
Great food/healthy lifestyle, horror films, paying it forward, and kindness are my main things.
Joined November 2017
- Tweets 3,913
- Following 804
- Followers 930
- Likes 3,455
502 Photos and videos




12 Jul 2024
#dermpath #pathology #dermatology
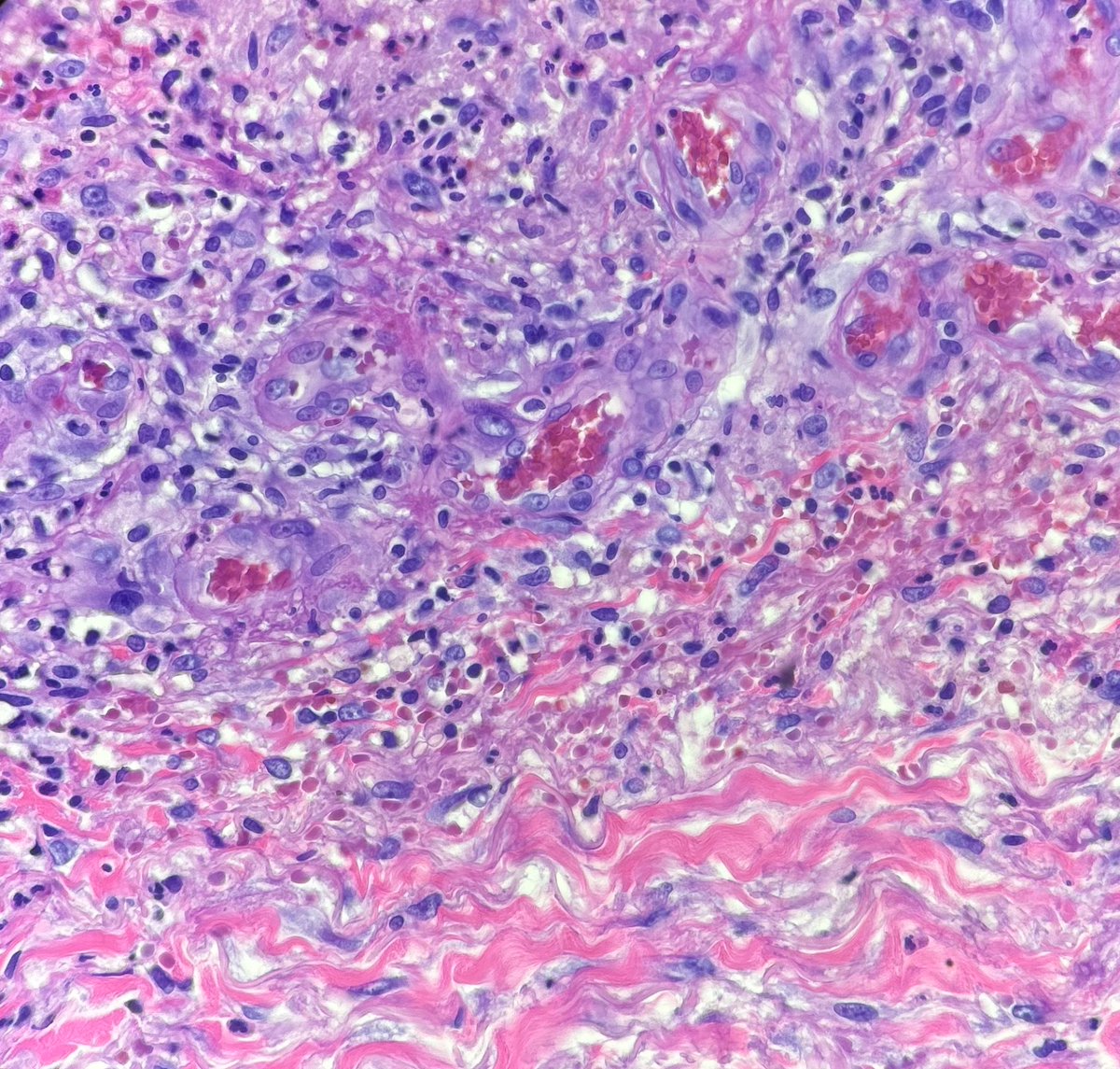
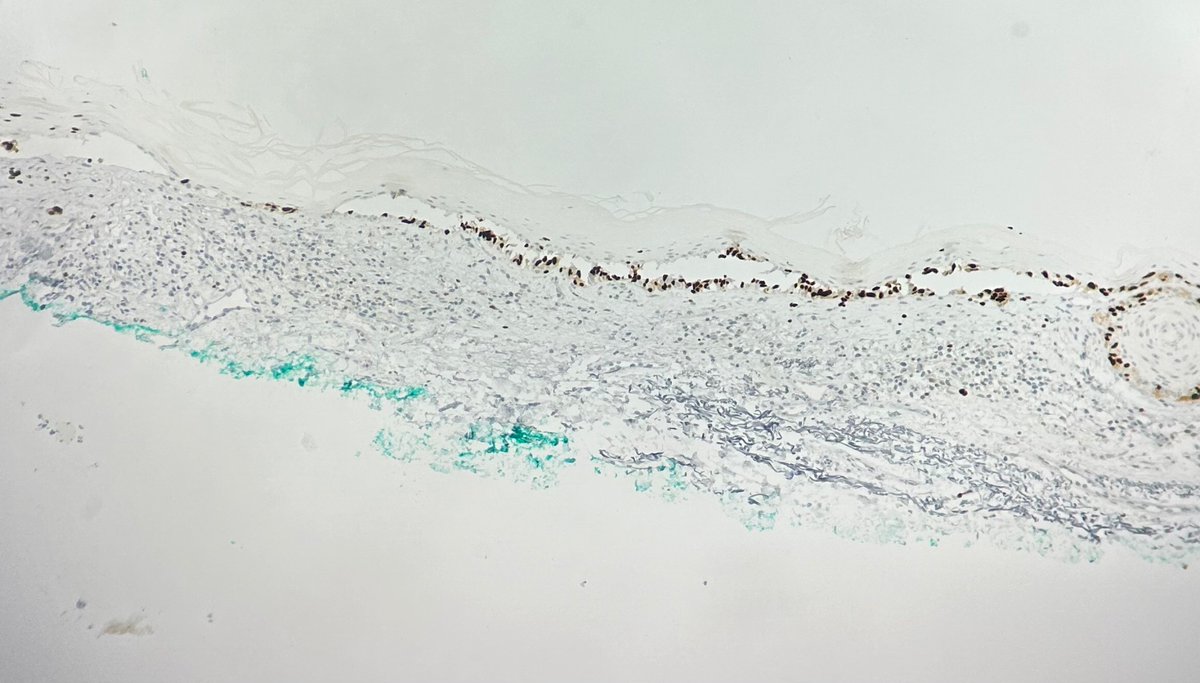
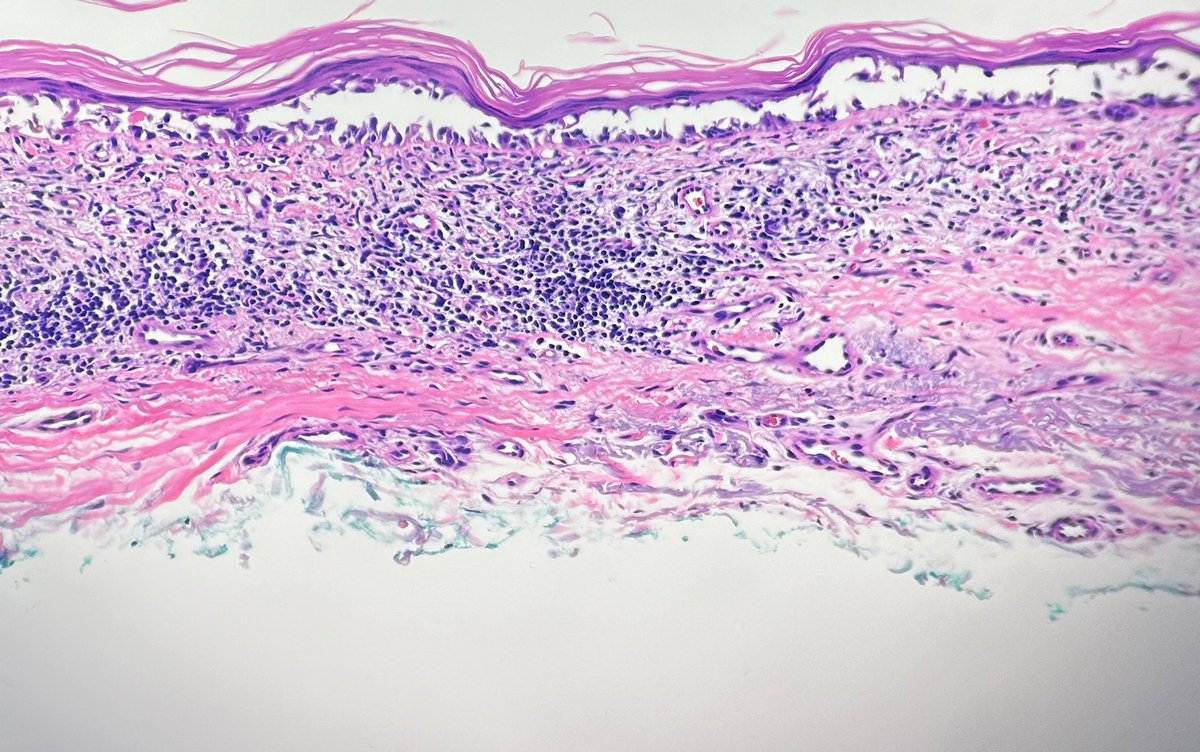
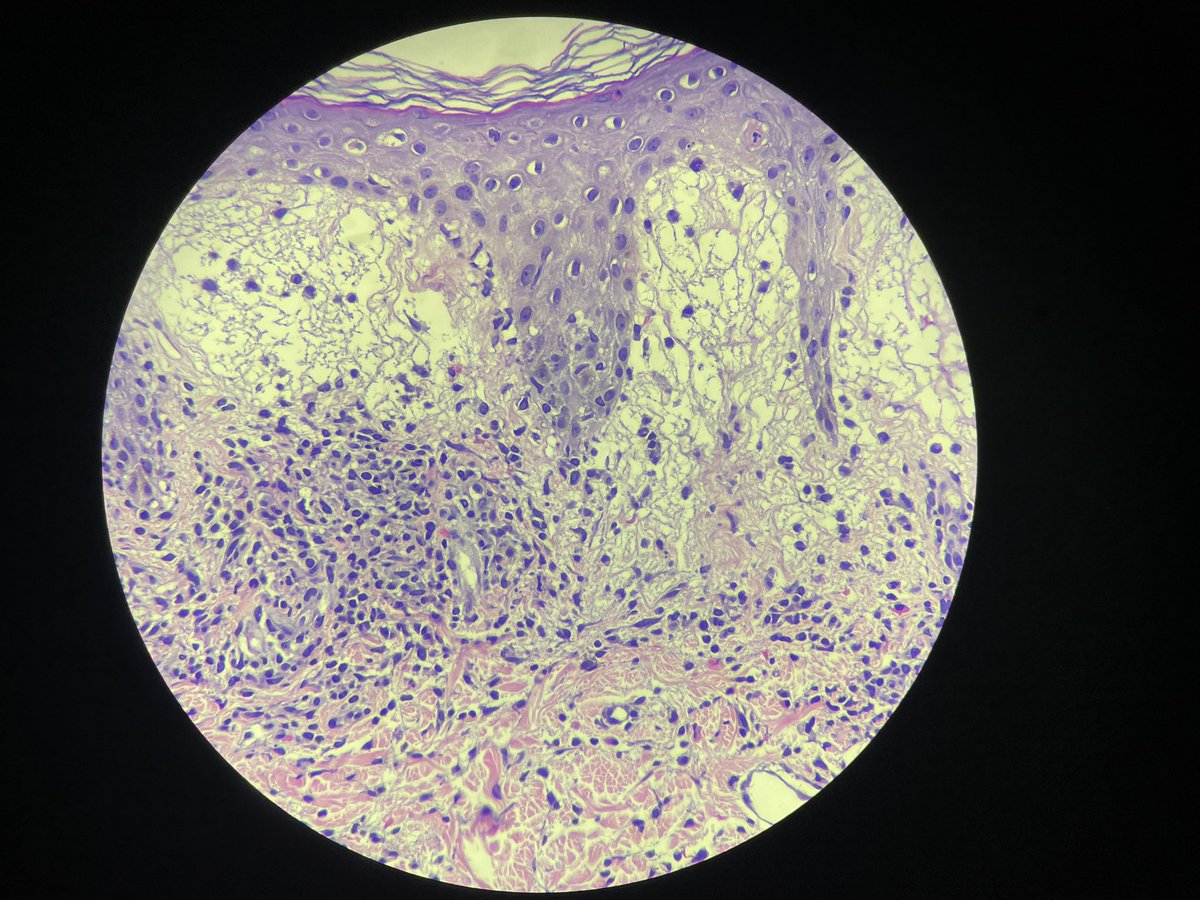
Recent case I had of cutaneous involvement by known granulomatosis with polyangiitis. These were photos I shared with the clinician who was concerned for infection.

3
161
12 Jul 2024
More very good #dermpath learning cases to come. It’s been very busy lately and I fell off the map.
8
264
12 Jul 2024
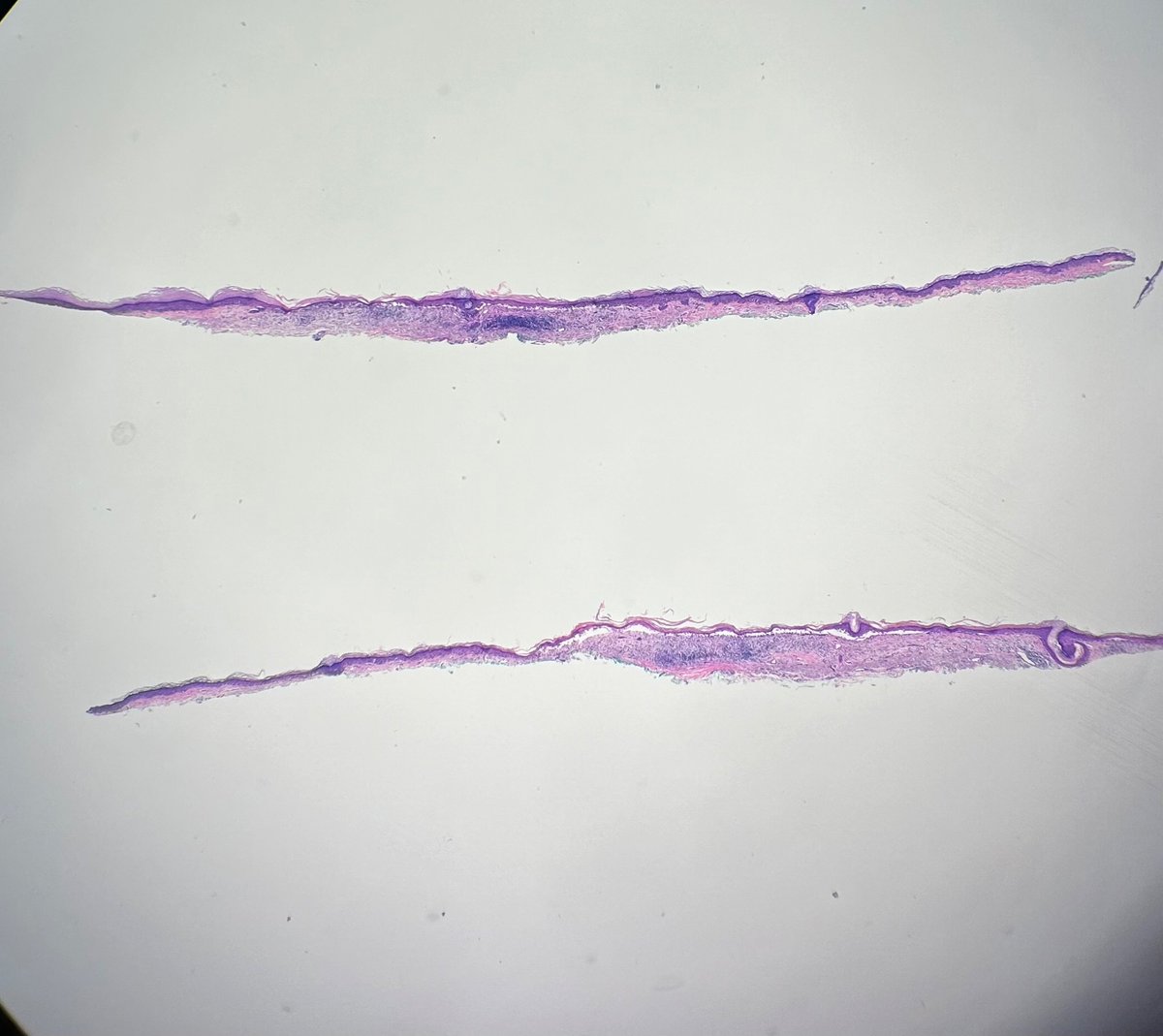
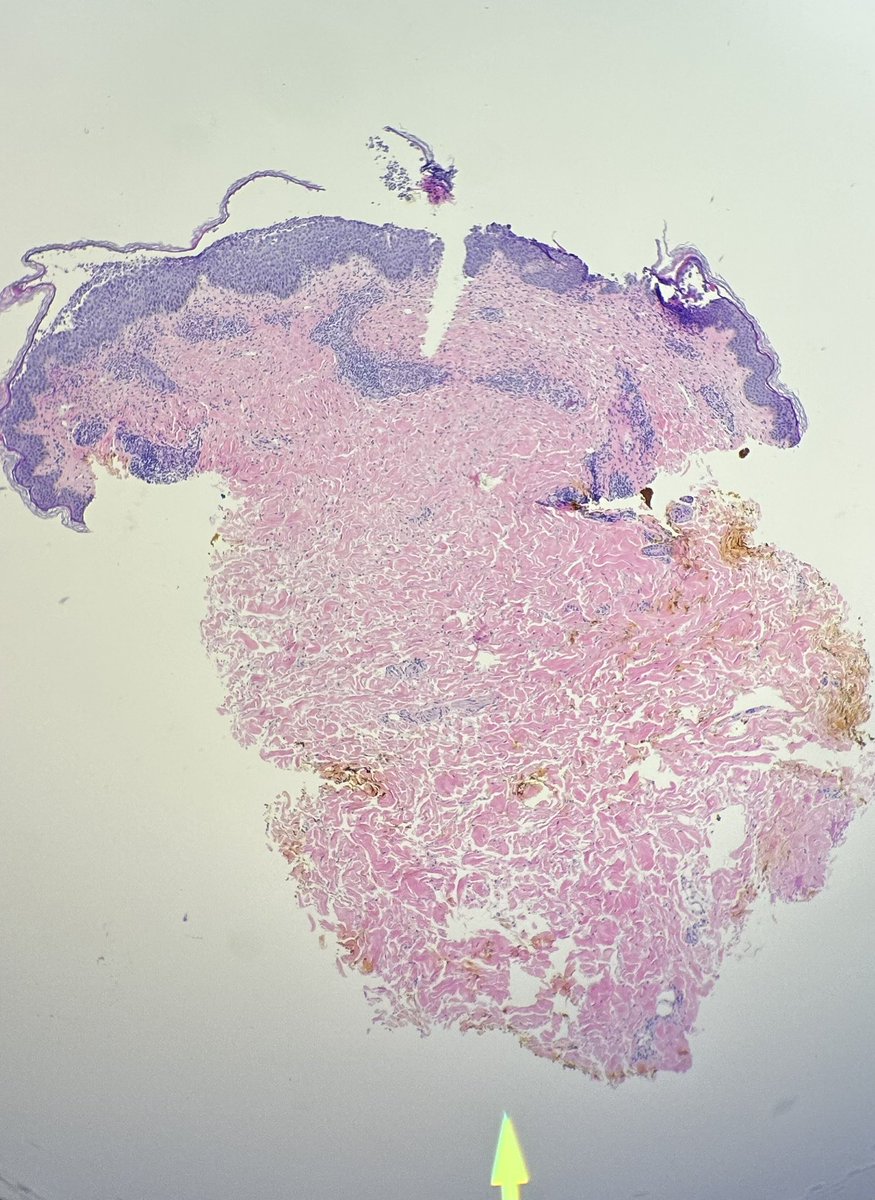
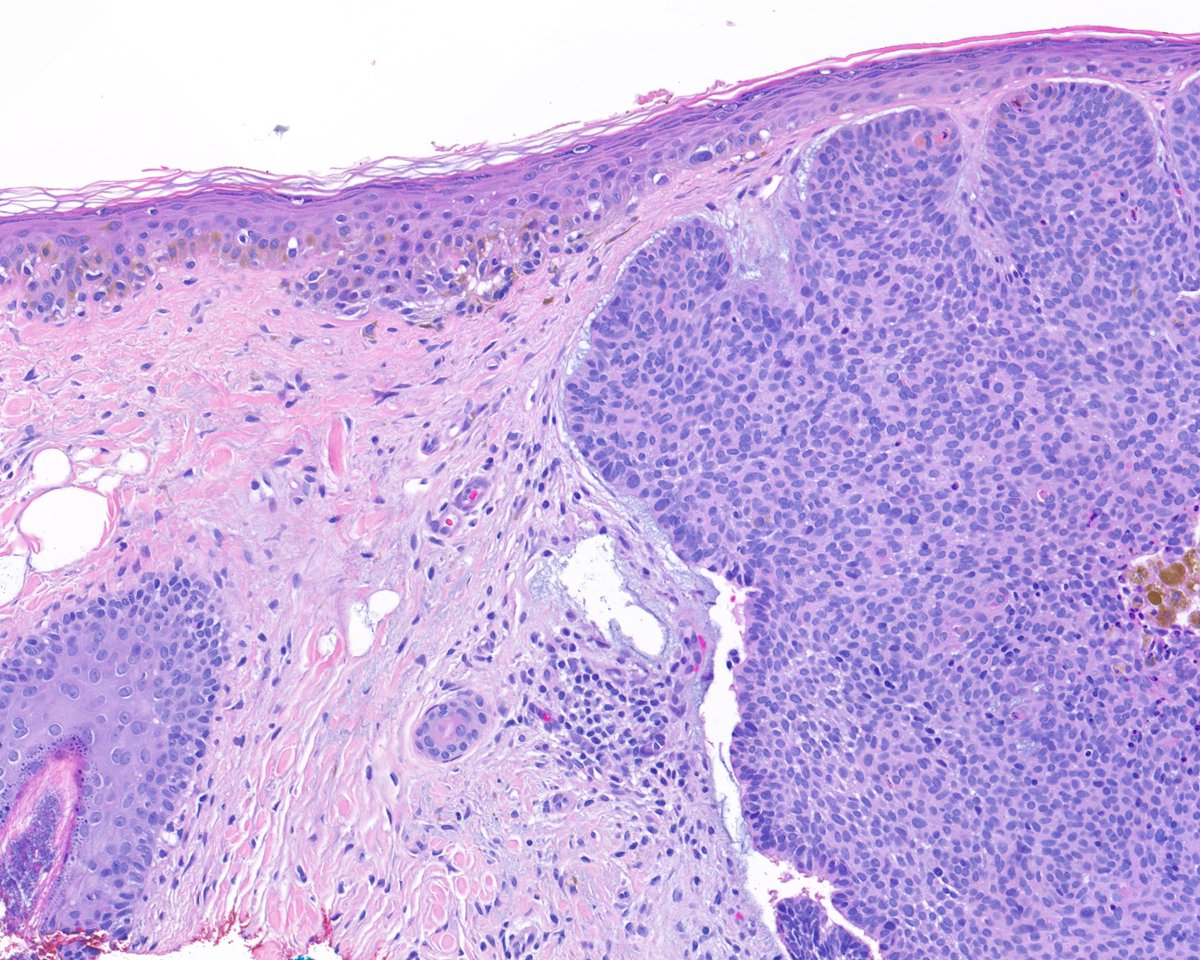
1) Another land mine of a case. TRUST YOUR EYES AND TRAINING. 70 y.o 👩 upper arm. “NUB vs BCC” #dermpath
Looks like a BLK, right? What is a big clue that it’s NOT!
1
1
1
185
12 Jul 2024
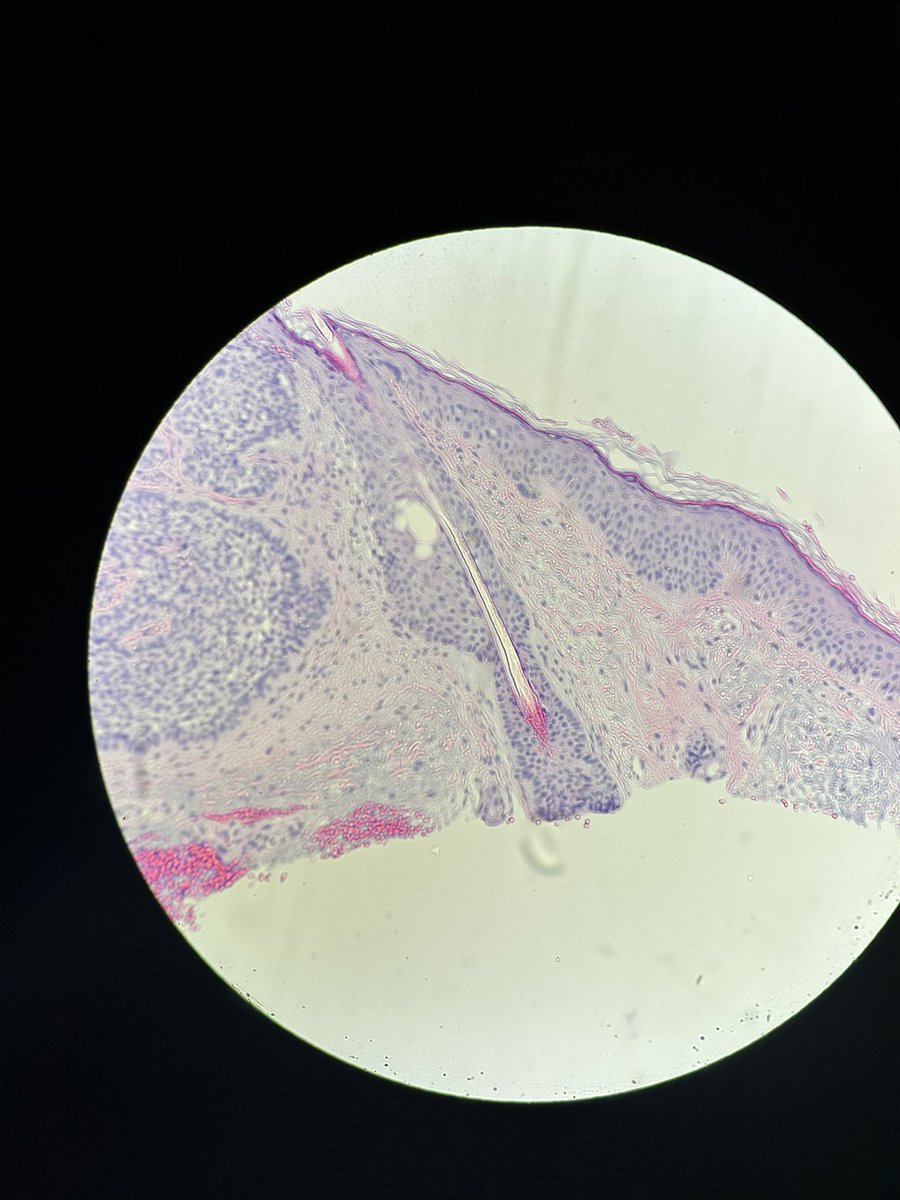
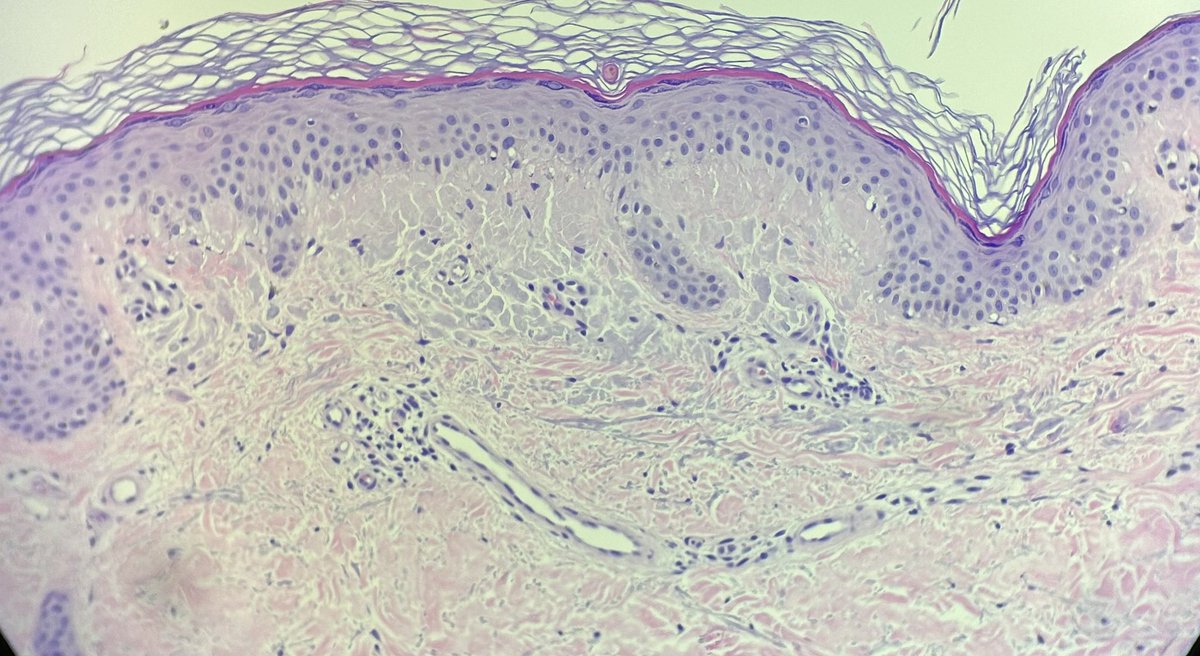
2) Where is the disruption? It’s not at the DEJ like one would see in an interface process. It’s INTRAEPIDERMAL (unzippering). Remember melanocytes lack desmosomes=no adherence
Also, see how jumbled and grey the epidermis is? Another clue.
1
1
94
12 Jul 2024
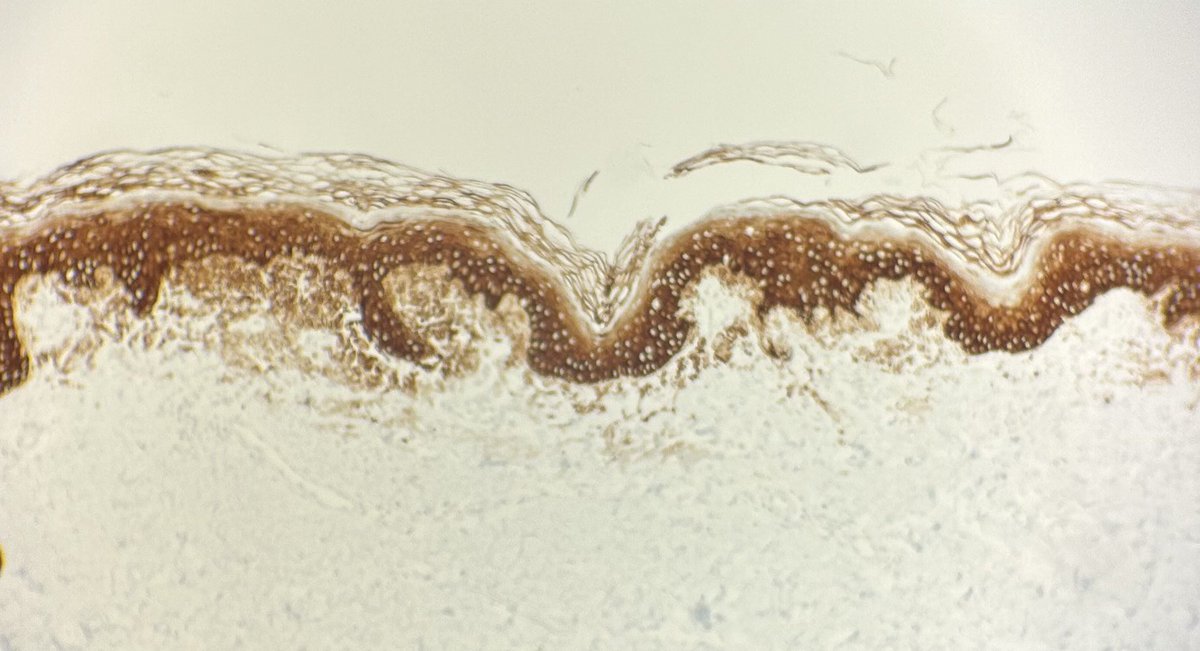
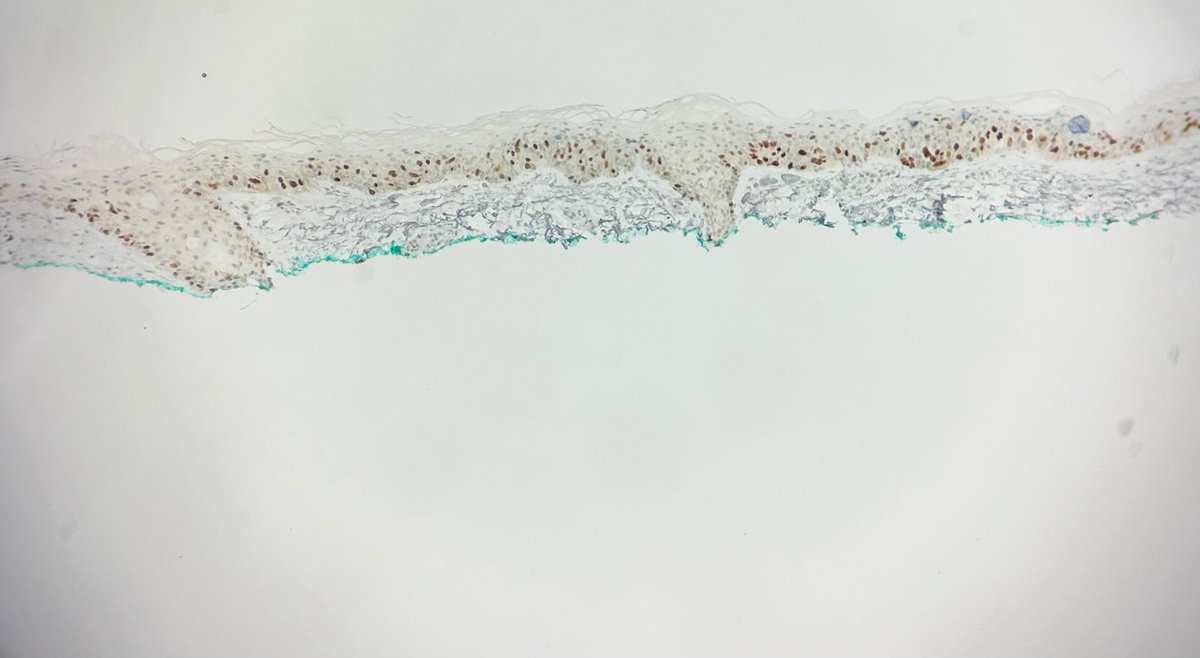
3) IHC to confirm (🧦10 and PRAME). I let out an audible gasp when I got saw them, but was also very relieved that I didn’t go down the tubes with this one (I had great training from @MightyDermPath)! Got the PRAME after the 🧦 for re-excision feasibility purposes.
2
74
Brie Schmidt retweeted

28 Dec 2023

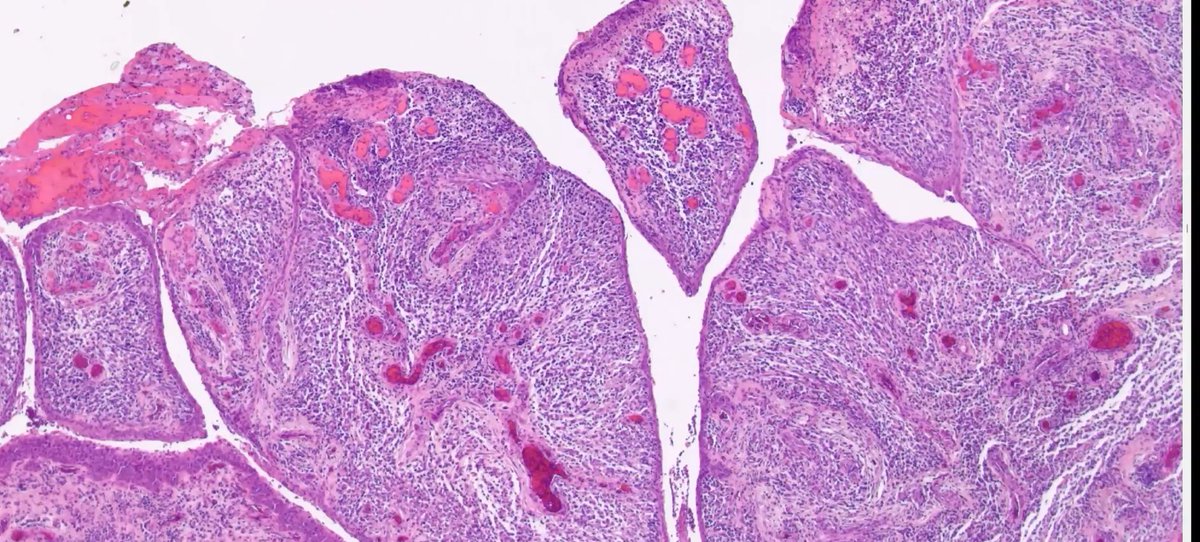
6yo with recent ptosis
Pic B: Squamous papilloma with marked inflammation??
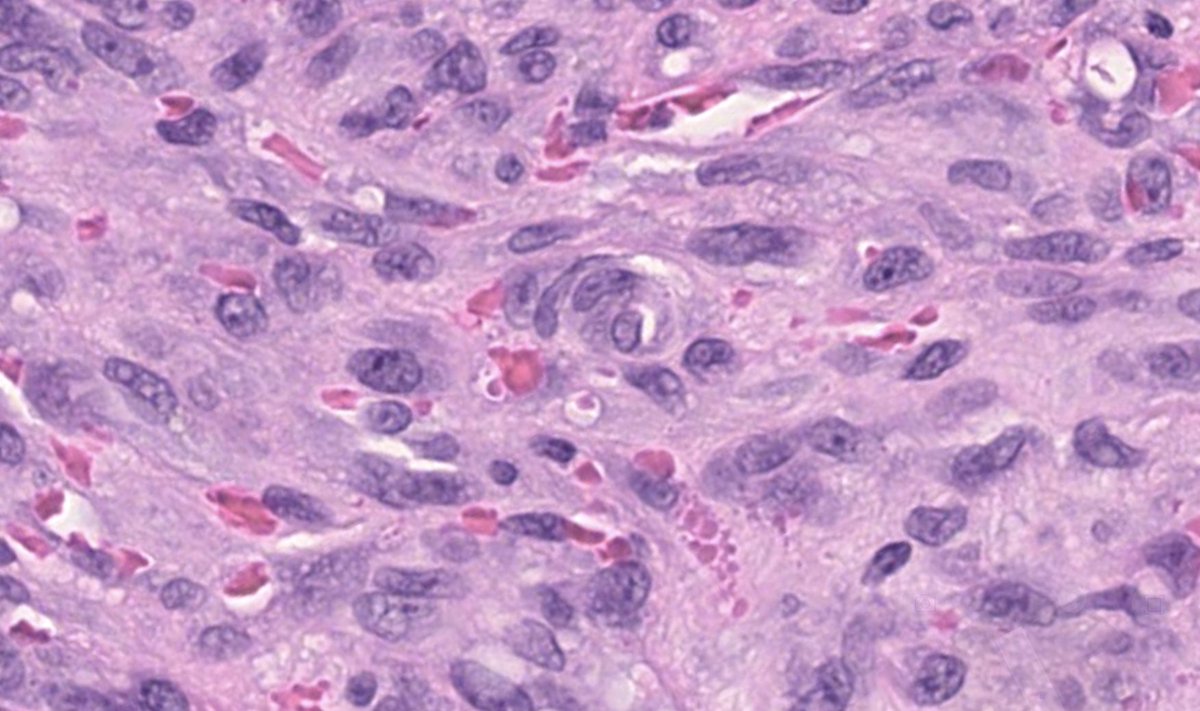
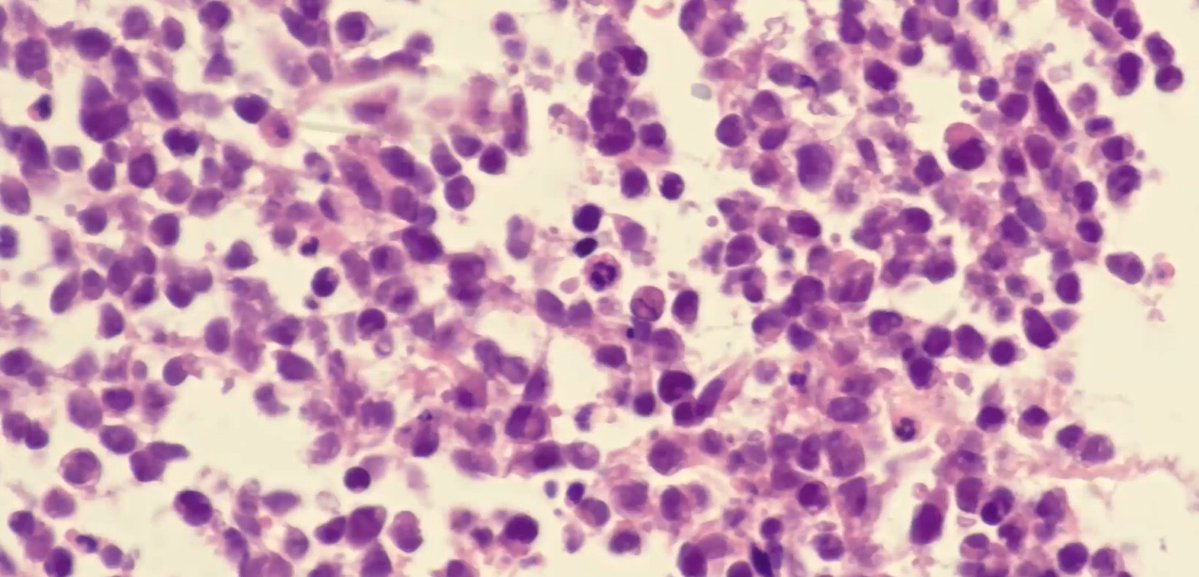
Pic C: High power shows small round atypical cells.
Final diagnosis: Botryoid type embryonal rhabdomyosarcoma
Dr. Stagner and Zembowicz #ophtalmicpath #dermpath #PathX #PathTwitter #pathologists

2
1
3
407
30 Dec 2023
Doctors are pushing Hollywood for more realistic depictions of death and dying on TV - NPR apple.news/Ag2nZx68QSwWttltU…
109
Brie Schmidt retweeted

20 Dec 2023
40yo. Vague GI symptoms and subsequent rash of edematous and erythematous plaques, starting intertriginous, spreading to trunk and extremities. First pruritus, then tender. No response to low dose steroids. Completely cleared after higher dose. Thx @mccalmo for lighting the way.
7
13
33
5,182
Brie Schmidt retweeted

1 Dec 2023
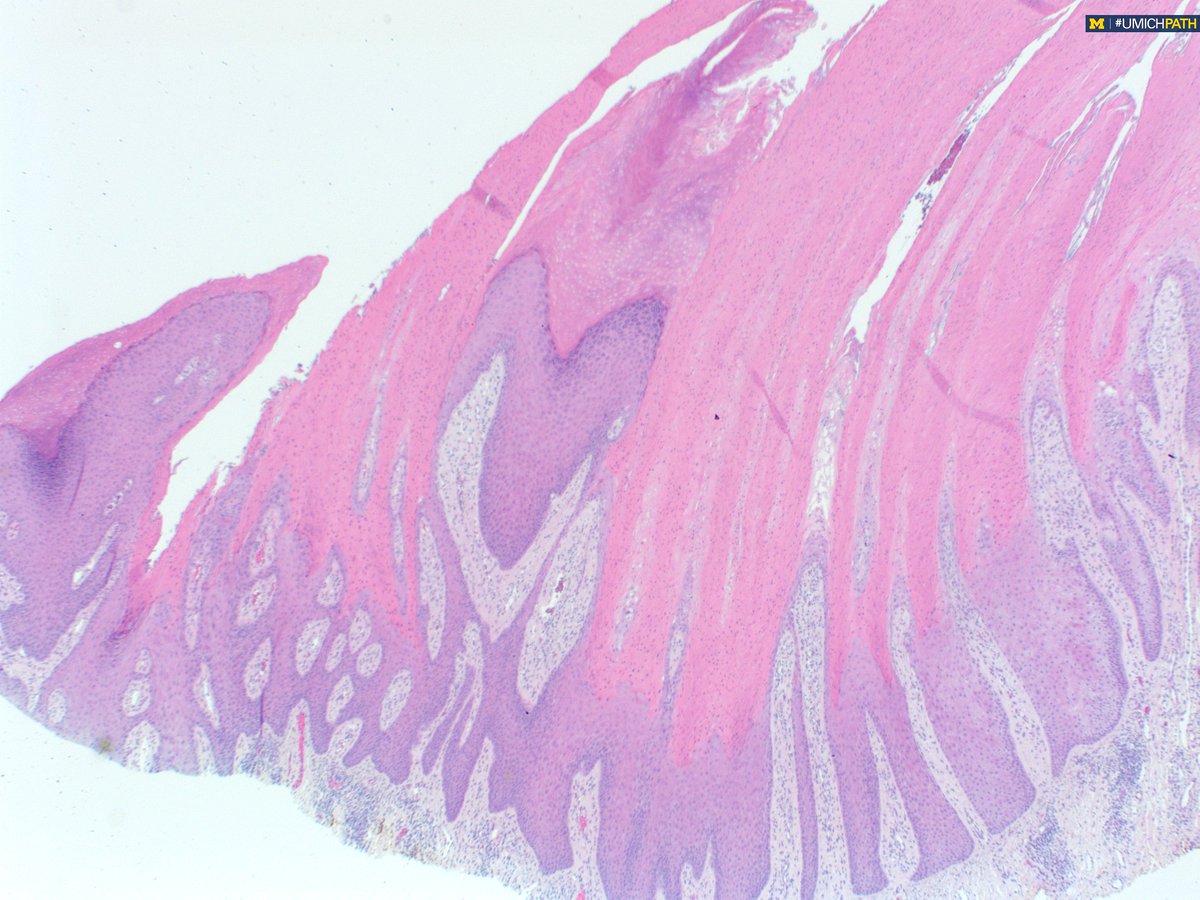
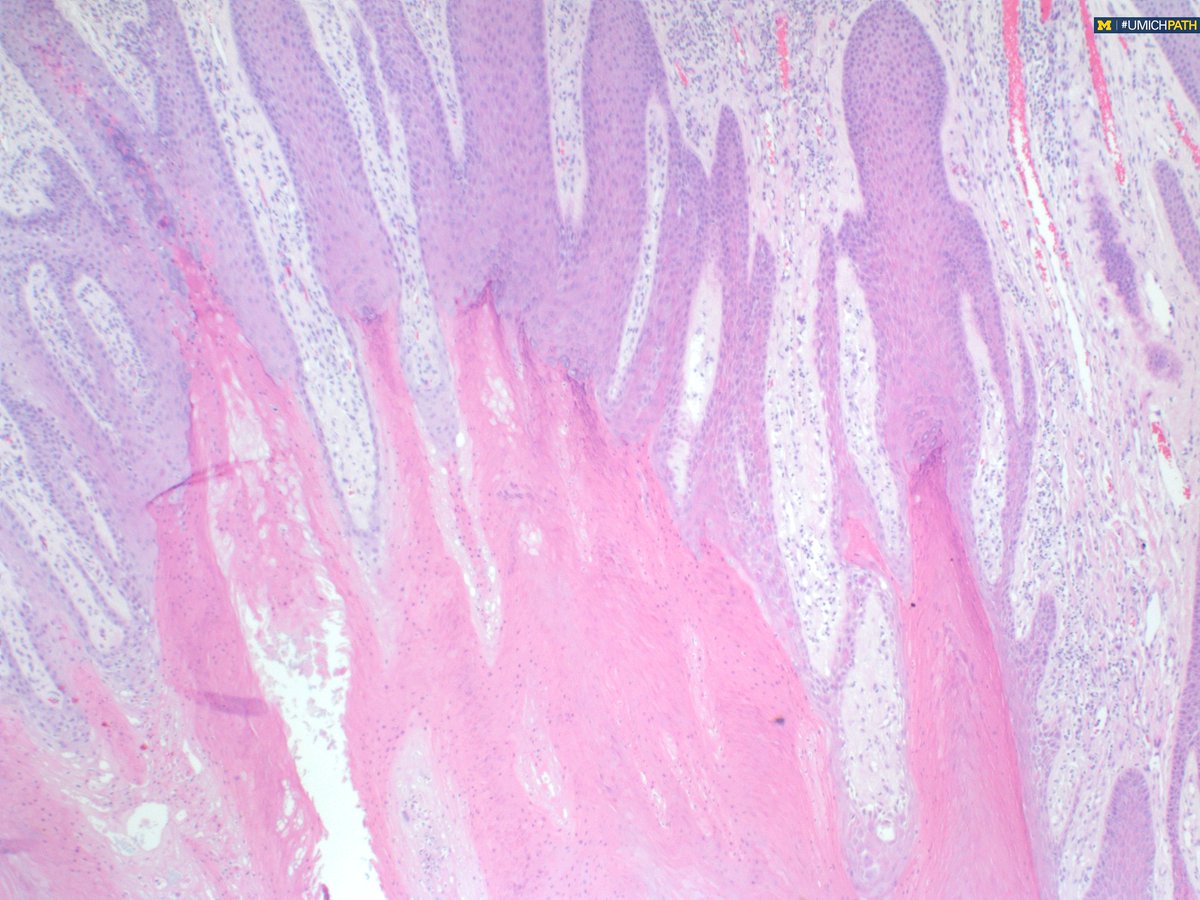
Answer: This is a porokeratoma! At low power you see diffuse wave-like, columnar cornoid lamella with an abrupt transition from normal. Read more about this entity here: onlinelibrary.wiley.com/doi/…
29 Nov 2023

#COTW with PGY1 @meredithkherman featuring a variant in #dermpath. Shave biopsy of groin lesion. What histologic features do you see? What is your differential diagnosis?

7
26
3,802

7 Dec 2023
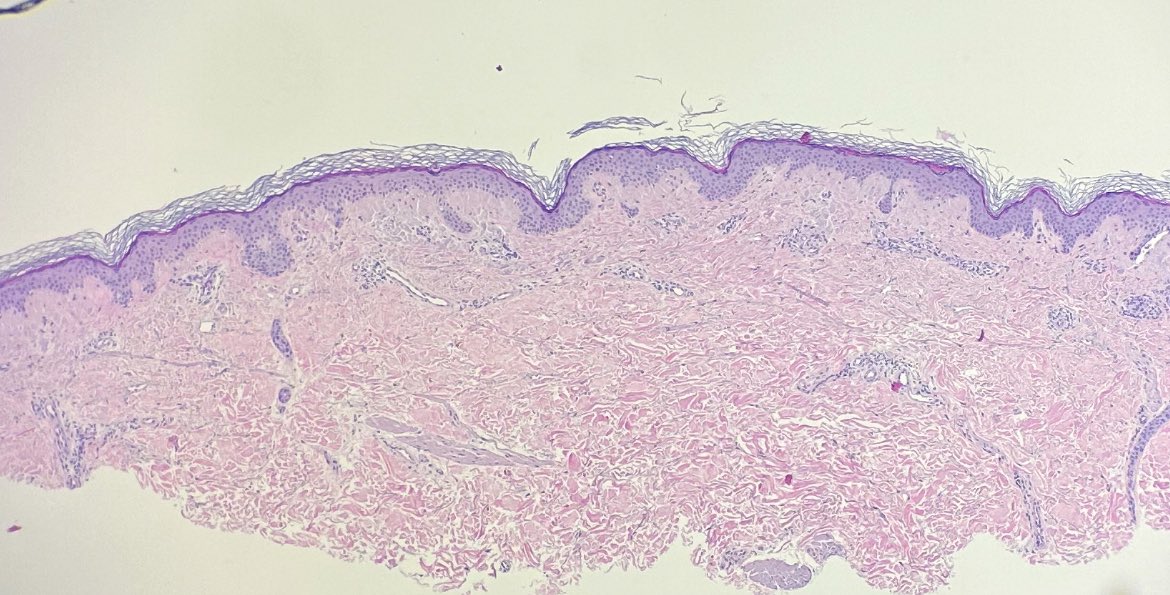
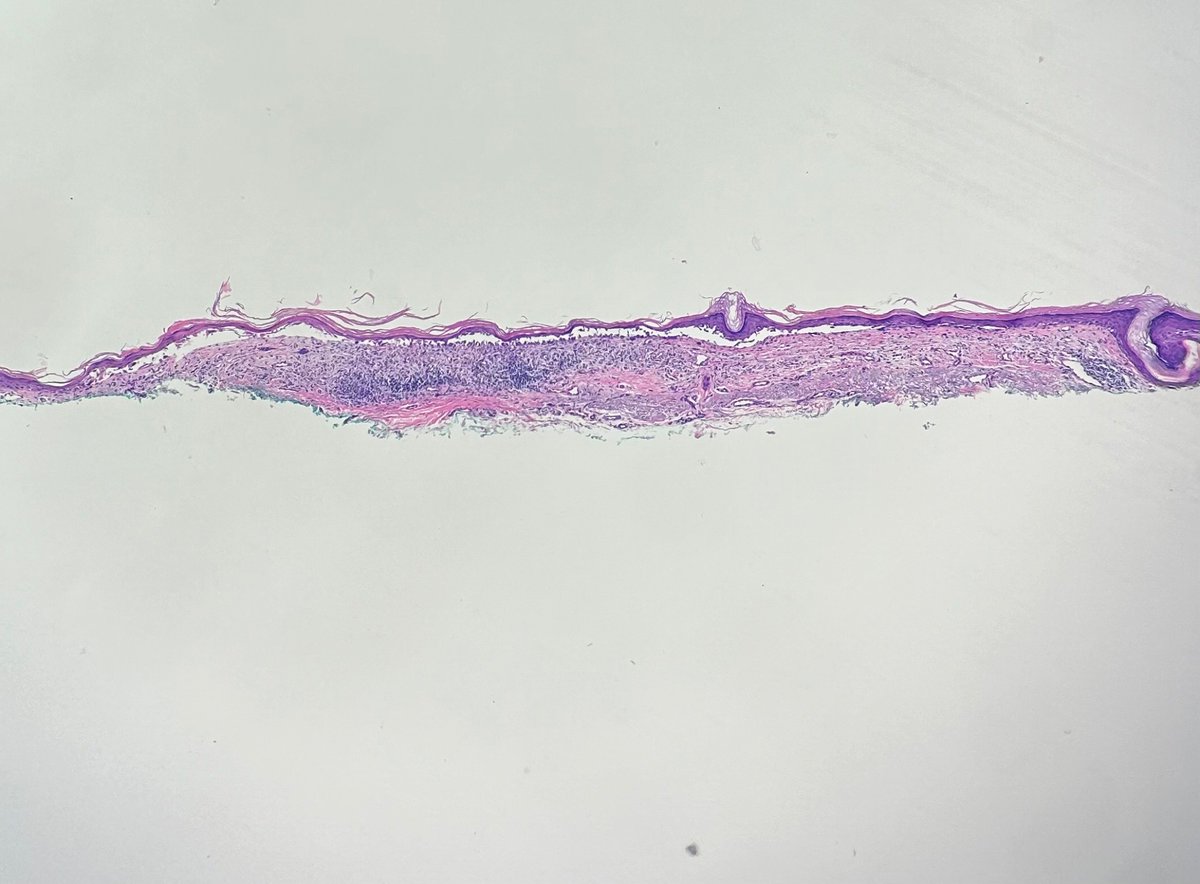
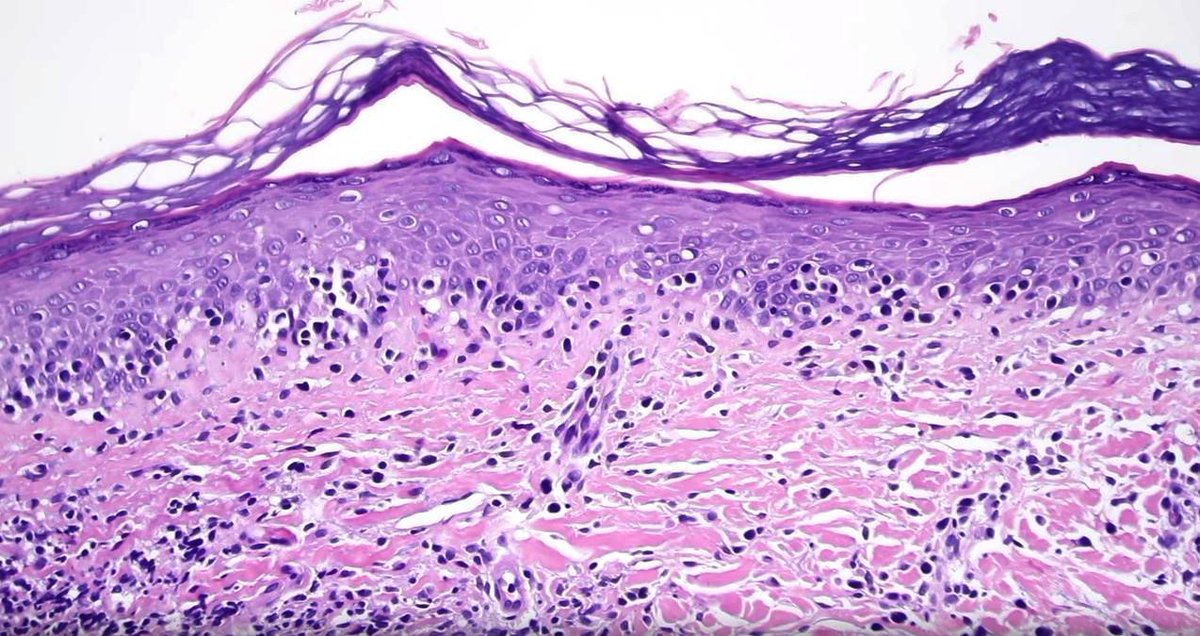
#dermpath for trainees. Middle aged adult, elbow. “Ddx dermatitis vs psoriasis”
What is your low-power impression? Can we exclude psoriasis already?
2
4
30
5,692
7 Dec 2023
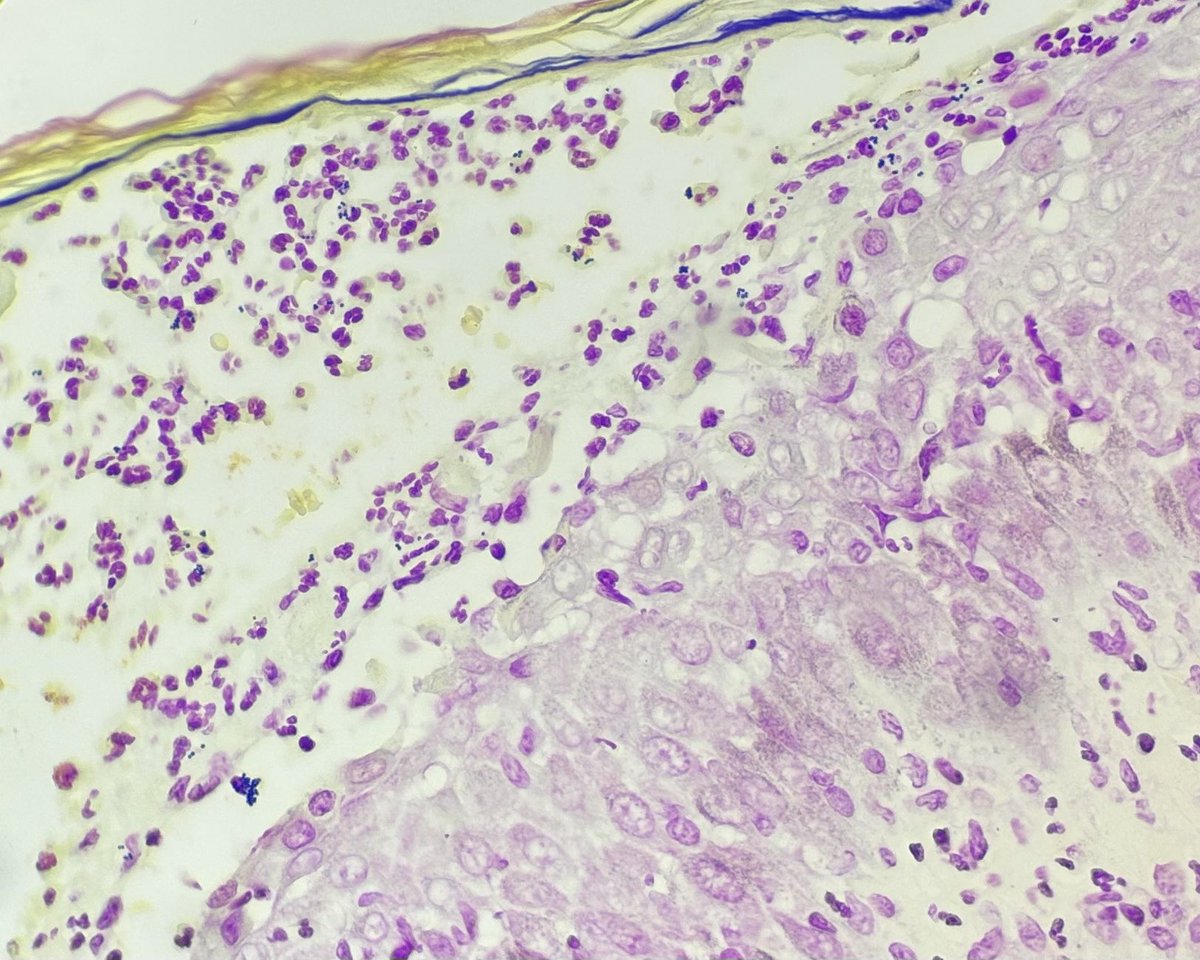
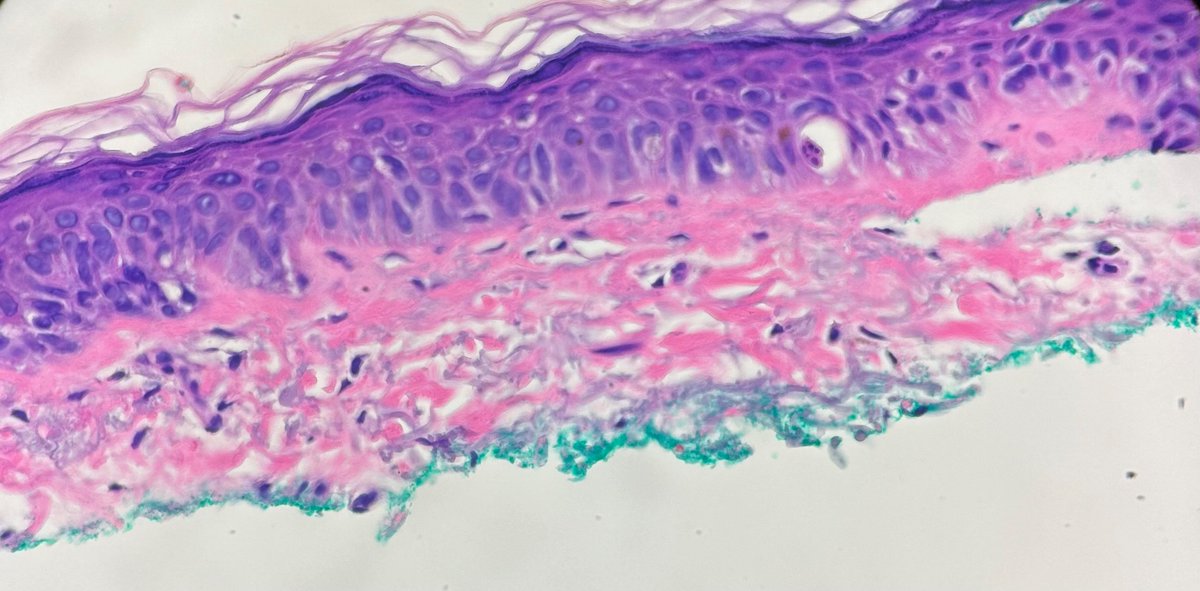
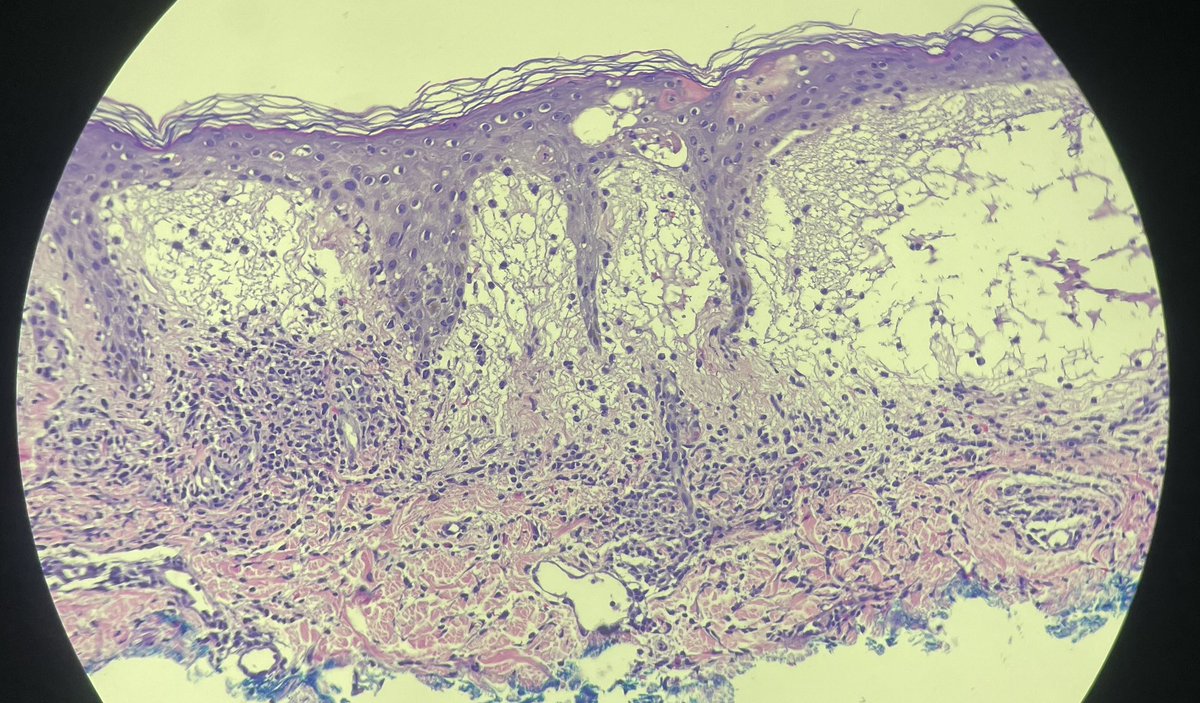
I believe we can. Now, let’s look on high-power. What’s going on? How would you describe the papillary dermis? What’s your ddx and which stain(s) should you get?
3
7
373
7 Dec 2023
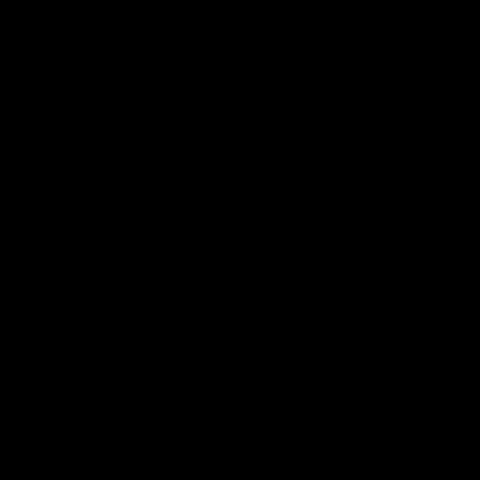
So to recap: this is (macular) localized cutaneous amyloidosis. Presents as (usually) pruritic hyperpigmented macules/patches, usually on upper body/extremities. Amyloid is keratin-derived. Amorphous eosinophilic deposits (some)🐷 incontinence.
1
1
189
7 Dec 2023
This is a CK5/6 (of course I also got a PAS which was neg for fungi). Look @ how that material lights up! This is keratin-derived amyloid. Since there’s minimal epidermal change, I decided “c/w macular amyloid” (vs lichen).
2
16
547
22 Nov 2023
📸regulations.gov/docket/FTC-2…
Let your voice be heard on non-compete clauses by March!
#noncompete
#fairwages
1
176
22 Nov 2023
Scary!
21 Nov 2023

Can you make diagnosis on one pic, or #TooCloseToDiagnose? (yes, IRL you MUST have clinical info) What are 2 clues seen here?
Answers: kikoxp.com/posts/15540
Video: kikoxp.com/posts/4131
#pathology #pathologists #pathTwitter #dermpath #dermatology #dermatologia #dermtwitter
234