
Commentary from a coloradan parent who wants people to understand the COVID situation in Colorado. Tweets A LOT about masks. Blocks misinformation spreaders
Joined March 2021
- Tweets 22,806
- Following 866
- Followers 2,154
- Likes 79,711
4,337 Photos and videos






Pinned Tweet

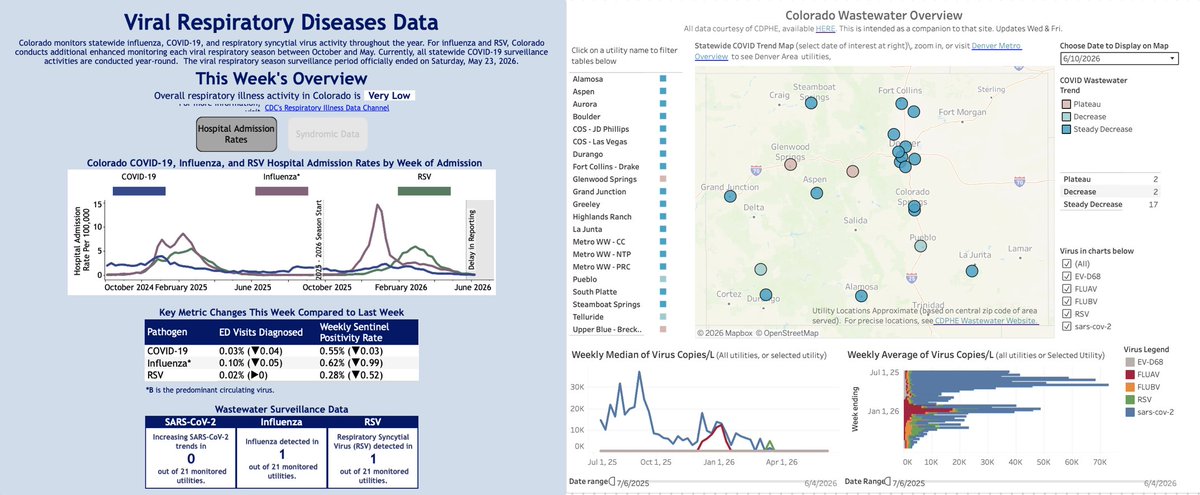
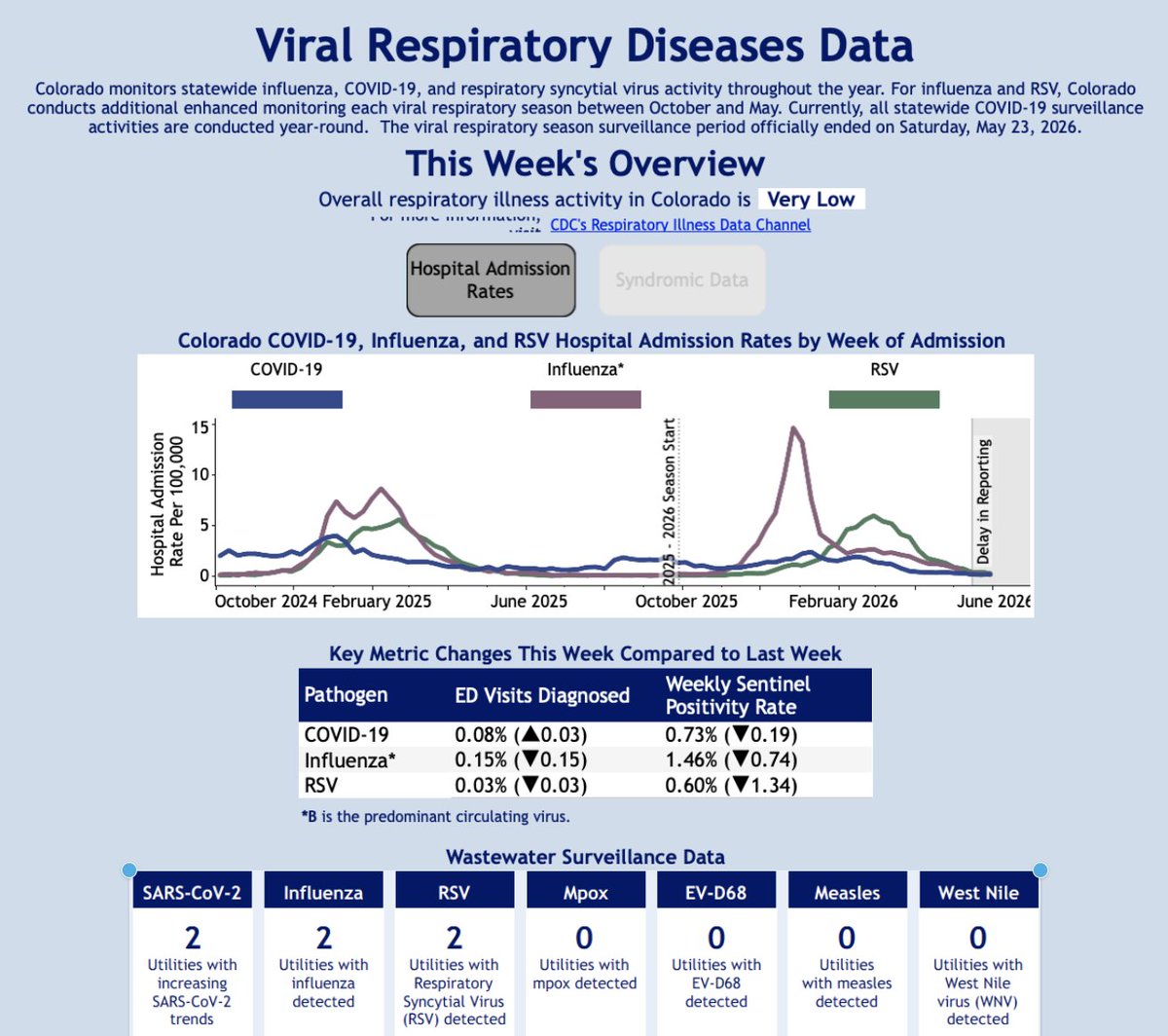
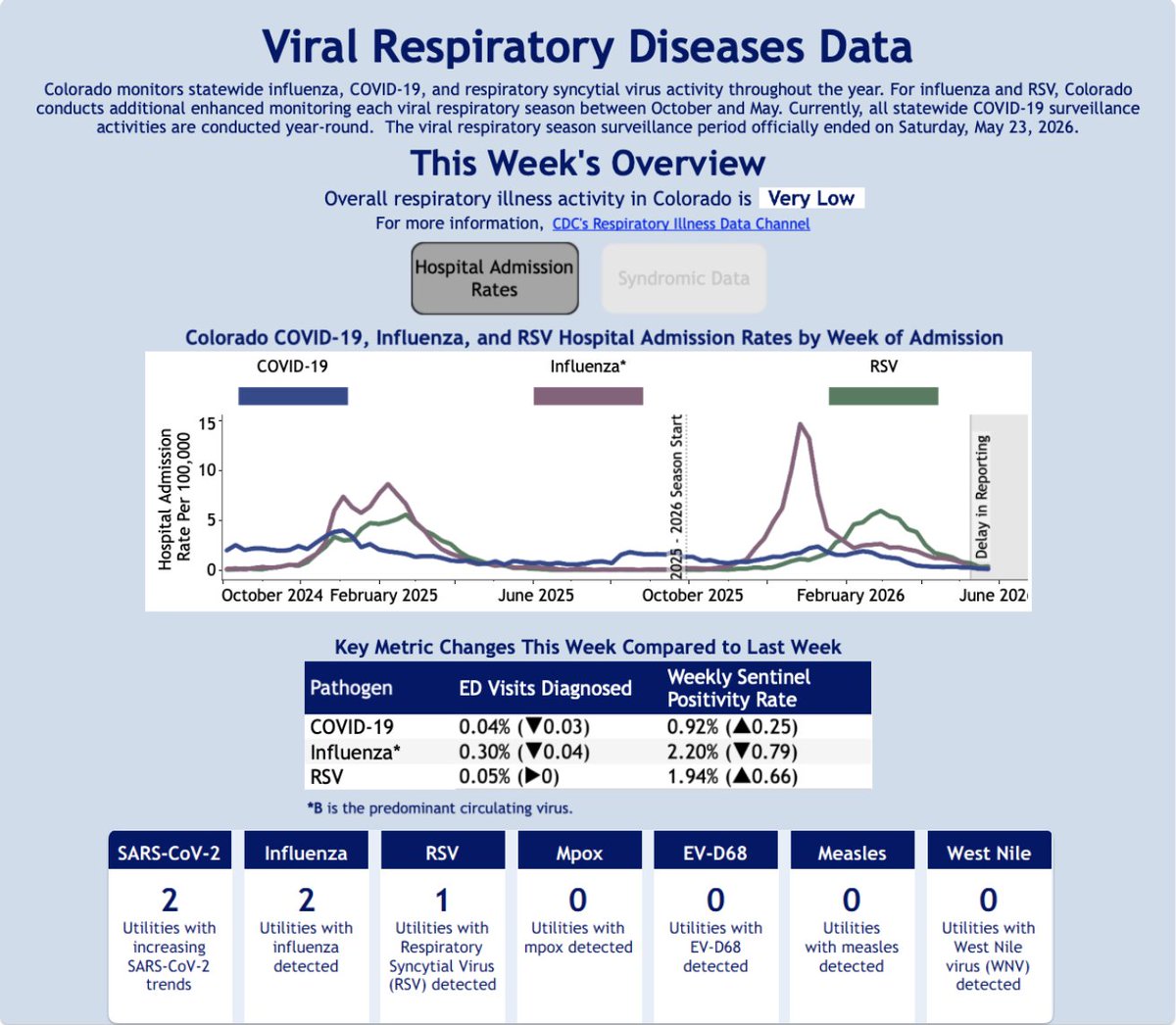
COVID, Flu & RSV in Colorado update, 6/10/26
All indicators are wildly low.
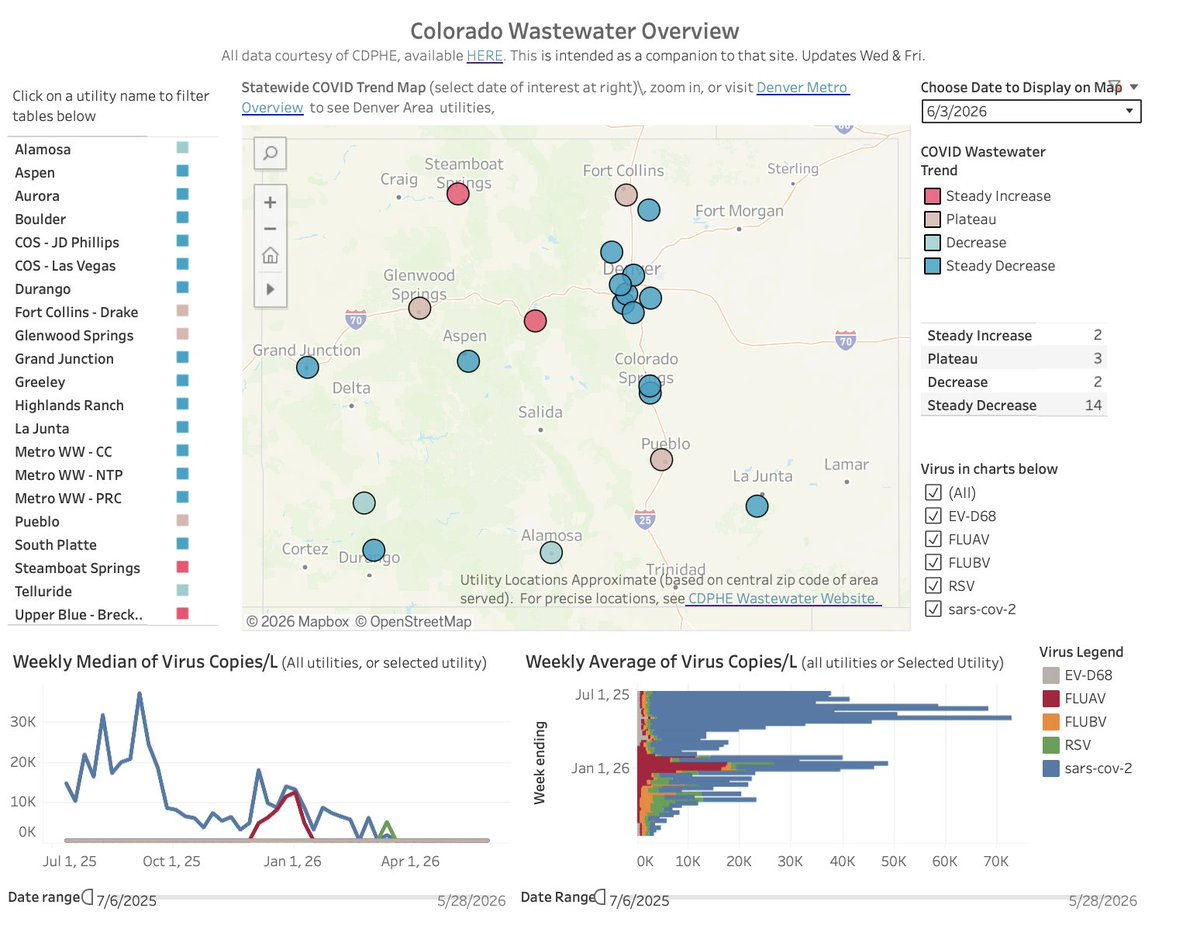
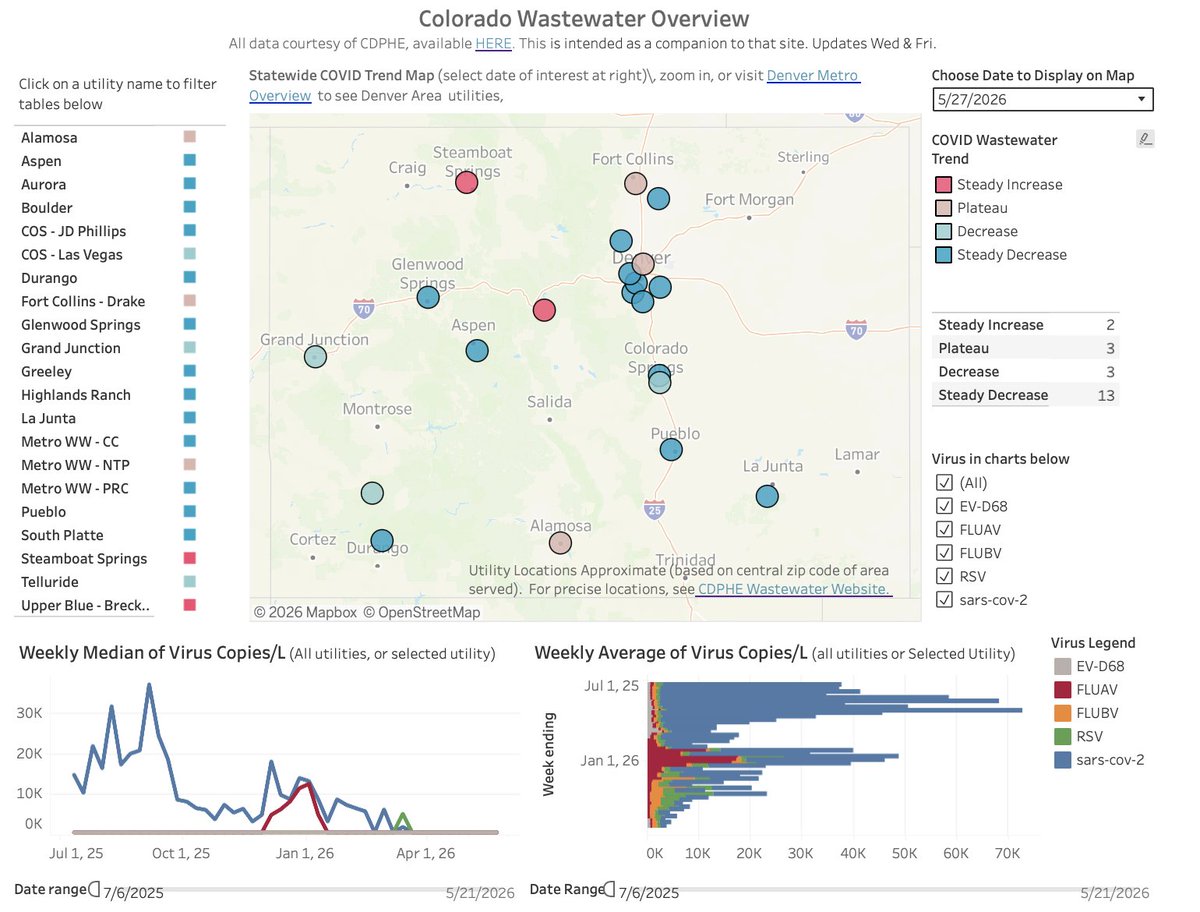
COVID Wastewater levels are lower than they have ever been. The last 2 positive detections of COVID in wastewater were on May 28.
There are no "increasing" COVID WW trends. (1st time since October)
2
3
21
649
The worst thing about following the INCREDIBLE Dr Hotez is his incessant retweets of Texas Propaganda, failing to acknowledge when it is swathed in racism.
Here, he celebrates the state borders drawn by the evil 1850 compromise that compromised slavery for westward expansion/1
1
2
75
The 1850 compromise literally required the North to return escaped slaves via the Fugitive Slave Act and extended slavery westward & for another decade.
Its one of the most evil sets of laws enacted in US history.
Theres nothing to celebrate about it.
archives.gov/milestone-docum…
1
1
5
59
Dr Hotez is one of the true mensches of this decade: expanding COVID vaccine access to LMIC countries and finding and funding treatments for high consequence global disease.
He should be attuned to the racist aspects of Texas History and choose not to propagate it.
3
61
COVID, Flu & RSV in Colorado update, 6/10/26
All indicators are wildly low.
COVID Wastewater levels are lower than they have ever been. The last 2 positive detections of COVID in wastewater were on May 28.
There are no "increasing" COVID WW trends. (1st time since October)
2
3
21
649
Hospital Admissions (comparing to initial #s for last week)
Covid: 6*, down from 8 last week
Flu: 3, down from 6
RSV: 6, down from 13
*tied for the record lowest initial number ever.
Flu hospitalizations have finally flattened out.
3
63
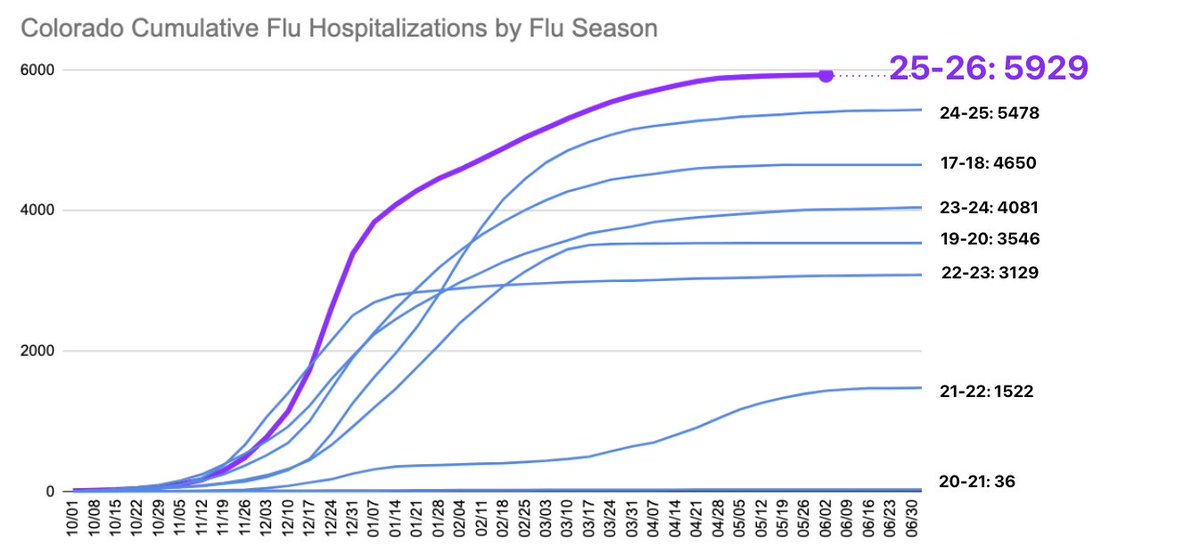
COVID, Flu & RSV in Colorado update, 6/3/26
Flu season officially comes to a close, with Flu A, Flu B, RSV, and COVID are very low in hospitalizations, wastewater, and positivity.
1
2
8
356
Hospital Admissions (comparing to initial #s for last week)
Covid: 8, up from 6 last week
Flu: 6, down from 9
RSV: 13, down from 21
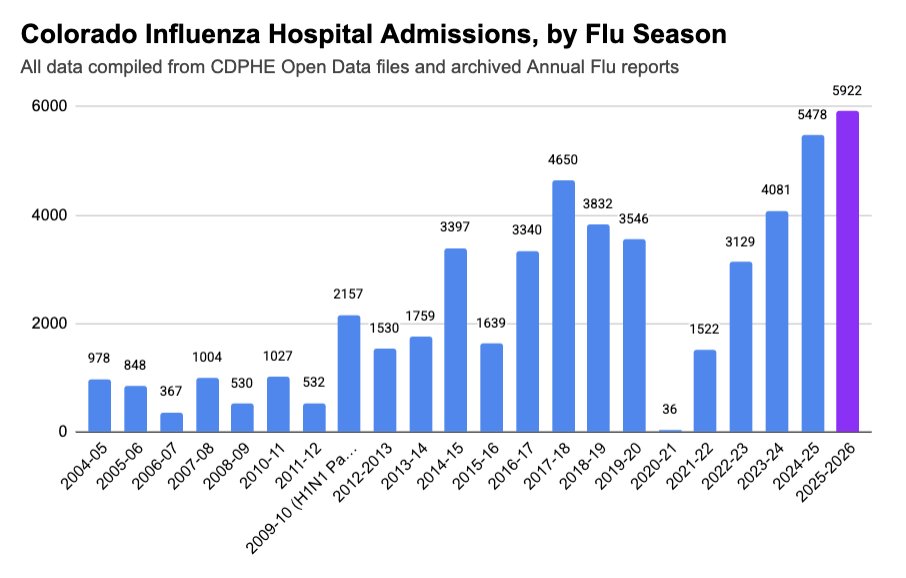
Flu Season closes with more cases in a season than ever before, breaking last year's record.
1
1
8
125
Wastewater remains in incredible lows, for all tested viruses.
There were only 4 positive samples of RSV in the entire Month of May and only 3 positive samples for Flu B in May. COVID levels remain at record lows, with only 13 positive samples of 154 in all of May.
1
9
83
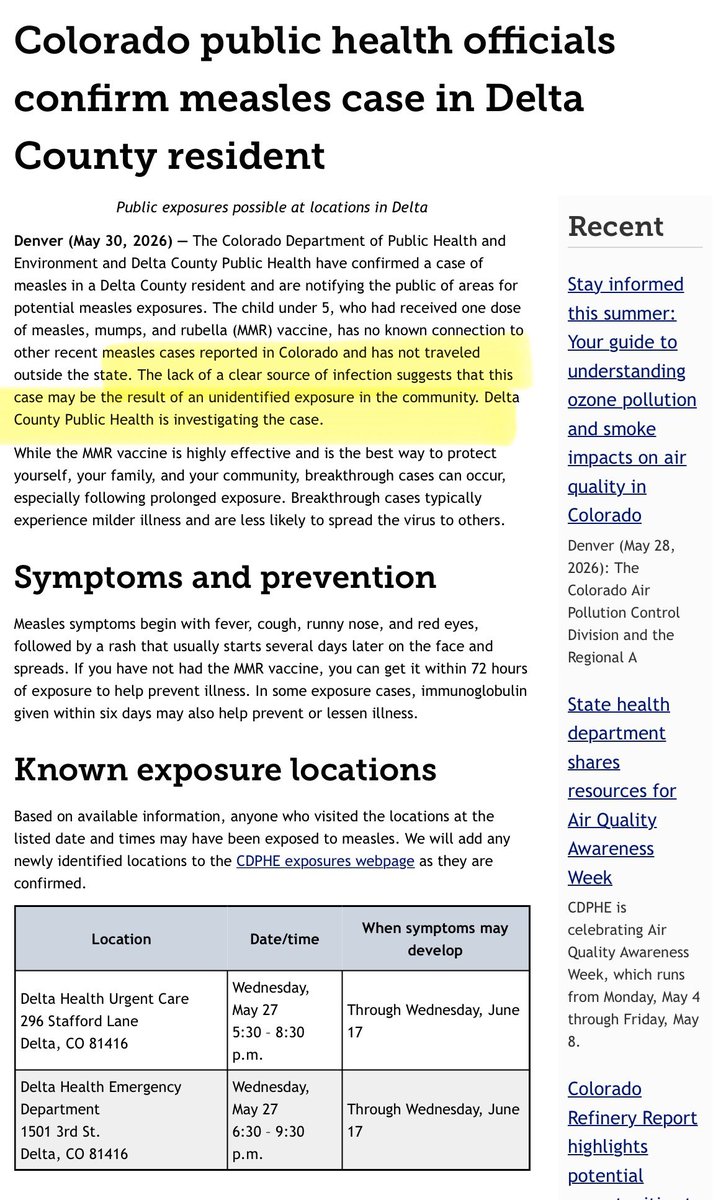
Colorado reports its 23rd case of Measles this year in a young partially vaccinated child.
The child has no known exposure and no travel, indicating there are likely unintended cases/exposures in the community.
7
17
502
Love thy neighbor: wear an N95😷 retweeted

May 30
Filtering the air may help prevent your own infection from becoming more severe
If everyone in a household becomes infected with the same virus, does it help to isolate from each other and can you be a danger to yourself? Read on to find out...🧵1/
#AirQuality #IAQ #Ventilation
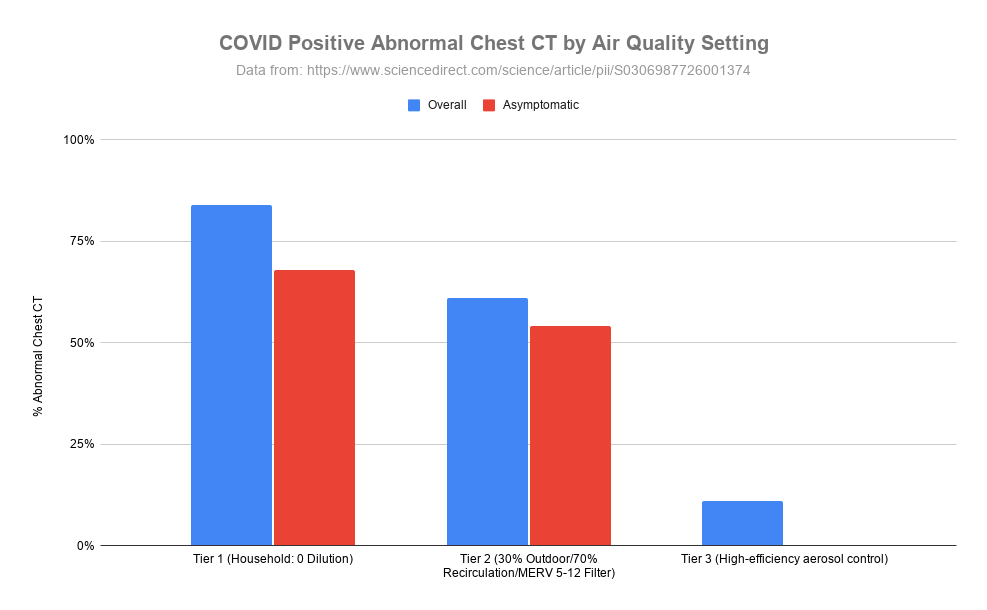
ALT This grouped bar chart, titled "COVID Positive Abnormal Chest CT by Air Quality Setting", displays the percentage of abnormal chest CT scans among COVID-positive patients across three different tiers of air quality control. The graph compares overall and asymptomatic cases, illustrating a clear downward trend in the percentage of abnormal scans as air filtration and ventilation efficiency improve from household levels to high-efficiency aerosol control.
30
307
1,009
40,449
Reminder about Polis's COVID policies:
cpr.org/2021/06/24/colorado-…
May 28

I have killed zero people, and you can take that to the bank.
6
100
Love thy neighbor: wear an N95😷 retweeted

Colorado reports a 2nd #hantavirus case, this time in an Arapahoe County adult.
The good news? It's not tied to the cruise ship outbreak.
The even better news? The man is recovering and the variant, endemic to CO, does not spread person-to-person: denver7.com/lifestyle/health…
3
10
1,846
Love thy neighbor: wear an N95😷 retweeted
French prime minister Sébastien Lecornu says several case contacts linked to the #hantavirus cruise ship outbreak have tried - unsuccessfully - to challenge the state's quarantine measures before the courts.
His response?: "The precautionary principle over the risk of spread."
May 26

Depuis plusieurs jours, face au cluster d’hantavirus détecté à bord du navire MV Hondius, le Gouvernement agit avec une seule priorité : protéger les Français.
Oui, certains cas contacts ont contesté devant la justice les mesures d’isolement préventif imposées. La justice a validé la légalité de ces décisions.
Oui, cette attente est éprouvante humainement. Mais alors que deux nouveaux passagers ont encore contracté le virus ces dernières 48 heures en Espagne et aux Pays-Bas, chacun comprend pourquoi, face à une maladie à incubation longue, relâcher la vigilance maintenant serait irresponsable.
Le choix du Gouvernement est simple : le principe de précaution plutôt que le risque de propagation.
À celles et ceux qui acceptent aujourd’hui cette contrainte, la Nation sait ce qu'elle vous doit. La solidarité d’une vingtaine de personnes contribue à protéger 66 millions de Français.
2
3
9
401
There are no less than THIRTEEN special pathogen treatment centers in the US with trained staff and proper facilities to care for Ebola patients.
They train regularly to ensure readiness to treat patients, protect staff and communities.
netec.org/about-netec/partne…

Members of the U.S. Public Health Service have already begun training at Joint Base Andrews to staff the facility, according to people familiar with the response.
One person expressed concern that the training period was only three days, which experts say is not sufficient. wapo.st/4dxCt5E
2
9
313
COVID, Flu & RSV in Colorado update, 5/27/26
*Holiday Week
The COVID lull continues.
Tiny upticks in positivity from very low levels in RSV and COVID.
COVID hospital admissions reach record lows.
1
2
8
200
Hospital Admissions (comparing to initial #s for last week)
Covid: 6*, down from 7 last week
Flu: 9 down from 14
RSV: 21, up slightly from 19
*This is the smallest initial number of COVID admissions recorded in a week since March 2020.
1
5
305
Wastewater levels of all viruses remain VERY VERY low
1
8
114
If you’re publicly whining about your right to free speech being curtailed, youre not a democrat.
If you’re doing it while complaining that a private organization is curtailing your freedom to speak at their events, you’re just a dim bulb.

Gov. Jared Polis, fresh off being censured by the Colorado Democratic Party for letting Tina Peters out of prison early, showed up today to a private, internal party call like this #copolitics

2
66
Love thy neighbor: wear an N95😷 retweeted

May 24
#hantavirus #ebola
[This interview is absolute🔥🔥🔥Worth a read. ⬇️⬇️⬇️ Excerpts: ]
➡️ The crisis of public health in the era of the COVID-19 pandemic: An interview with Arijit Chakravarty
<snip>
- What public health authorities do every time, without fail, is assume they already know. They say, “That’s hantavirus. We know what it’s like because we saw the 2018 outbreak.” But you should not count on getting the same reproductive number as 2018. That R0 is a function of population density, cultural responses, the measures taken in the initial days, all of which are different in the current context. In the Epuyén outbreak [in Argentina], R values as high as 6 were recorded at the outset, dropping to 0.9 only after controls were put in place.
- So ➡️ what you get every time is dysfunctional communication rooted in false certainty. Authorities will say, “We know what this is because we had the Epuyén outbreak—R-naught of two, case fatality rate of 30 percent.” But that ignores the total infection fatality rate. There may be many people walking around with mild hantavirus. All of this mythologizing substitutes for the honest answer, which is that you don’t know what will happen to this virus, and you don’t know what its actual R0 is when someone boards a crowded airplane for eight hours.
- There is also a genetic dimension that is being ignored. You cannot assume this is the same virus that circulated in Epuyén. The sequence data already shows significant divergence and multiple mutations. The 1918 influenza differed from its predecessors by only two nucleotides, and that was enough to drive catastrophic change. Depending on which mutations are present, even a small number of changes can produce radically different behavior in a pathogen.
- ➡️ The core failure, in every case, is that t➡️ he entire focus is on managing the public’s emotional response rather than managing the disease. Martha Lincoln and I wrote a piece several years ago titled, “The Coronavirus Doesn’t Care About Your Feelings.” Our argument was precisely this: ➡️ Managing the emotional response to a disease is not the same thing as managing the disease itself. The wrong lessons were drawn from COVID-19, and we are living through the consequences.
- BM: ➡️ What you are describing was on full display with hantavirus. ➡️ Experts across the field—virologists, epidemiologists—were almost unanimously telling the public this is not SARS-CoV-2, as though that comparison settled the question of risk. Meanwhile, on a ship of roughly 150 passengers, at least 10 percent were infected before the WHO was even notified almost a month later.
- There were almost certainly discussions between the ship and relevant stakeholders in which the decision was made to stay the course, because passengers had paid substantial sums for this expedition. The ship called at various islands, passengers disembarked and intermingled, new passengers boarded. Then a passenger collapsed in the Johannesburg airport. Given that the Andes virus has an incubation period of up to eight weeks and a serial interval of 21 days, the media’s framing of this situation was entirely inadequate. From your perspective, what should a competent public health response to the hantavirus outbreak have looked like?
- AC: ➡️ The hantavirus situation presents two possible approaches, and they could not be more different. ➡️ The first is to say: We know this virus well, it does not spread easily between people, and our job is to keep the public calm. ➡️ The second is to say: Here is a zoonotic event involving a pathogen we have not seen in an outbreak context in seven or eight years, and ➡️ we should approach it with the precautionary principle. ➡️ The contrast is between a public health response focused entirely on calm-mongering and a public health response focused on actually doing the job.
- A professional response would have acknowledged the cone of uncertainty around this virus explicitly. The R0 from the 2018 outbreak cannot be assumed to automatically apply here. The context is different: People are flying internationally, the genetic sequence of the virus has diverged, and there are multiple reasons why the 2018 R0 should not be treated as a baseline.
- Most critically, we know this virus is transmitted efficiently. The landmark 2020 New England Journal of Medicine paper on the Epuyén outbreak documented a transmission event in which two individuals simply walked past each other and exchanged brief greetings. That is either aerosol transmission or extremely efficient short-range person-to-person spread. And given what that paper shows about the birthday party super-spreading event, aerosol transmission is the more plausible explanation.
- ➡️ The appropriate default position for any novel virus should therefore be to➡️ assume aerosol transmissibility from the outset and to put measures in place immediately to limit the spread from the first known cases. That is not a radical position. It is common sense, and it is unconscionable that we are still having this argument six years after the COVID-19 fiasco.
- The COVID-19 public health failure
- ➡️ COVID-19 was a public health failure in every sense of the word. The role of public health agencies should not be to act as midwives for every emergent pathogen, gently shepherding the disease to endemicity while keeping the public calm.‼️ ➡️ That is what failure looks like. COVID-19 should never have been allowed to become endemic.
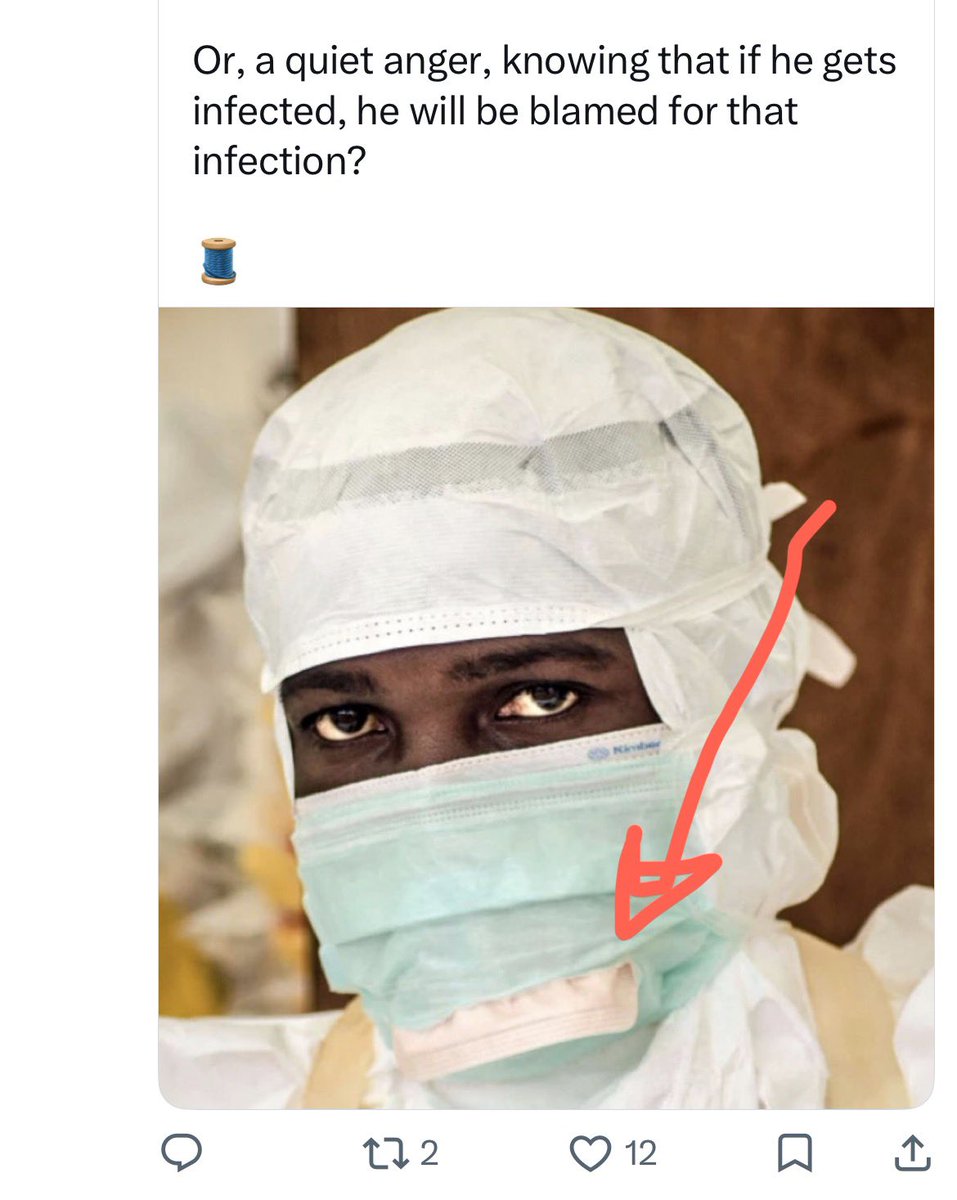
- In February 2020, there were photographs circulating from China showing healthcare workers in full hazmat suits. At the same time, we saw pictures in the newspaper of the first American patients—in a facility in Washington state—being moved around by what looked like administrators, holding up a bedsheet for the patient’s privacy, some of them wearing surgical masks. When I saw that image, it was clear to me where this was headed. ➡️ Our entire approach to infectious disease threat management was oriented around tangential concerns—HIPAA compliance, public perception—rather than preventing onward transmission.
- ➡️ With hantavirus, authorities have been discussing this outbreak in the past tense almost from the beginning, while simultaneously failing to implement any of the measures the situation required. ➡️ The CDC started out with “encouraging” passengers from the infected cruise ship to isolate. ➡️ A couple of days later, they significantly tightened their guidance, but those adjustments are meaningless once people have been circulating freely in public for any length of time. ➡️ All clichés about barn doors and horses bolting apply, of course.
<snip>
- ➡️ If we dodge this one, it will be entirely due to luck. ➡️ That is the whole of our current strategy, and it is remarkable that ➡️ there has been no serious postmortem of the failure of public health during the early stages of COVID-19. ➡️ The WHO conducted an internal review that produced a list of recommendations, but ➡️ conspicuously absent from that list was airborne protections. If you look at their website on COVID-19 even today, they still talk about practicing “respiratory etiquette” by coughing into your elbow. Without an honest assessment of the role of airborne spread, ➡️ there’s no commitment to treating the next zoonotic outbreak event as a potential pandemic threat requiring aerosol mitigations from day one.
- The lack of an honest post-mortem explains why
➡️ we are in this Groundhog Day situation, where every new outbreak triggers the same cycle: debate about whether transmission is really airborne, eventual acknowledgment that it may be, and then the implicit conclusion that because it’s airborne, nothing can be done. ‼️When a fire breaks out in your house, it’s not a good time for debate. You reach for the fire extinguisher.
- The Ebola outbreak in Central Africa
- BM: The Ebola PHEIC itself, one of the indicators driving the declaration, is exactly what you are describing on the deterministic side.➡️ Confirmed cases have appeared in Kampala and Kinshasa
➡️ among individuals with no known epidemiological links to each other, ➡️ which means community spread in two major urban centers. What is your read on this outbreak and on the WHO’s capacity to respond?
- AC: Frankly, I’m at a point now where I scrutinize everything the WHO says for their angle rather than accepting it at face value. But on this particular call, I think they are correct. ➡️ There is genuine cause for alarm, and I believe the WHO knows it. The real reason for concern is not simply that the virus has reached national capitals—It reached capital cities (Freetown and Conakry) during the 2014-2015 epidemic as well. Studies following that outbreak suggest that the official toll of roughly 30,000 infections and 11,000 deaths likely reflected somewhere between 30 and 85 percent of actual cases, meaning the true number of infections was probably closer to 100,000 or more. So that was a huge outbreak, if you think about it.
- ➡️ The real difference this time is the absence of US capacity. During the 2014-2015 outbreak, CDC scientists were on the ground managing biocontainment facilities. ➡️ During the Tom Frieden era, the CDC was the premier disease control institution in the world. That infrastructure, that institutional capacity and that willingness to engage directly; all of it is gone. ➡️ The affected countries do not have the resources to independently construct field hospitals with biocontainment capability. The WHO knows it is going to have to manage this outbreak largely alone, and that is why it has issued the PHEIC.
- ➡️ What is equally troubling is how much we don’t know about this strain. We don’t know how efficiently the Bundibugyo virus spreads by the aerosol route. We don’t know the extent of asymptomatic transmission. We don’t know what fractions of cases are mild even though mild Ebola does exist. There is no diagnostic test, no treatment and no vaccine. And this is a pathogen with a case fatality rate of 30 to 50 percent. Both the hantavirus and Ebola outbreaks deserve to be treated with maximum seriousness.
- BM: ➡️ The parallel that concerns me is also procedural. How the MV Hondius situation was handled—the delayed notification, the disembarkation of passengers without adequate screening, people being brought in for evaluation and then sent home—is now the model through which we must view the Ebola response. If the past week is any guide to the present, we should be asking if there are airport controls in place? Where have exposed individuals traveled? What contact tracing infrastructure actually exists?
➡️ Overlaying the hantavirus mismanagement onto a disease with a 30 to 50 percent fatality rate spreading in densely populated, resource-limited cities presents a genuinely alarming picture.
- AC: Yeah, exactly! ➡️ With respect to the hantavirus response, if this was a work of fiction, it would be rejected by any editor as implausible. ➡️ Why would a public health agency disembark all passengers from a vessel with a confirmed outbreak and simply allow them to disperse? ➡️ Why would individuals brought to a quarantine unit for evaluation be told they were free to go home? ➡️ The level of institutional failure is almost beyond satire. And you’re absolutely right: When you layer that track record over what is now unfolding in Kinshasa, we have a serious problem.
- What makes this moment different from 2014 and 2015 is not just the absence of US institutional capacity. ➡️ There has been a broader cultural shift, driven in no small part by the messaging of agencies like the WHO and CDC over the past six years, ➡️ in what the public and governments are willing to accept. Quarantine laws have been weakened in multiple US states. Contact tracing infrastructure has been systematically dismantled.
<snip>
- ➡️ On Ebola specifically, there’s one thing about this that’s different from previous outbreaks. ➡️ It is very difficult to calm-monger a disease that produces hemorrhagic fever. Everyone has seen the images. No one is indifferent to a 30 to 50 percent fatality rate. Ryan Gregory and I wrote a blog post on the logic of calm-mongering as a systematic public health strategy. ➡️ The playbook begins with “more information is needed,” progresses to emotional management, and ends with making risk discussion itself undiscussable. ➡️ The minute anyone raises the question of mitigation they are accused of fearmongering. It is as though every time you reach for a fire extinguisher, someone stops you to debate whether a fire could realistically break out in this particular kitchen. Ebola will test whether that playbook can survive contact with a visibly catastrophic disease.
- A convergence of crises
- BM: We are dealing with this convergence of crises—COVID-19 still ongoing, H5N1, Mpox, hantavirus, Ebola and now a measles resurgence driven by the systematic dismantling of vaccination infrastructure and the deliberate reframing of public health as a matter of individual choice. This is not a calamity approaching. It is already underway.
- AC: Absolutely, I couldn’t have said it better! To your point, the COVID-19 public health failure seeded all of this in three distinct ways, and it’s worth being precise about each one.
- The first is institutional. ➡️ Governments and international bodies have concluded that they can manage any infectious disease outbreak through communication alone or that talking the public through a crisis is equivalent to controlling it.‼️ In a very real sense, institutionalized public health now works to undermine actual public health. ➡️ Agencies spread misinformation. ➡️ They make it harder for individuals to protect themselves. ➡️ The explicit demonization of masking is the clearest example. ⚠️ When the chief public health officer of British Columbia describes the PPEs (personal protective equipment) as “that word that we all dread to hear,” that is just a straight-up abdication of the most basic professional responsibility.
- The second is immunological. ➡️ Repeated COVID-19 infections are producing population-level immune impairment. The “airborne AIDS” framing is a straw man; it does not require that level of devastation to matter. It’s well established at this point that COVID-19 infections cause lymphocytopenia (white blood cell loss). People who don’t take precautions for COVID-19 can expect to get it once or twice every two years or so. Every infection takes a bite out of your white blood cell population, and recovery can take six months or more. A transiently weakened immune response across a large section of the population creates exactly the conditions of vulnerability that pathogens exploit. The combination of recurring COVID-19 reinfection and collapsing vaccination coverage means we are entering these new outbreaks with a population whose baseline immune competence is lower than it was in 2019.
- ➡️ The third is behavioral. ➡️ The deliberate mismanagement of COVID-19 has produced ➡️ a public that is substantially less willing to mask, less willing to take quarantine seriously, and less willing to recognize the social obligation not to infect others. The MV Hondius situation illustrated this with extraordinary clarity. One passenger fled the ship and transited through four major international airports to reach Pitcairn Island before being located and isolated. Another flew to Hanoi to attend an extreme travelers conference, an event populated by people whose defining characteristic is that they travel the entire globe continuously. If this were submitted as a plot point in a novel, it would be rejected as unbelievable. This is the behavioral landscape in which we are now trying to contain both hantavirus and Ebola.
- BM: There is another dimension that compounds all of this: ➡️ the relationship between armed conflict and infectious disease. We are seeing polio reestablish in Gaza and resurface in the United States. Ebola is now spreading in the DRC, an active conflict zone with resource-rich territory and desperately poor access to those resources for its civilian population. History is unambiguous on this point; 1918 influenza and World War I are canonical examples. We are in a period of perpetual wars, where political and economic impasses are managed by armed conflict.
- AC: I agree. ➡️ War and disease are fellow travelers. That historical parallel is entirely apt, and the current geopolitical situation is worse in terms of active conflicts than anything we faced 10 years ago. The implications are direct and serious. We addressed this in a Scientific American piece on H5N1. The consistent message has been that the precautionary principle is not optional. The claim that “we dodged the bullet” on bird flu is simply false. H5N1 continues to circulate in poultry flocks across the United States, and zoonotic spillover events are ongoing.
- ➡️ The history of 1918 influenza is instructive here. That virus smoldered in swine herds and poultry flocks for approximately a decade before it produced a pandemic. Because influenza has a segmented genome, the large pools of genetic variation circulating in animal reservoirs provided the raw material for increased transmissibility in swine, which in turn generated the mutations that combined with existing human seasonal influenza to produce the 1918 strain. ➡️ The final pandemic-capable variant emerged as essentially a single-step jump, but ➡️ that jump was only possible because of the vast genetic diversity that had accumulated over years compounded by the fire set by the war effort. ➡️ What we are doing by tolerating H5N1’s continued spread in animal reservoirs is allowing the virus to take unlimited potshots at the human population. ➡️ Relying on luck is a strategy—if you can call it that—with a mathematically guaranteed endpoint: If you wait long enough, your luck will run out.
- ➡️ The structural problem underlying all of this is the consistent ➡️ abandonment of the precautionary principle. Early containment of an emergent pandemic is extraordinarily low-cost relative to what follows once containment fails. We no longer have a meaningful contact-tracing infrastructure. The COVID-19 experience demonstrated definitively that once a pathogen escapes the initial containment window, contact tracing at the population level becomes impossible. And ➡️ the communication framework remains entirely wrong. Describing hantavirus to the public as something you only need to worry about if you are inhaling rodent feces is misinformation. The Andes strain transmits human to human, which is a fact, and the official messaging contradicted it from the outset. Calling an infectious disease “rare” is not a scientific statement. It is a policy choice. A disease will be rare or not rare depending on the decisions a public health agency makes about containment.
<snip>
AC: ➡️ The right lessons from COVID-19 were identifiable from very early in the pandemic, and none of them were learned. ➡️ The first was to improve indoor air quality (IAQ) as a permanent infrastructure investment and not a crisis response. The baseline analogy to this public health standard is equivalent to the history behind access to clean public water. By my estimate, you could upgrade indoor air quality in every public building in the United States, to the point where airborne transmission was significantly mitigated, for roughly cost of a single aircraft carrier. Six years later, not only has that not been done, we haven’t even had a public conversation about the cost-benefit of better IAQ in public spaces.
- ➡️ The second was to ➡️ communicate honestly and precisely about risk and ➡️ not to manage emotional responses but to give the public accurate information and the tools to act on it.
- The third was to ➡️ establish, as a standing protocol, that every new zoonotic outbreak event is to be treated as a potential aerosol-transmissible threat until proven otherwise. That default doesn’t require certainty. It requires only that we stop assuming the best case. There’s a reason you’re not supposed to play with roadkill—It’s not because if you do, you will pick up an infection. It’s because you might. And that “might” is enough to stop most people.
- Beyond those principles, the critical operational failure in both the hantavirus and Ebola responses has been the sequencing of priorities. In the early days of any outbreak, public health’s first obligation is to establish testing and get contact tracing operational or to put a ring around the initial cases before anything else happens. Instead, ➡️ what we have seen repeatedly is an immediate pivot to press conferences and public messaging, with contact tracing and isolation protocols backfilled weeks later when they can no longer accomplish anything. ➡️ It is outlandish to be debating the basics of containment protocol a month into an outbreak. These frameworks should have been designed, tested and institutionalized years ago.
- The deeper consequence of refusing to learn from COVID-19 is that the public has been led to believe that the problem with the COVID-19 response was that any mitigation measures existed at all. That is precisely the inversion of the truth. ➡️ The problem was that mitigation measures were deployed too slowly, abandoned too quickly, and never given the institutional backing that would have made them effective. Until there is genuine accountability for what went wrong—not public relations exercises but honest institutional reckoning—we will continue cycling through these emergencies with the same tools, the same assumptions and the same outcomes.
That disproportion between the cost of prevention and the cost of failure extends to the broadest possible frame. We are at a demographic and epidemiological inflection point that is not well understood.➡️ For more than a century, humanity has steadily reduced the burden of infectious disease, the primary predator of our species for most of recorded history. Walk through any old cemetery in the Northeastern United States and you will find a children’s section, full of graves of two- and three-year-olds taken by infectious disease. The suppression of that mortality has been one of the central drivers of population growth. ➡️ We have built a civilization premised on the assumption that we have won against infectious disease.
- ➡️ We have not. What we have done is create the conditions for a fresh wave of pathogens to encounter an enormous, globally connected, immunologically vulnerable population. The analogy to water sanitation is precise: Cleaning the water supply allowed us to eliminate cholera and other waterborne diseases as mass killers. Addressing airborne transmission with equivalent seriousness is the next necessary step, because the pandemic-potential pathogens we are now facing are overwhelmingly airborne. The systematic refusal to acknowledge this—the insistence among some epidemiologists that “airborne” means only measles-level transmissibility—is not a scientific position. It is a liability management strategy. And it cannot be sustained indefinitely without catastrophic consequences.
- You asked me for a closing comment, so I would put it this way. ➡️ Public health in the 21st century has one paramount obligation: to prevent new infectious diseases from establishing themselves in the human population. Every pathogen that succeeds in making that transition to endemicity, as COVID-19 unfortunately did, weakens our collective defenses against the next one. If we let measles re-establish, it causes immune amnesia, where your immune system becomes weaker, for several years. ➡️ Each new disease establishing itself in the human population makes the population less healthy, more vulnerable to other diseases. The whole game, properly understood, is to reduce the total burden of infectious disease. Everything else that public health does—wellness campaigns, screen-time guidance, lifestyle interventions—they can skip. It’s right of the decimal point. If they fail at that primary obligation, none of the rest of it matters.
By Benjamin Mateus
wsws.org/en/articles/2026/05…
5
9
32
1,592