc analysis, meaning the aging question was bolted on after the fact rather than planned from the start. The sample was modest, the cohort specific, the follow-up just 32 weeks.
It is also not the only hint pointing this way. A companion pilot study, published last month in npj Aging , followed people with HIV and fatty liver disease through 24 weeks of semaglutide. Roughly 42 per cent saw their pace of aging slow on DunedinPACE, and those same people lost more liver fat. About a third showed slowing on the mortality-risk clock. And in nearly half, the telomeres, the protective caps on the ends of chromosomes that fray with age, actually got longer; those participants tended to walk faster afterwards, a small but tangible sign of better physical function. Two studies, same direction of travel. That is the sort of thing that gets a field interested.
The obvious question is whether any of this matters for people who do not have HIV. Corley thinks it might. “Many of the biological processes we study in HIV are also central to aging in the general population,” he said, adding that because those processes show up earlier and more sharply in this community, it can help researchers spot interventions that improve healthspan for everyone. Whether the effect would be as pronounced in a healthier, slower-aging body is anyone’s guess for now. Larger trials will need to sort out dosing, how long the benefits last, and whether stacking the drug on top of better sleep, diet and exercise amplifies anything.
There is a whiff of irony here. A class of drugs currently famous for what it does to appearance may turn out to matter more for what it does invisibly, in the methylation patterns no mirror will ever show you. The Stein Institute is already talking about building individualized “aging dashboards” that track these clocks and let clinicians tune therapies to the specific machinery going wrong in a given patient. Whether semaglutide earns a permanent place on that dashboard, or gets eclipsed by the newer GLP-1 compounds now arriving, is exactly the question the next round of trials will have to answer.
...
Frequently Asked Questions
Does this mean Ozempic can make you age more slowly?
Not exactly, and the researchers are careful about the wording. In this trial semaglutide slowed several biological markers of aging in the blood, but slowing a molecular clock is not the same as proven longer or healthier life. It is an early signal worth chasing, not a verdict, and it has only been shown so far in a specific group of people living with HIV.
How can a drug change your biological age without changing your DNA?
The clocks used here do not read your genetic code; they read chemical marks called methylation that sit on top of it and shift with age, stress and inflammation. Semaglutide appears to nudge those marks toward a younger-looking pattern, probably by lowering inflammation and stripping away fat around the organs. Some researchers suspect it may also reprogram cells in various organs, which would explain why the effect showed up across so many different clocks.
Why study people with HIV to learn about aging?
People with well-controlled HIV often age faster biologically than expected, so the processes behind aging tend to appear earlier and more strongly in them. That makes the group a kind of accelerated test case, where an anti-aging effect is easier to detect over a short trial. Whether the same benefit carries over to healthier bodies is one of the big open questions the next trials aim to settle.
How solid is the evidence at this stage?
It is promising but preliminary. The main finding came from a post hoc analysis, meaning the aging question was added after a trial designed to study abdominal fat, with fewer than 90 participants and only 32 weeks of follow-up. A separate pilot study points the same way, which is encouraging, but larger trials built specifically to test aging are needed before anyone draws firm conclusions.
scienceblog.com/weight-loss-…

1
8
1,531
Jun 2
Why Fixing a Person’s Sleep Might Also Lift Their Depression | Ben Sullivan, ScienceBlog
The body of someone with chronic insomnia is, in a sense, always braced. Heart rate a touch high, mind refusing to idle, muscles never quite letting go, even at 3am when nothing is happening and nothing needs to. Sleep scientists have a name for this perpetual readiness: hyperarousal. And it now looks like the lever a self-guided app pulls when it quietly improves not just sleep, but mood and worry too.
That, at least, is what a new analysis of a German insomnia therapy suggests. The therapy is called somnovia, and the question the researchers asked was deceptively simple: when it works, what exactly is it fixing first?
Most trials would never answer that. They lump every symptom into a single score, tally it before and after, and report whether the number dropped. Useful, sure, but it flattens everything. Difficulty falling asleep and daytime exhaustion get treated as interchangeable, even though they are clearly different beasts that may respond to treatment at quite different speeds. Linda Betz and her colleagues wanted to pull that lump apart.
So they went back to a completed randomized trial of 290 adults with chronic insomnia, roughly three-quarters of them women, average age around 50. Half had used somnovia on top of their usual care; half had usual care alone.
Then they ran something called network intervention analysis. Rather than a single before-and-after number, the method maps each individual symptom, sleep complaints, depressive symptoms, anxiety symptoms, as a node in a web, with the lines between them showing which symptoms move together. Crucially, it can also show which symptoms the treatment touches directly, and which only shift because their neighbours did.
The picture at three months was strikingly narrow. somnovia was tugging hardest on a small cluster: difficulty relaxing, dissatisfaction with sleep, worry about sleep, and to a lesser degree a kind of restless physical agitation. Everything else, the better mood, the lower anxiety, seemed to come along indirectly, downstream of those few.
The Knot Beneath the Sleeplessness
What links that cluster is arousal. Not the racy kind, the clinical kind. Worry about sleep and dissatisfaction with it are the cognitive, churning end of the spectrum; the difficulty relaxing and the bodily restlessness sit at the physiological end. somnovia, which delivers the standard toolkit of cognitive behavioural therapy for insomnia (sleep restriction, stimulus control, relaxation work, and techniques for interrupting the 2am spiral of catastrophic thoughts) appears to lean on both ends at once. The effect, as Betz puts it, is that the programme primarily targets a central transdiagnostic process: hyperarousal . Loosen that, and the vicious loop of frustration and vigilance that keeps insomnia spinning starts, perhaps, to slacken.
Then time did something interesting. By six months, the tidy little cluster had spread.
The treatment’s fingerprints were now smudged across the wider network, reaching fatigue, excessive worry, appetite. Dissatisfaction with sleep and sleep-related worry were still the strongest links, but the influence had diffused outward. The researchers read this not as the therapy fading but as its benefit becoming embedded, soaking into the whole symptom system rather than sitting on a few complaints. As they describe it, the early gains in core arousal symptoms ripple along the connections to their neighbours, and the neighbours’ neighbours, until the improvement is everywhere and nowhere in particular.
One Lever, Many Symptoms
Here is why that matters well beyond a single app. Insomnia is not just an unpleasant thing in its own right; it is a known predictor of depression and anxiety, a thread running through dozens of mental health conditions. If hyperarousal really is the shared upstream knot, then untangling it early, with something as cheap and scalable as a website, could in principle head off trouble that would otherwise surface later as something darker. That is a big “if,” and worth keeping in view. The depression and anxiety effects here were knock-on, not direct, and some of the later, weaker links in the network were a bit wobbly, the kind of finding that wants replicating before anyone gets carried away.
One more thing worth flagging: somnovia is made by GAIA, the company that also funded this work and pays two of the authors. It is already prescribable in Germany, listed in the national directory of digital health apps, with the cost picked up by statutory insurers, which makes the question of how, and how well, it actually works rather more than academic. The next step is teasing apart which bits of the programme do the loosening, and whether the same upstream-knot logic holds for other digital therapies built on the same bones.
For now, the takeaway is quietly radical. Treat the sleep, and you may be treating a good deal more than the sleep.
...
Frequently Asked Questions
Why would an insomnia app affect depression and anxiety at all?
Because the three conditions appear to share an underlying driver: hyperarousal, a state of being mentally and physically over-keyed. The analysis suggests that when the therapy calms that arousal to help with sleep, the benefit travels along to connected symptoms of low mood and worry over time, rather than the app treating depression head-on. It is sleep as an upstream lever, not a cure-all.
How does network intervention analysis actually work?
Instead of collapsing all of a person’s symptoms into one score, it treats each symptom as a point in a web and maps which ones move together and which the treatment touches first. That lets researchers separate symptoms changed directly by the therapy from those that only improve because a connected symptom got better. It is a way of seeing the order in which recovery unfolds.
Is a self-guided app really as good as seeing a therapist for insomnia?
Meta-analyses suggest digital cognitive behavioural therapy for insomnia reaches efficacy broadly comparable to face-to-face treatment, which matters because trained therapists are in short supply and waiting lists are long. somnovia is fully self-guided, with no therapist contact, and most users in the trial finished the whole programme. Whether it suits everyone is a separate question worth asking your doctor.
Should I trust a study funded by the company that sells the product?
It is a fair flag. The developer funded the work and employs two authors, which is disclosed, and the underlying trial was randomized and registered in advance, which tightens the case. Still, independent replication is the thing that would settle it, and that has not happened yet.
scienceblog.com/why-fixing-a…

4
1
11
5,174
May 30
Urine Test Can Identify Most Children With Autism by Reading Their Gut Bacteria | Ben Sullivan, ScienceBlog
Deep in the gut of a two-year-old, bacteria are doing something they were not quite supposed to do. Working on amino acids drawn from whatever the child has eaten, communities of microbes convert tryptophan and phenylalanine into molecules that look, structurally, quite a lot like serotonin and dopamine. Not the real thing. Distorted versions, chemically adjacent, that travel through the bloodstream and cross into the brain. In children with autism, these metabolites are present at concentrations that would be unremarkable if they were a little elevated. They are not a little elevated. In some cases they are a thousand times higher than anything seen in typically developing children of the same age.
That single biological fact has now been turned into a screening test, one that requires nothing more invasive than a urine sample. And it may be able to flag which young children are at high risk for autism before a clinician has formally assessed them.
The research, published in Molecular Psychiatry , comes from Arizona State University’s Biodesign Center for Health Through Microbiomes, where James Adams has spent roughly fifteen years building a case that the gut microbiome is doing something important in autism spectrum disorder. The study measured concentrations of seventeen microbially derived metabolites in urine samples from 52 children with autism and 47 typically developing children, all between the ages of two and eleven, recruited at four sites across the United States. What the team found was not subtle: nearly every child with autism had at least one metabolite exceeding the highest level observed in any control child. The average child with autism had three elevated metabolites. The control children had none.
What the Bacteria Are Making
The metabolites fall into three broad categories: those derived from phenylalanine and tyrosine, those derived from tryptophan, and those associated with yeast and fungal overgrowth. The first two groups are the most conceptually striking. Tryptophan is a precursor to serotonin and melatonin. Phenylalanine feeds into dopamine synthesis. When gut bacteria process these amino acids, they produce metabolites that compete with, mimic, or interfere with the neurotransmitter pathways that those amino acids would otherwise supply.
“What’s really striking about the bacteria is that they make metabolites that are basically altered versions of serotonin and dopamine,” said Adams, who is a President’s Professor at ASU and a corresponding author on the study. He argues these compounds could explain quite a lot about the behavioral and cognitive profile of autism: the social communication difficulties, the anxiety, the attention problems, the mood instability. Whether the metabolites are a cause or a downstream consequence of a disrupted gut microbiome is not something this study can resolve. But the association, across more than 40 prior studies measuring individual metabolites, is consistent enough that Adams’s team is now fairly confident the connection is real.
The best-studied of these compounds is p-cresol sulfate, a molecule produced from phenylalanine or tyrosine by more than sixty gut bacterial species. It has been found elevated in children with autism compared to controls in 17 of 17 independent studies; in animal models, administering p-cresol produces autistic-like behaviors, and fecal transplants from healthy animals reverse the effect. That kind of cross-species consistency is not something researchers see every day.
The Test Itself
The diagnostic tool the team has developed, called the MDM System, works as a scoring method rather than a single-biomarker test. For each of seventeen metabolites, the system checks whether the child’s urine concentration exceeds the reference range established from typically developing children. Each metabolite above that threshold adds a point. A score of one or more means the child has at least one extremely elevated microbial metabolite; in this study, that threshold caught 90% of the autism group and misidentified none of the controls. Sensitivity of 90%, specificity of 100%. Those are, to put it plainly, unusually strong numbers for a screening test, though the researchers are cautious about the moderate sample size and are running a replication cohort.
Christina Flynn, the first author and now research director of ASU’s newly launched autism diagnostics laboratory, has been working on this since her doctoral research in chemical engineering. She is also the parent of a child with autism. “What we’ve discovered is that 80 to 90% of children with autism have extremely high levels of one or more microbially derived metabolites,” she said. Beyond the diagnostic number, she is interested in what a biological test might do for families who have been waiting. Autism is currently diagnosed through behavioral observation, which requires a specialist clinician, and the average age of first diagnostic assessment in the United States is 47 months, nearly four years old. For families who suspect something earlier, that wait is substantial.
Flynn talks about families spending months, sometimes years, not knowing what they are dealing with. “If this test shortens that gap, even by a little, that’s meaningful because earlier intervention can really help,” she said. She has also noted that parents sometimes delay seeking diagnosis because they worry they will be judged, that it will look like a parenting failure. A urine test that points to gut chemistry, she thinks, could reframe that entirely.
A New Phenotype, and What Comes Next
Based on their finding that roughly nine in ten children with autism in the study had elevated metabolites, the team has proposed a new clinical phenotype: ASD associated with Microbially-Derived Metabolites, or ASD-MDM. The roughly 10% of children with autism who showed no elevated metabolites in urine were not simply normal across the board; most of them had other significant metabolic anomalies, in some cases suggesting possible inborn metabolic errors that may have independently produced autistic features. The implication is that ASD-MDM might define the large majority of autism cases, with a biologically distinct minority group underneath.
The test is already commercially available through Analutos, a UK laboratory that performed the quantitative analysis for the study and now offers the test internationally from samples shipped to them. Rosa Krajmalnik-Brown, director of the Biodesign Center and a co-author, has been pursuing the gut-autism connection for over fifteen years. “I am excited about the MDM test, which includes important microbial metabolites, previously hypothesized to be linked with autism,” she said. For her, the test represents a way to make a biological hypothesis operational in a clinical setting, something that has proved difficult to do in this field.
Whether the metabolites can also serve as therapeutic targets is the question that follows naturally, and the one the team is most cautious about. A prior open-label trial of microbiota transplant therapy found substantial reductions in p-cresol sulfate alongside meaningful improvements in gut and behavioral symptoms, but that study was not controlled, and the field is not at the point where anyone should be recommending transplant therapy as routine. Still, if a urine test can tell you which metabolites are elevated in a specific child, and if future trials demonstrate that reducing those metabolites improves outcomes, the path toward personalized gut-targeted intervention for autism starts to look at least plausible.
For now, the urine test is a screening tool, not a diagnosis. A positive result means a child should move to the front of the queue for formal evaluation, not that the evaluation can be skipped. But in a system where waiting lists for pediatric developmental assessments can stretch for years, moving to the front of the queue is not a small thing.
Frequently Asked Questions
How does a urine test detect autism if autism is a brain condition?
The test doesn’t measure anything in the brain directly. It detects metabolites produced by gut bacteria that appear to influence brain chemistry by mimicking or disrupting the pathways that produce serotonin and dopamine. In children with autism, these metabolites were found at concentrations up to a thousand times higher than in typically developing children, suggesting the gut microbiome is behaving very differently. The gut-brain axis, the chemical signaling pathway between the digestive system and the nervous system, is increasingly understood to play a significant role in neurodevelopmental conditions.
Does this mean autism is caused by gut bacteria?
Not necessarily, and the researchers are careful to say so. The study demonstrates a strong and consistent association between elevated gut metabolites and autism spectrum disorder, backed by over 40 prior studies finding similar patterns. But whether the disrupted microbiome is a cause of autism, a consequence of it, or something that worsens symptoms without causing the condition in the first place remains an open question. What the findings do suggest is that gut biology is involved in the majority of cases, which opens up new possibilities for both screening and treatment.
Could a child test positive on this and not have autism?
In the study sample, none of the typically developing children had even one metabolite above the reference range, giving the test 100% specificity, meaning no false positives among controls. That said, the sample size was moderate at 99 children total, and the researchers stress that a positive result should prompt formal clinical evaluation rather than replace it. The test is designed as a triage tool to help prioritize which children see a specialist sooner, not as a standalone diagnosis.
What’s stopping this from being used widely right now?
The test is already commercially available through a UK laboratory called Analutos, which accepts samples from anywhere in the world. The main obstacles are awareness and replication: this is a pilot study and a larger independent cohort needs to confirm the findings before most clinical guidelines would recommend it. There are also open questions about whether the reference ranges hold across more diverse populations, very young infants, and teenagers or adults, since the study focused on children aged two to eleven.
If gut metabolites are the problem, could fixing the gut microbiome improve autism symptoms?
Preliminary evidence suggests it might in some cases. An earlier open-label trial of microbiota transplant therapy found substantial reductions in p-cresol sulfate, one of the key metabolites measured in this study, alongside improvements in gastrointestinal and behavioral symptoms. The researchers are far from recommending it as standard care; the trial wasn’t controlled, and more rigorous studies are still needed. But the possibility that personalized gut-targeted therapies could reduce symptom severity is one of the more concrete therapeutic directions this line of research is pointing toward.
scienceblog.com/urine-test-c…

3
7
34
2,302
May 30
Pandemic Loan Fraud Helped Push Up US House Prices, and Ordinary Buyers Paid for It | Ben Sullivan, ScienceBlog
Follow the money far enough and it ends up somewhere physical. A car. A furniture order. A house. When economists at the University of Texas at Austin went looking for what happened to the billions stolen from America’s pandemic relief programs, that is roughly where the trail led: into driveways and onto deeds. Stolen public money, it turns out, does not just vanish into someone’s account. It goes shopping.
And when it went shopping for houses, it left a mark on the price everyone else paid.
That is the uncomfortable finding from John Griffin, Samuel Kruger and doctoral student Prateek Mahajan, whose paper is forthcoming in the Journal of Financial Economics. The trio had already spent years picking apart fraud in the Paycheck Protection Program, the $793 billion scheme rushed out in 2020 to keep small businesses alive. Their earlier work flagged tens of billions in suspicious loans, the kind of number that gets you cited by a congressional committee. This time they asked a different question. Not how much was stolen, but what the theft did to the rest of us.
The answer is a bit grim if you bought a home in the wrong place at the wrong time.
Following the Stolen Money Into the Housing Market
Working through property records for 18,761 ZIP codes, covering 93 percent of the US population, the team matched a random sample of 250,000 PPP recipients against who was buying houses and when. People who took flagged, likely-fraudulent loans were 17% more likely to buy a home than recipients whose loans looked clean. They moved more, too. And because this particular flavour of fraud clustered, spreading along social networks until some neighbourhoods had upwards of 40 per cent of their loans flagged as dodgy, all that sudden buying power landed in the same places at once.
“That’s where real people get hurt by this,” says Kruger. “If you’re just a regular homeowner, and you happen to purchase in one of those areas in 2021 or 2022, you probably purchased at an inflated price. As that excess demand comes off the market, you’re going to expect to lose money on the house.”
Here is the part that ought to give policymakers pause. The researchers compared house price growth across ZIP codes inside the same county, so they could strip out the obvious macro stuff, interest rates, the general post-2020 mania. ZIP codes in the top tier of suspicious lending saw prices climb 5.8 percentage points more than those in the bottom tier. That sounds modest until you scale it: it accounts for roughly 22.5% of the average price surge during 2020 and 2021. Run a horse race among all the usual suspects, remote work, migration out of cities, the teleworkable office job, prior price momentum, and fraud comes out as one of the two strongest predictors, neck and neck with plain old lack of available land. Legitimate PPP money, the loans that did what they were meant to do, had no measurable effect on prices at all. Which makes sense. That cash was plugging holes, not chasing real estate.
The distortion was worse exactly where you would least want it. In tight markets, places where you cannot just throw up more houses to soak up demand, the effect was over 30% stronger.
None of this means fraud was the whole story; migration and remote work were real and the authors are careful to say so. But fraud was bigger than either, which almost nobody saw coming.
Why Dirty Money Moves Prices and Clean Money Doesn’t
What lifts this out of the usual fraud-accounting exercise is the idea underneath it. Economists have long suspected that fraud carries costs beyond the stolen sum, a notion that goes back to George Akerlof and Paul Romer in the early 1990s. A normal government transfer, a stimulus cheque say, is spread thinly and proportionally and mostly offsets lost income. A fraudulent one behaves differently: it is a windfall, concentrated, and the sort of person willing to commit fraud is perhaps not the sort to tuck it away in savings. So it gets spent, fast, on cars (auto registrations ticked up measurably in high-fraud areas), on furniture, on restaurant meals, and on houses. And spending that is bunched up in space and time is exactly what moves a local price. The effect even shows up later in regional inflation figures, lingering into 2023.
“It hurt individuals who bought houses at inflated prices,” says Griffin. “Fraud can have large unintended consequences.”
There is a sting in the tail, literally. After June 2022, the high-fraud areas turned around and underperformed, clawing back about a third of those earlier gains as the fake demand drained away. So the regular buyer who bought near the peak got it from both ends: an inflated purchase price, then a softer market to sell into. Heads you lose, tails you lose.
Griffin, who knows his financial history, points to an unsettling precedent. The 2008-09 crash was fuelled in part by inflated home prices that eventually cracked, taking the banking system with them. He is not predicting a repeat, exactly. But fraud-fuelled price bubbles have form.
The researchers’ verdict is less a warning than a design note for next time, and there will be a next time, because there is always another emergency and another firehose of relief money. “Our findings show fraudulent transfers can be wealth shocks that generate economic distortions not created by normal transfers,” Kruger says. “Future government program designs should take more proactive steps to prevent fraud on the front end.” Build the locks before you fill the vault, in other words. The PPP was designed for speed, and speed is what it delivered, to everyone, including the thieves.
doi.org/10.1016/j.jfineco.20…
Frequently Asked Questions
How could loan fraud actually push up the price of a house down the street?
Stolen relief money behaved like a sudden windfall rather than a top-up for lost income, so recipients spent it fast, and a chunk went on homes. Because this fraud clustered in particular neighbourhoods, the extra buyers piled into the same local markets at the same time, and concentrated demand is exactly what nudges prices upward. The effect was strongest in tight markets where supply could not stretch to meet it.
Is it true that the fraud mattered more than remote work or migration?
According to the study, yes, at least within the comparison it ran. When the researchers pitted all the leading explanations against each other in the same statistical model, suspicious lending came out as one of the two strongest predictors of price growth, rivalling a simple shortage of land. Remote work and migration were real, but smaller once everything was weighed together.
If I bought a home in one of these areas, did I lose money?
Possibly, if the timing was unlucky. High-fraud areas saw inflated prices through mid-2022, then underperformed afterwards as the artificial demand drained away, clawing back roughly a third of the earlier gains. A buyer near the peak could have paid too much and then watched the local market soften, a double hit the researchers describe in detail.
Could this happen again with the next round of emergency relief?
The researchers think it could, which is rather the point of their warning. Programs built for speed, like the 2020 Paycheck Protection Program, tend to skimp on fraud safeguards, and the next national emergency will bring another flood of fast money. Their suggestion is to design those defences in from the start rather than chasing the losses afterwards.
scienceblog.com/pandemic-loa…

2
2
26
1,563
May 21
A Pill That Keeps Your Throat Awake Could Transform Sleep Apnea Treatment | Ben Sullivan, ScienceBlog
The moment you fall asleep, your throat starts forgetting what it’s supposed to do. Not all at once. It’s a gradual withdrawal, a quieting of the neural signals that spend every waking hour keeping the muscles of your upper airway taut and open. In people with obstructive sleep apnea, that nightly retreat goes too far. The airway sags. It collapses. Breathing stops, the brain fires off an alarm, you half-rouse without knowing it, and then the whole cycle begins again, dozens, sometimes hundreds of times a night.
For decades, the only real answer was a machine. The continuous positive airway pressure device, or CPAP, essentially splints the airway open with a stream of pressurised air delivered through a mask strapped to the face. It works, when people use it. Many don’t. They find the mask claustrophobic, or the noise intolerable, or they simply wake one morning and decide they’ve had enough. By some estimates nearly half of patients abandon CPAP within a year. And that matters, because obstructive sleep apnea affects something like a billion people globally, raising their risk of heart disease, stroke, cognitive decline, and early death, mostly through the cumulative oxygen deprivation that comes with a night’s worth of interrupted breathing.
So the question researchers have been circling for years is a deceptively simple one: could you take a pill instead?
Targeting the Root Cause
A large phase 3 clinical trial presented this week at the American Thoracic Society’s international conference suggests, for perhaps the first time in a convincing and scalable way, that the answer might be yes. The drug is called AD109, and what makes it unusual is that it doesn’t treat the symptoms of sleep apnea so much as go after the underlying machinery of why the airway collapses in the first place.
The mechanism, worked out over decades of painstaking neuroscience in animal models, centres on a structure deep in the brainstem called the hypoglossal motor nucleus, the neural hub that controls the tongue and surrounding muscles keeping the throat open. During wakefulness, this nucleus receives a steady stream of excitatory input, particularly from the noradrenergic system. At sleep onset, that excitatory drive falls away. In REM sleep, a second inhibitory mechanism kicks in via muscarinic receptors linked to potassium channels, suppressing motor activity even further. The airway, deprived of its neural scaffolding, is left to fend for itself against gravity and anatomy.
AD109 is designed to counteract both mechanisms simultaneously. One component, atomoxetine, is a norepinephrine reuptake inhibitor (familiar from its use in ADHD) that boosts the excitatory noradrenergic drive to the motor neurons. The other, aroxybutynin, is a selective antimuscarinic that blocks the REM-related inhibitory pathway. Together, in theory, they keep the throat’s muscles somewhat more awake than the rest of you.
The SynAIRgy trial enrolled 646 adults across 69 centres in the US and Canada, all of them diagnosed with mild to severe obstructive sleep apnea and all of them either unwilling or unable to tolerate CPAP. They were randomised to AD109 or placebo for six months. The results, simultaneously published in the American Journal of Respiratory and Critical Care Medicine, showed a model-estimated 44 percent reduction in breathing interruptions per hour among those taking the drug, compared with about 18 percent in the placebo group. More than 40 percent of patients improved their disease severity category, and roughly 18 percent achieved what the trial classified as complete disease control.
Not a Cure, but Perhaps Enough
Patrick Strollo, a sleep medicine physician at the University of Pittsburgh Medical Center and the trial’s first author, framed the findings in terms of what he described as a troubling double standard in chronic disease care. “In many other chronic diseases, such as cardiovascular disease, asthma, or type 2 diabetes, it would be unthinkable for the majority of diagnosed patients to remain untreated or undertreated. Yet that remains the reality in OSA,” he said. “An oral pill that targets the underlying neuromuscular drivers of airway collapse during sleep could help address this gap and broaden the range of effective options for patients who remain untreated today.”
It’s worth dwelling on the numbers a bit before getting swept up in the optimism, though. AD109 isn’t doing what CPAP does. CPAP, when used properly, can bring breathing interruptions close to zero. The drug shifted the median patient from the moderate severity range down into mild (meaningful, perhaps, in terms of long-term cardiovascular risk, but not elimination). And about one in five patients discontinued the drug because of side effects: dry mouth, insomnia, nausea, urinary hesitation, all predictable from the pharmacology. The REM-suppressing effects of atomoxetine, in particular, raise questions about long-term sleep architecture that haven’t yet been answered. Small increases in heart rate and blood pressure were also recorded, which could matter for patients with underlying cardiac conditions.
Still, a companion mechanistic review published simultaneously in the American Journal of Respiratory Cell and Molecular Biology makes a case that the improvement in oxygen levels: specifically in what researchers call hypoxic burden, a measure of how deeply and for how long blood oxygen falls during sleep. That metric may translate into real cardiovascular protection over time. That metric has been more strongly linked to heart disease outcomes than the standard count of breathing interruptions, and AD109 reduced it by nearly 45 percent in the trial’s intent-to-treat analysis.
“These results provide encouraging evidence that targeting neuromuscular dysfunction can translate into meaningful clinical outcomes, aligning with our evolving understanding of the disease biology,” Strollo said.
A More Personalised Future
The drug’s manufacturer, Apnimed, has submitted a New Drug Application to the FDA. Under a Fast Track designation, a decision is expected by early 2027. If approved, AD109 would be only the second pharmacological therapy ever cleared specifically for obstructive sleep apnea; tirzepatide, a GLP-1 receptor agonist originally developed for diabetes, gained approval last year primarily for obese patients by reducing the weight pressing down on the airway.
AD109 works rather differently, and in a population that includes plenty of people who aren’t obese (a third of the SynAIRgy participants had a normal or overweight BMI). That’s important because OSA has long been misunderstood as primarily a disease of the overweight middle-aged man. Recent epidemiology has corrected that picture substantially: the condition is broadly distributed across sexes, body types, and ages, with the neuromuscular dysfunction at its core present to some degree in virtually all sufferers.
The researchers are already thinking about combinations. Patients with a strong anatomical component might do best pairing AD109 with a GLP-1 drug to reduce airway crowding from excess tissue. Those with ventilatory instability (where the breathing control system itself oscillates too easily) might benefit from adding sulthiame, a carbonic anhydrase inhibitor in phase 2 trials that targets that particular trait. The vision, in other words, is a field that stops giving everyone the same mask and starts asking which mechanism, or combination of mechanisms, is most to blame in each individual patient.
That’s perhaps where the real significance of this week’s results sits. Not in a single drug’s modest effect sizes, but in the confirmation that the neuromuscular machinery controlling the sleeping throat is, as one mechanistic review puts it, a tractable therapeutic target. The brain tells your throat to stay open. During sleep, it gets quieter. Now there’s evidence that pharmacology can turn the volume back up.
Read more:
scienceblog.com/a-pill-that-…
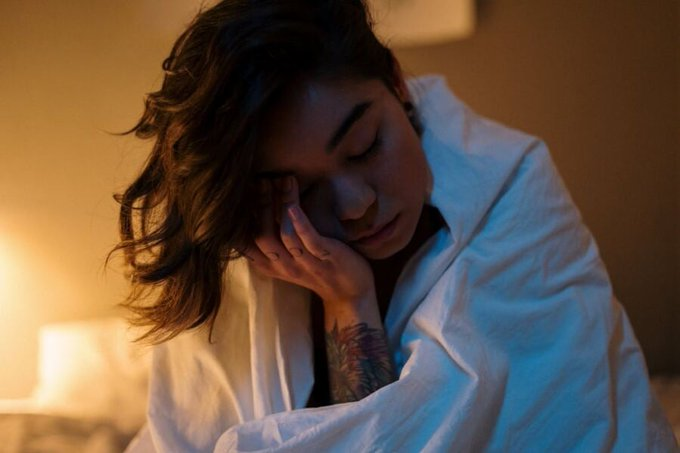
12
1,478
May 15
Nonprofit Hospitals Have Spent $7.8 Billion on Management Consultants. Nobody Can Find Any Benefit. | Ben Sullivan, ScienceBlog
For any hospital chief executive watching the balance sheet erode, the pitch from a management consulting firm must be hard to resist. Here, the partners promise, are people who have seen every operational failure, every cost spiral, every revenue leak in the industry, people who can fix things (in a matter of months, they promise) what internal staff have struggled with for years. The consultants arrive with laptops and frameworks. They run workshops. They deliver decks. They leave with very large cheques. And according to the most rigorous study ever conducted on the practice, they leave hospitals almost exactly as they found them.
A paper published this week in JAMA has done what a remarkable number of people apparently did not think to do: it actually looked at the numbers.
Joseph Dov Bruch, a health policy researcher at the University of Chicago, had a practical reason to want an answer. Students coming through his programme kept asking him whether a career in healthcare management consulting was a meaningful way to improve the system. He found, to his frustration, that he had no good evidence either way. So he and his colleagues went looking. They combed through IRS Form 990 filings, the detailed financial disclosures nonprofits are required to submit each year, and used machine learning to identify hospital contracts with management consulting firms across a twelve-year period. What they found was, depending on your perspective, either entirely unsurprising or quite extraordinary.
A $7.8 Billion Shrug
More than one in five American nonprofit hospitals hired a management consultant at some point between 2010 and 2022. Across the sector, the total bill came to at least $7.8 billion over roughly a decade, with the average hospital paying $15.7 million for its engagement. That is money that might otherwise have gone toward patient care, capital improvements, or the community health programmes that nonprofit status is nominally supposed to encourage.
The researchers compared 306 hospitals that initiated their first consulting contract during the study period against 513 carefully matched hospitals that did not, then tracked both groups across a battery of financial, operational, and clinical metrics. Net patient revenue. Operating margins. Days of cash on hand. Inpatient length of stay. Staffing levels. Executive compensation. Thirty-day mortality and readmission rates for heart attacks, pneumonia, and stroke.
Across virtually every measure, the result was the same: nothing. No statistically significant, systematic improvement attributable to the consulting engagement. Operating margins didn’t meaningfully shift. Revenue didn’t climb. Hospitals didn’t become leaner or more efficient. “It’s not necessarily a waste,” Bruch said, “but we don’t have evidence of meaningful improvements.”
The one exception was small and unwelcome: a modest increase in thirty-day readmissions among stroke patients. It was statistically significant, just barely, but the researchers note it was not robust when they tested alternative model specifications, so it is probably noise. Still. Not the direction you would hope for.
Why the Evidence Gap Lasted This Long
What makes the study genuinely odd, in retrospect, is how long it took for someone to do it. Management consultants have been a fixture of American healthcare for decades, wielding influence that Bruch’s paper notes is higher than in almost any other sector of the economy. Hospitals have been handing over billions in tax-subsidized dollars to these firms throughout a period when American healthcare was under intense political scrutiny for its costs and outcomes. And yet, as Bruch’s team documents, there was no prior large-scale empirical attempt to measure what hospitals actually got in return.
Part of the explanation is practical: the data didn’t exist in a usable form until someone went digging through IRS filings with machine learning. Part of it may be something a bit more awkward. Management consulting is a diffuse, relationship-dependent industry where firms rarely publicize detailed records of what they recommended or why, and hospitals are disinclined to trumpet the cases where advice didn’t pan out. The whole arrangement runs on reputation and trust rather than documented outcomes, which is an unusual posture for an industry advising organizations whose core mission is evidence-based medicine.
Bruch is measured in his conclusions. “This initial analysis suggests that consultants may deliver neither the dramatic efficiencies they promise nor the harms that critics sometimes fear,” he said. The framing matters: he is not claiming consultants are useless, only that the evidence of usefulness is, so far, absent. It is possible, he acknowledges, that consulting engagements affect things the study couldn’t capture, or that benefits take longer to materialize than the study window allows, or that some hospitals gain and others lose in ways that cancel out in aggregate. But the null result, across this many hospitals and this many metrics, is hard to dismiss.
What the Numbers Don’t Capture
The paper’s scope is also deliberately narrow: it looked only at management consultants, defined specifically, not the broader ecosystem of external expertise that hospitals buy. When the researchers widened the definition to include HR and IT consultants, total spending by nonprofit hospitals over the study period climbed past $25 billion. That figure raises the obvious question of whether similar analyses of those adjacent industries would yield similar shrugs, and Bruch thinks it probably should prompt someone to look.
There is also the question of what “meaningful improvement” would even look like in a system as complex as an American hospital. Consulting firms typically frame their value in terms of strategic alignment, organizational culture change, and positioning for future growth: outcomes almost definitionally resistant to measurement in Bruch’s study timeframe. Whether that resistance to measurement is a genuine feature of complex organizational change, or a convenient property for an industry whose outputs are hard to audit, is a question the data cannot answer.
What the data can say is that $7.8 billion bought no detectable improvement in any metric that hospital administrators, policymakers, and patients would normally care about. For Bruch, the more immediate hope is that the finding changes some individual calculations. His students, the ones considering consulting careers, kept asking whether the work could actually move the needle on healthcare’s deep inefficiencies. “Answering those questions has been difficult because the evidence has been so limited,” he said. Now the evidence exists. The answer is a little more specific, and a little less comfortable.
Read more:
scienceblog.com/nonprofit-ho…

1
1
12
1,113
May 14
A Molecular Grappling Hook Could Keep Cancer Drugs Trapped Inside Tumors | Ben Sullivan, ScienceBlog
Getting a cancer drug to a tumor is only half the problem. Within hours of arrival, many therapeutics begin to drift, diluted by blood flow, expelled by pumps embedded in cancer cell membranes, or simply diffusing into surrounding healthy tissue before they’ve had a chance to work. The tumor, in other words, doesn’t hold onto them. And that failure of retention, more than anything else in drug development, might explain why treatments that look promising in the lab so often disappoint in the clinic. A team at the University of California, San Francisco has spent years trying to fix this, and their latest results suggest a rather elegant solution: a molecular grappling hook that physically embeds itself in the cancer cell membrane and refuses to let go.
The system, described in a paper published this week in ACS Central Science, works by exploiting one of the tumor’s own biochemical quirks to anchor drugs in place rather than releasing them to wander.
At the heart of the approach is a class of engineered peptides the researchers call restricted interaction peptides, or RIPs. Each one is roughly 30 amino acids long and built in three sections, almost like a Swiss Army knife snapped shut. The first section, derived from an antimicrobial peptide called Temporin L, is the business end: it can fold into a corkscrew-like structure and dig into cell membranes. The second section is a masking domain that keeps the first section folded and inert, prevented by its electrical charge from touching anything. Between them sits the key: a short sequence specifically designed to be cut by a protease enzyme that the tumor produces in abundance. Leave the peptide whole, and the masking domain does its job, keeping the whole assembly inactive. Clip it in the right place, and the membrane-grabbing end springs free.
The protease in question is fibroblast activation protein, or FAP. It’s a serine protease expressed at high levels by cancer-associated fibroblasts, the supportive cells woven through the stroma of solid tumors, present in nearly every cancer type. FAP has long attracted interest as a therapeutic target, partly because it’s so consistently expressed across tumor types and largely absent from normal adult tissue. Early attempts to block it pharmacologically ran into trouble (protease redundancy means blocking one enzyme rarely achieves much), but the new strategy does the opposite: instead of stopping FAP, it uses FAP as a trigger.
Designed to Stick
To build the FAP-activated version, which they call FRIP, the team first needed to know exactly what sequences of amino acids FAP prefers to cut. They screened 228 peptides simultaneously using a technique called multiplex substrate profiling by mass spectrometry, essentially running hundreds of cleavage reactions in parallel and tracking the results by mass. The winner was a sequence reading HIGP-TAAY, which FAP cleaved at a rate roughly comparable to, and in some respects faster than, collagen, FAP’s natural substrate in tissue.
What happened next, when FRIP met a live cancer cell, was visible in real time under a confocal microscope. Fluorescently tagged FRIP added to U-251 glioblastoma cells (a line chosen for its high FAP expression) produced a sharp ring of fluorescence along the cell membrane within about 10 minutes. By 20 minutes, the signal had moved inward: the peptide, and whatever it was carrying, had been swallowed whole. Block FAP with an inhibitor first, and the ring never forms. Use a cell line with low FAP expression, and the effect is sluggish. The mechanism is about as clean as these things get.
For the drug delivery test, the team attached MMAE (monomethyl auristatin E), a potent cell-killing agent widely used in antibody-drug conjugates. The combination proved toxic to glioblastoma cells at concentrations roughly 30 times lower than needed for the undelivered drug, suggesting the membrane-tethering step was shuttling far more payload into cells than passive diffusion alone could manage. Michael Evans, one of the study’s corresponding authors, has argued that retaining drugs within tumors is perhaps the most overlooked dimension of cancer pharmacology. The data rather support him.
Outsmarting the Clinic’s Standard Bearer
In mice bearing head and neck cancer tumors, FRIP loaded with MMAE shrank tumors more effectively than the drug alone, and without the body-weight loss that forced the free-drug group to be withdrawn from the study at day 8. That last detail matters: MMAE is genuinely toxic at the doses needed to reach therapeutic effect systemically. Tethering it to a tumor-specific delivery vehicle appears to substantially reduce the collateral damage, letting the drug concentrate where it’s needed without the rest of the body bearing the consequences.
The team then swapped the chemotherapy payload for radioactive copper, first for imaging (copper-64, a positron emitter) and then for therapy (copper-67, a beta emitter). Here the comparison gets particularly pointed. The researchers pitted their FRIP against FAPI-46, an active site-directed FAP radioligand currently in clinical trials and something of a gold standard in the field. Both compounds cleared from blood at nearly the same rate. But 24 hours after injection, FRIP had accumulated in tumors at roughly five times the concentration of FAPI-46. The underlying reason is almost counterintuitively simple: FAPI-46 binds to FAP in a one-for-one stoichiometric fashion, while FRIP exploits the catalytic nature of the enzyme. A single FAP molecule can clip many FRIP peptides in sequence, each one anchoring to the nearest membrane, building up like barnacles. The competition, by contrast, can only get as far as there are active sites to occupy.
One dose of therapeutic copper-67 loaded onto FRIP delayed glioblastoma growth significantly compared to vehicle and outperformed an equivalent dose of the clinical-stage radioligand. The authors are careful, as they should be, to note that the different chelation chemistry and pharmacokinetics make a completely rigorous comparison difficult. But the signal is hard to ignore.
Evans says the technology should maximize drug delivery to tumor tissue while sparing normal tissues, and that the same molecule used to image a tumor could eventually treat it. First-in-human imaging studies are expected to begin later this year, with a UCSF spinout called Therapaint developing the platform commercially. The version already in clinical trials, GRIP B, targets a different enzyme (granzyme B, released by immune cells in the tumor microenvironment) and is being used to monitor responses to immunotherapy. FRIP is the oncology-targeted version of what is, in principle, an endlessly adaptable system: swap the cleavage sequence, swap the payload, and theoretically you have a new targeting agent for any disease where a protease runs hot.
Whether that modularity holds up in human bodies, where enzymes roam farther from their tumors and individual variation in FAP expression may complicate the picture, remains to be seen. But the logic of the approach, letting the disease itself arm the weapon, is one of those ideas that seems obvious in retrospect. It took quite a lot of biochemistry to make it work.
Read more:
scienceblog.com/a-molecular-…
8
1,356