
💊 ⌛ Edinburgh based multi-disciplinary team of #AntibioticGuardians #KeepAntibioticsWorking #AntimicrobialResistance #AntimicrobialStewardship #AMR
Joined July 2019
- Tweets 1,614
- Following 245
- Followers 573
- Likes 2,331
70 Photos and videos





Pinned Tweet

17 Nov 2020
Tomorrow is #EuropeanAntibioticAwarenessDay we have updated our intranet page with lots of resources #dontbeadipstick #WAAW2020 thanks to @elizbeech for the inspiration "to dip or not to dip"

8
37
NHS Lothian Antimicrobial Stewardship retweeted

29 Jun 2023
Like Edinburgh and the Lothians? Come be my boss!
An exciting time in infection medicine - joint ID and micro job
apply.jobs.scot.nhs.uk/Job/J…
6
11
3,627
NHS Lothian Antimicrobial Stewardship retweeted
23 Jun 2023
2023 RCPATH ACHIEVEMENT AWARD WINNERS 🏆
Huge effort by NHS Lothian infection team to deliver the "Infection bootcamp" over past 2 years. Well deserved recognition of the team's hard work 🎉

23 Jun 2023

Well done Team Micro/Virol NHSLothian for our fantastic Infection Training Bootcamp!
6
25
3,020
NHS Lothian Antimicrobial Stewardship retweeted

21 Jun 2023
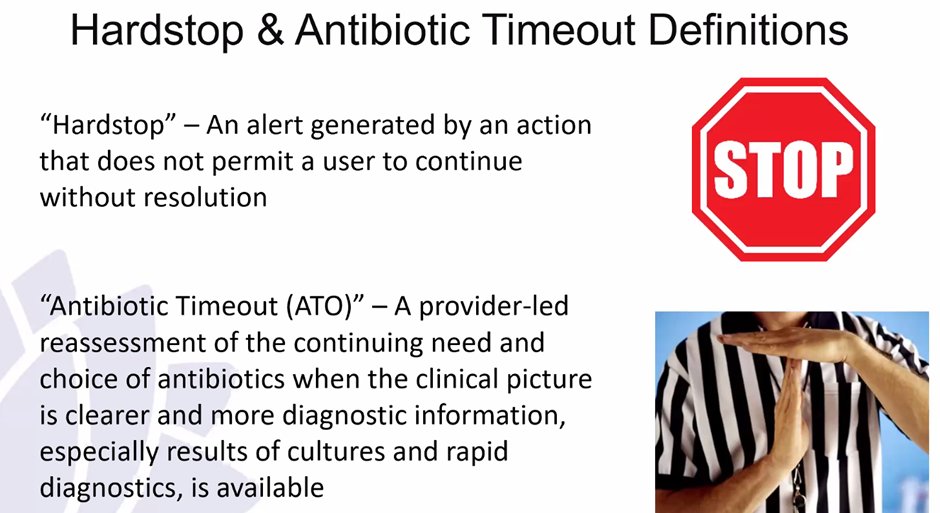
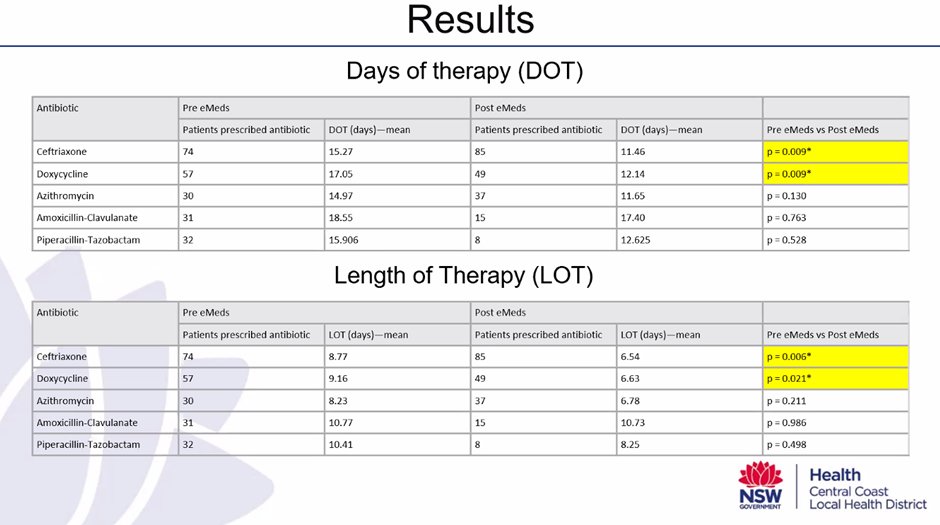
@NCAS_Aus Journal Club. Thanks @simgalimam for discussing his local health networks implementation of antibiotic hard stops, the benefits of reducing #DOTs and #LOTs and potential consequences when not reviewed. Read full publication here: bmcinfectdis.biomedcentral.c…
1
6
4,327
NHS Lothian Antimicrobial Stewardship retweeted

9 Jun 2023
The official opening of the new and improved Junior Doctors mess at WGH today in Pentland Lodge. Thank you to all who made it happen especially our Chief Registrars and @NHSLothianMedEd team

2
5
62
6,831
NHS Lothian Antimicrobial Stewardship retweeted

6 Jun 2023
I also have a related editorial with @ValerieVaughnMD that a lot of the environment we "swim" in hasn't been thoughtfully designed at all.
#HVMC2023
qualitysafety.bmj.com/conten…
3
14
1,082

“ACCEPT-UTI: Empirical use of piperacillin/tazobactam for ESBL UTIs showed no difference in clinical success outcomes compared to the empirical use of carbapenems”
Check out this study by @sylviastefanos et al:
doi.org/10.1093/jacamr/dlad0…
@AthenaLVHobbs @SIDPharm #JACAMRNews
23
81
10,110
NHS Lothian Antimicrobial Stewardship retweeted

18 May 2023
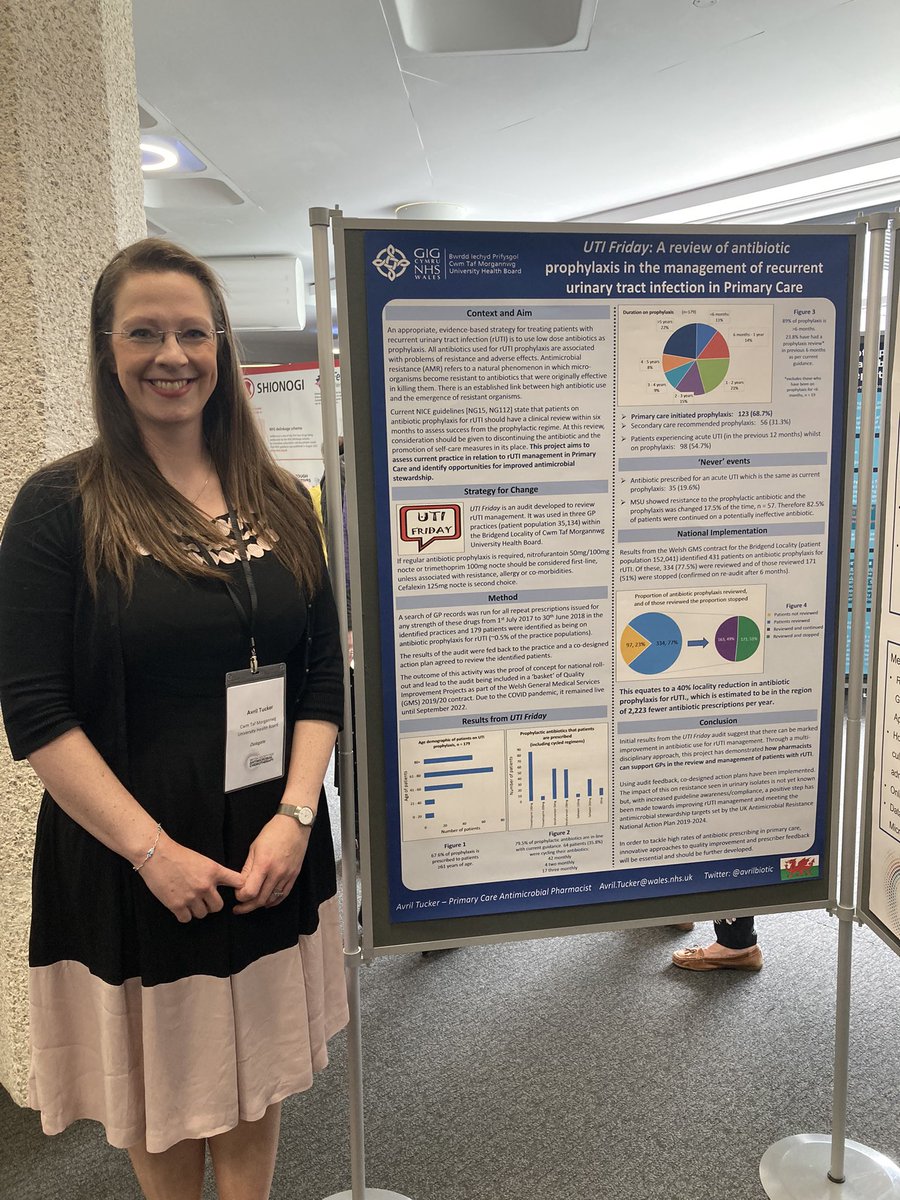
Found my poster! 📸
Outcome: 40% REDUCTION in antibiotic prophylaxis for recurrent UTI within Bridgend locality! That’s >2,200 fewer antibiotics per year.
#UTIFriday #BSACSpring2023
12
20
146
13,758
NHS Lothian Antimicrobial Stewardship retweeted

16 May 2023
Fluoroquinolone antibiotics: reminder of measures to reduce the risk of long-lasting, disabling and potentially irreversible side effects | European Medicines Agency europa.eu/!WGkDrR via @EMA_News
5
16
4,575
NHS Lothian Antimicrobial Stewardship retweeted

16 May 2023
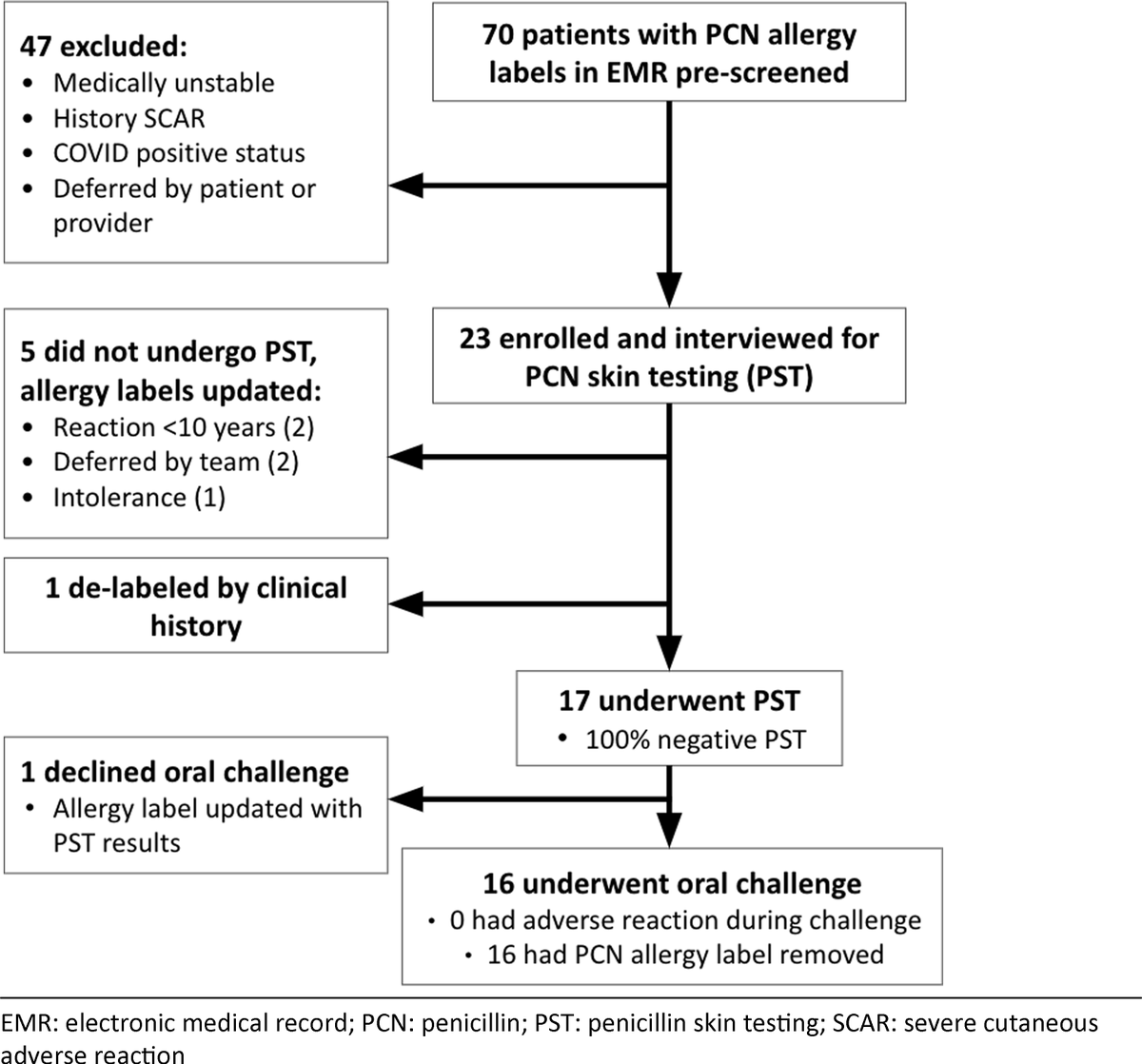
From @dr_vpatel910; @BrianChuSF; @UPenn_Allergy: A penicillin allergy testing service assessed penicillin allergy in patients with hematologic malignancies. All tested patients were negative. Patients who were challenged passed and were delabeled.
📄cup.org/42DWxvj
7
16
2,944
NHS Lothian Antimicrobial Stewardship retweeted

16 May 2023
Transfer of antibiotics and their metabolites in human milk: Implications for infant health and microbiota: doi.org/10.1002/phar.2732
5
12
1,984
NHS Lothian Antimicrobial Stewardship retweeted

15 May 2023
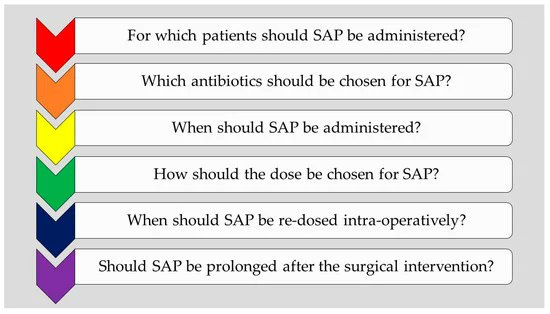
🆕️⚡️ @antibioticsmdpi @MassimoSartelli
Six Long-Standing Questions about Antibiotic Prophylaxis in Surgery #IDTwitter
mdpi.com/2079-6382/12/5/908
1
20
55
10,323
NHS Lothian Antimicrobial Stewardship retweeted

15 May 2023
Are you an early-stage clinician interested in haematological #infections? The #ICDhaem course in our Infection Clinical Dilemmas series explores the common infection issues in haemato-oncology patients and the best ways to manage them 🦠 Join now! 👇 infectionclinicaldilemmas.co…
4
11
1,612
NHS Lothian Antimicrobial Stewardship retweeted
15 May 2023
Assessing clinical cure of empirical piperacillin/tazobactam for ESBL urinary tract infections (ACCEPT—UTI) academic.oup.com/jacamr/arti…
5
7
1,739
NHS Lothian Antimicrobial Stewardship retweeted

11 May 2023
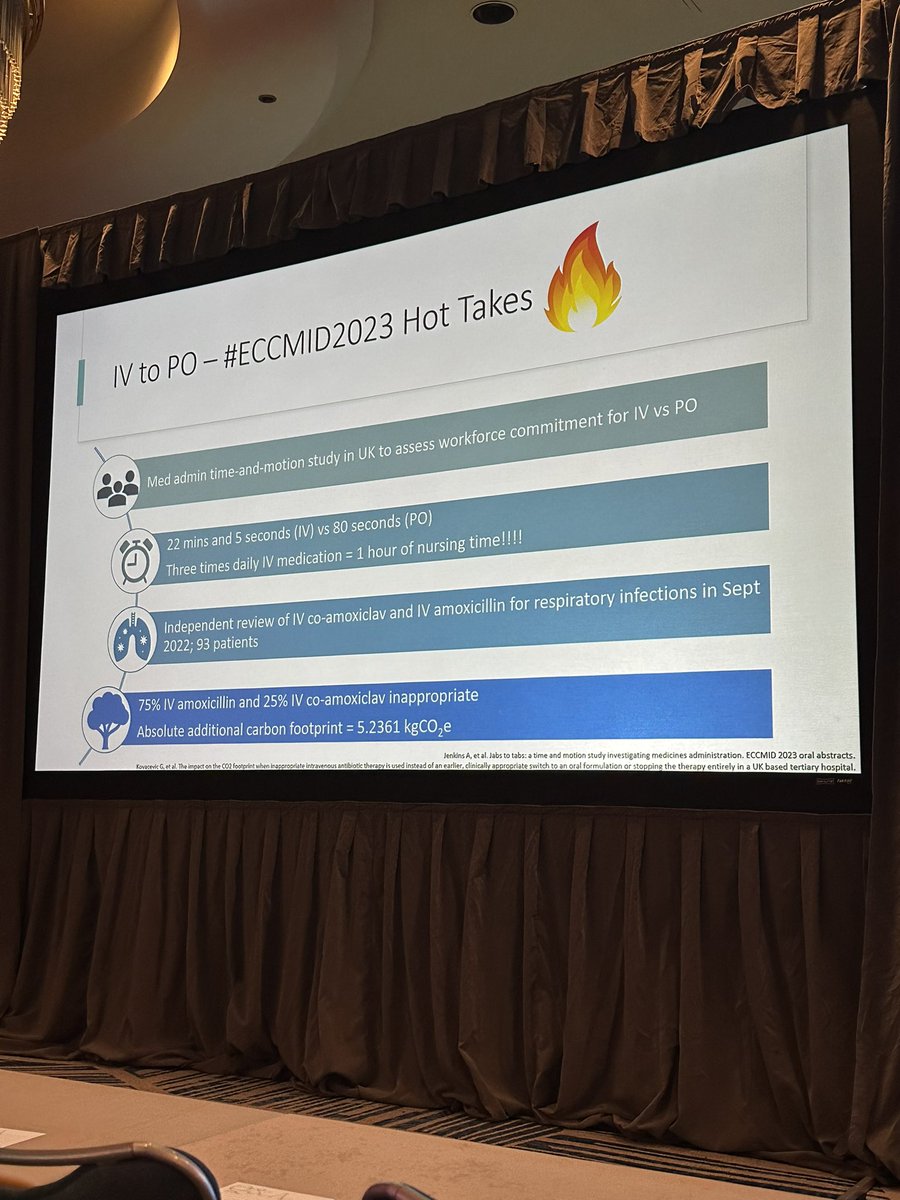
@ErinMcCreary giving us a unique argument for advocating IV to PO abx switch for serious infections ➡️ Saving massive amounts of nursing time! ⏰ (avg 22 min to administer IV vs. 80 seconds for PO) 🤯
@MAD_ID_ASP #MADID2023

2
9
51
4,654
NHS Lothian Antimicrobial Stewardship retweeted
11 May 2023
"IV antibiotics hold some kind of “mythical status” for both the clinician and patient, especially when it comes to deeper infections like bacteremia and infective endocarditis.Mythology is, unfortunately, a poor proxy for data, but luckily evidence-based alternatives exist!"🎯
11 May 2023

Wow., it's published! @BradSpellberg et al @CMIJournal
🔥Choosing Patients Over Placebos: Oral Transitional Therapy vs. IV-Only Therapy for Bacteremia and Infective Endocarditis🔥 #IDTwitter
clinicalmicrobiologyandinfec…
4
20
10,761
NHS Lothian Antimicrobial Stewardship retweeted
11 May 2023
"Choosing the less safe, not more effective IV-only alternative may be akin to administering a proverbial “placebo” to treat the clinician’s or patient’s own anxiety"
Please RT
11 May 2023
Wow., it's published! @BradSpellberg et al @CMIJournal
🔥Choosing Patients Over Placebos: Oral Transitional Therapy vs. IV-Only Therapy for Bacteremia and Infective Endocarditis🔥 #IDTwitter
clinicalmicrobiologyandinfec…
5
10
4,818
NHS Lothian Antimicrobial Stewardship retweeted
9 May 2023
Defining the Optimal Duration of Therapy for Hospitalized Patients With Complicated Urinary Tract Infections and Associated Bacteremia academic.oup.com/cid/article…
1
9
13
2,535
NHS Lothian Antimicrobial Stewardship retweeted

Real-world evaluation of linezolid-associated serotonin toxicity with and without concurrent serotonergic agents @UKCPAPIN @ESGAP_ABS @biainfection @NCAS_Aus @FIP_org @CW_Pharmacists @ptsafetyNHS sciencedirect.com/science/ar…
8
16
1,640
NHS Lothian Antimicrobial Stewardship retweeted

3 May 2023
Another study that shows the low utility of urine culture in those without urinary symptoms, even for a high risk patient group (HSCT recipients with neutropenic fever)

2
31
83
9,005