
Validating AI in classifying colorectal cancer in real-time surgery. Funded by @HorizonEU. Tweets reflect only the views of the project owner.
Joined May 2022
- Tweets 670
- Following 777
- Followers 939
- Likes 707
282 Photos and videos













Pinned Tweet

5 Sep 2022
🇪🇺 CLASSICA | Validating AI in Classifying Cancer in Real-Time Surgery
💡 Five leading cancer surgery centres across Europe will treat 500 patients during the project.
Check out our website to learn more
👉 classicaproject.eu/
#HorizonEU #classica #ai #colorectal #cancer
2
9
26
Jun 14
Training is an important part of CLASSICA's dissemination work. Coordinator Prof Ronan Cahill joined the European Society of Surgical Oncology (ESSO) - International Society for Fluorescence Guided Surgery (ISFGS) Course in Leiden on 11th June 2026, where he spoke about the kinetics of fluorescence in cancer imaging.
#HORIZONEU #SurgicalInnovation
37
Mar 12
Read our summary of a @classicaproject study in the Journal of Law and the Biosciences examining whether Europe's landmark AI law will actually make AI systems fairer—particularly in healthcare. Authors Emilia Niemiec, Peter A E Davis (both at CeBIL, @UCPH_Research), and Mathias K Hauglid (Wikborg Rein Advokatfirma AS) take a close look at the EU AI Act's rules around training data, asking whether they're strong enough to tackle one of AI's most persistent problems: biased datasets.
🔗classicaproject.eu/2026/03/k…
1
3
67
CLASSICA retweeted

Great to see @classicaproject featured in the European Commission #Science4EU portal: research-and-innovation.ec.e… @UCDMedicine @ucddublin
1
1
5
180
Mar 9
🔬 New Surgical Endoscopy publication summary from the @classicaproject team, 𝑷𝒆𝒓𝒊𝒕𝒐𝒏𝒆𝒂𝒍 𝒐𝒑𝒆𝒏𝒊𝒏𝒈 𝒅𝒖𝒓𝒊𝒏𝒈 𝒕𝒓𝒂𝒏𝒔𝒂𝒏𝒂𝒍 𝒆𝒏𝒅𝒐𝒔𝒄𝒐𝒑𝒊𝒄 𝒎𝒊𝒄𝒓𝒐𝒔𝒖𝒓𝒈𝒆𝒓𝒚: 𝒄𝒂𝒏 𝒑𝒓𝒆𝒐𝒑𝒆𝒓𝒂𝒕𝒊𝒗𝒆 𝒑𝒐𝒔𝒊𝒕𝒊𝒐𝒏𝒊𝒏𝒈 𝒂𝒔𝒔𝒆𝒔𝒔𝒎𝒆𝒏𝒕 𝒊𝒎𝒑𝒓𝒐𝒗𝒆 𝒊𝒏𝒕𝒓𝒂𝒐𝒑𝒆𝒓𝒂𝒕𝒊𝒗𝒆 𝒎𝒂𝒏𝒂𝒈𝒆𝒎𝒆𝒏𝒕?
Peritoneal opening during TEM/TEO surgery is largely predictable, and when well-managed, doesn't increase overall patient risk. Important findings for safer surgical planning. 🏥
👉 @albertoarezzo, Ammirati, Distefano et al., @unito
#MinimallyInvasiveSurgery #Colorectal #TEM #KnowledgeUnwrapped
📚 classicaproject.eu/2026/03/k…
2
3
82
CLASSICA retweeted
Now published open access online @SurgEndosc “Perioperative splanchnic perfusion variation around colorectal surgery using both indocyanine green spectrophotometry and fluorescence angiography” @ucdmedicine @jeffreydalli @Ashokk_s
access via the link…links.springernature.com/f/a…~
3
5
366
Mar 2
🩺 New evidence in #TEM surgery
What predicts peritoneal opening during transanal endoscopic microsurgery—and does patient positioning matter? A Feb 2026 study in Surgical Endoscopy from @unito (@albertoarezzo et al.) shows that peritoneal opening during TEM is anatomically predictable based on lesion features and positioning.🔎 Key takeaways:
• Predictable risk based on anatomy & positioning
• Higher conversion rates & longer LOS
• No significant increase in morbidity when promptly recognised and managed👨⚕️ Authors: Alberto Arezzo, Carlo Alberto Ammirati, Giovanni Distefano, Michele Barbiero, Simone Arolfo, Mario Morino
📖 Read more 👉🏽 classicaproject.eu/2026/03/c…
🔗 Article 👉🏽 link.springer.com/article/10…
#ColorectalSurgery #MinimallyInvasive #SurgicalEndoscopy #PatientSafety #TEM
2
2
134
Feb 25
In an August 2025 🇪🇺 @classicaproject publication in npj Digital Medicine, '𝑬𝒏𝒂𝒃𝒍𝒊𝒏𝒈 𝒔𝒆𝒄𝒖𝒓𝒆 𝒂𝒏𝒅 𝒔𝒆𝒍𝒇 𝒅𝒆𝒕𝒆𝒓𝒎𝒊𝒏𝒆𝒅 𝒉𝒆𝒂𝒍𝒕𝒉 𝒅𝒂𝒕𝒂 𝒔𝒉𝒂𝒓𝒊𝒏𝒈 𝒂𝒏𝒅 𝒄𝒐𝒏𝒔𝒆𝒏𝒕 𝒎𝒂𝒏𝒂𝒈𝒆𝒎𝒆𝒏𝒕,' CLASSICA PI @TiMinCeBIL, @CeBIL_Center, @UCPH_Research, with co-authors Cindy Welzel, TU Dresden, Max Ostermann, Technische Universität Dresden, Hannah Louise Smith, University of Copenhagen (Københavns Universitet), @toralf_kirsten, Leipzig University, and Stephen Gilbert, Technische Universität Dresden, presented a conceptual framework for secure and self-determined health data sharing, discussing how emerging digital technologies can support trustworthy consent management. This research aims to explore how people can gain meaningful control over how their health data, which can be generated by apps and wearable devices, is shared and used for healthcare and research.
Why is this research important? Check out our easy-to-digest, “Knowledge Unwrapped” summary 👉🏽 classicaproject.eu/2026/02/k…
1
3
55
Feb 19
How does the EU AI Act address dataset quality and bias in AI systems, and what are the practical and legal implications of these provisions—particularly regarding data governance, the "debiasing exception" for sensitive data, and enforcement mechanisms? ⚖️
Authors of the Journal of Law and the Biosciences article, "𝑾𝒊𝒍𝒍 𝒕𝒉𝒆 𝑬𝑼 𝑨𝑰 𝑨𝒄𝒕 𝒉𝒆𝒍𝒑 𝒕𝒐 𝒎𝒊𝒕𝒊𝒈𝒂𝒕𝒆 𝒅𝒂𝒕𝒂𝒔𝒆𝒕 𝒃𝒊𝒂𝒔 𝒊𝒏 𝒎𝒆𝒅𝒊𝒄𝒂𝒍 𝑨𝑰?", @classicaproject researcher Emilia Niemiec, @CeBIL_Center, University of Copenhagen, Peter Davis, CeBIL, U of Copenhagen, and Mathias K. Hauglid, Wikborg Rein Advokatfirma AS, examine how Europe's new AI law tries to make AI systems fairer by setting rules about the data used to train them, requiring representative datasets and even allowing use of highly-protected sensitive data specifically to fix bias problems. The authors analysed whether these rules will work in practice, especially in medical AI, given the tension between accessing data to check for bias and protecting patient privacy.
Read on 👉classicaproject.eu/2026/02/c…
2
2
55
Feb 17
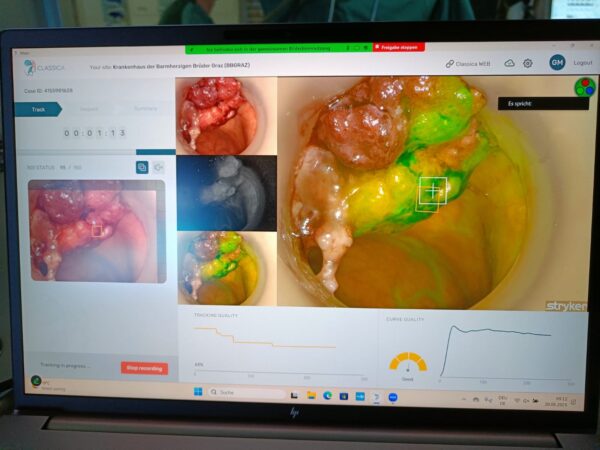
📣 Publication news! @CLASSICAproject explores how AI analysis of fluorescence perfusion can support in-situ classification of significant rectal polyps.
📄 "𝑨𝒓𝒕𝒊𝒇𝒊𝒄𝒊𝒂𝒍 𝒊𝒏𝒕𝒆𝒍𝒍𝒊𝒈𝒆𝒏𝒄𝒆 𝒄𝒍𝒂𝒔𝒔𝒊𝒇𝒊𝒄𝒂𝒕𝒊𝒐𝒏 𝒐𝒇 𝒓𝒆𝒄𝒕𝒂𝒍 𝒏𝒆𝒐𝒑𝒍𝒂𝒔𝒊𝒂 𝒃𝒚 𝒆𝒏𝒅𝒐𝒔𝒄𝒐𝒑𝒊𝒄 𝒇𝒍𝒖𝒐𝒓𝒆𝒔𝒄𝒆𝒏𝒄𝒆 𝒑𝒆𝒓𝒇𝒖𝒔𝒊𝒐𝒏 𝒂𝒏𝒂𝒍𝒚𝒔𝒊𝒔" by @PtrckBlnd et al. in @SciReports classicaproject.eu/2026/02/c…
#HorizonEU #AI #colorectalcancer
5
6
266
Feb 16
What can legal precedents from surgical technology adoption teach us about preserving patient autonomy through informed consent as AI diagnostic and decision-support tools become standard of care? In a Perspective titled, 𝑳𝒆𝒈𝒂𝒍 𝒊𝒎𝒑𝒍𝒊𝒄𝒂𝒕𝒊𝒐𝒏𝒔 𝒐𝒇 𝑨𝑰 𝒔𝒕𝒂𝒏𝒅𝒂𝒓𝒅 𝒐𝒇 𝒄𝒂𝒓𝒆 𝒊𝒏𝒕𝒆𝒈𝒓𝒂𝒕𝒊𝒐𝒏 𝒐𝒏 𝒑𝒂𝒕𝒊𝒆𝒏𝒕𝒔’ 𝒊𝒏𝒇𝒐𝒓𝒎𝒆𝒅 𝒄𝒐𝒏𝒔𝒆𝒏𝒕: 𝒍𝒆𝒔𝒔𝒐𝒏𝒔 𝒇𝒓𝒐𝒎 𝒔𝒖𝒓𝒈𝒆𝒓𝒚, by Mindy N. Duffourc @MND_Law, Maastricht University and @classicaproject Coordinator Professor Dr @RonanCahill15, @ucddublin, published in @npjDigitalMed, legal cases addressing consent and surgical innovation provide a framework for understanding how AI integration, particularly diagnostic and clinical decision-support tools, will affect the informed consent process and patient autonomy.
👉classicaproject.eu/2026/02/c…
1
2
3
339
Feb 13
Can AI Measure Surgical Skill? CLASSICA Says Yes.
Knowledge Unwrapped: 🇪🇺 @classicaproject researchers used computer vision to analyse how surgeons place stitches, investigating whether AI can objectively measure suturing quality. Testing three surgical platforms across different experience levels, the team discovered that irregular stitch spacing correlates with weaker sutures. While spatial patterns alone can't fully predict suture strength, this breakthrough moves us closer to intelligent surgical systems that provide real-time feedback during operations, transforming both training and quality assurance.
Lead author Professor @albertoarezzo and @unito colleagues just published this pivotal research in Surgical Endoscopy: "𝑭𝒓𝒐𝒎 𝒑𝒓𝒆𝒄𝒊𝒔𝒊𝒐𝒏 𝒕𝒐 𝒔𝒕𝒓𝒆𝒏𝒈𝒕𝒉: 𝒄𝒐𝒎𝒑𝒖𝒕𝒆𝒓 𝒗𝒊𝒔𝒊𝒐𝒏 𝒇𝒐𝒓 𝒔𝒖𝒕𝒖𝒓𝒆 𝒒𝒖𝒂𝒍𝒊𝒕𝒚 𝒂𝒔𝒔𝒆𝒔𝒔𝒎𝒆𝒏𝒕—𝒂𝒏 𝒆𝒙 𝒗𝒊𝒗𝒐 𝒑𝒊𝒍𝒐𝒕 𝒔𝒕𝒖𝒅𝒚."
Read the open-access paper in Surgical Endoscopy, or our lay summary ⚡: classicaproject.eu/2026/02/k…
1
2
71
CLASSICA retweeted

Feb 10
I am truly proud of this study—not only for its results, but for the direction it points to.
With this work, we show that computer vision–derived spatial metrics of suturing can be meaningfully linked to real mechanical performance (burst pressure). Spatial features alone are not yet sufficient as standalone predictors of suture quality—but that is not the main message.
The real takeaway is that precision can be quantified, compared, and ultimately automated.
This, in my view, is the real turning point for robotic surgery—including laparoscopic robotics.
The future is not about vaguely claiming “greater precision.” The real breakthrough will come when the robot itself is able to plan and execute optimal trajectories autonomously, completing a suture in true task autonomy.
Crucially, this autonomy must be human-in-the-loop:
the robot operates autonomously, but always under human supervision and control, with the surgeon retaining authority, responsibility, and the ability to intervene at any time. This is not about replacing the surgeon—it is about augmenting human skill with measurable, reproducible precision.
This is the approach robotic surgery advocates should take to demonstrate real value in the operating room:
•quantitative metrics,
•verifiable automation,
•objectively demonstrable technical benefits,
rather than generic statements about precision.
At MITIC-Lab, we believe this circle can close very soon. Within the year, at least in the laboratory setting, we expect to see genuine integration of automated routines into robotic surgical gestures.
At that point, the benefit of robotic technology will no longer be a matter of opinion.
It will be evidence-based.
Research on surgical automation is now becoming truly exciting, concrete, and useful. And this is only the beginning.
1
1
38
Feb 9
Can spatial metrics of suture placement quantitatively reflect mechanical performance, and how do operator experience and surgical platform influence technical outcomes in minimally invasive surgery? In the @classicaproject publication, authors Roberto Spagnulo, Francesco Marzola, Federica Corso, Giovanni Distefano, Matteo Pescio, Kengo Hayashi, Federica Barontini, Giulio Dagnino, Kaspar Althoefer, Bruno Siciliano, Sebastien Ourselin, and PI Professor @albertoarezzo of the @unito evaluated whether computer vision-derived spatial features of suture placement could predict mechanical strength (measured by burst pressure) across three surgical platforms with surgeons of varying experience levels. While spacing irregularity showed negative correlation with burst pressure, spatial metrics alone proved insufficient as standalone predictors of suture quality, though the approach shows potential for developing real-time feedback systems for surgical training and quality assurance. This paper, 𝑭𝒓𝒐𝒎 𝒑𝒓𝒆𝒄𝒊𝒔𝒊𝒐𝒏 𝒕𝒐 𝒔𝒕𝒓𝒆𝒏𝒈𝒕𝒉: 𝒄𝒐𝒎𝒑𝒖𝒕𝒆𝒓 𝒗𝒊𝒔𝒊𝒐𝒏 𝒇𝒐𝒓 𝒔𝒖𝒕𝒖𝒓𝒆 𝒒𝒖𝒂𝒍𝒊𝒕𝒚 𝒂𝒔𝒔𝒆𝒔𝒔𝒎𝒆𝒏𝒕—𝒂𝒏 𝒆𝒙 𝒗𝒊𝒗𝒐 𝒑𝒊𝒍𝒐𝒕 𝒔𝒕𝒖𝒅𝒚, was published on December 4, 2025, in Surgical Endoscopy.
Read the paper 👉link.springer.com/article/10…
2
3
6
89
CLASSICA retweeted
Jan 21
🇵🇹 Today we meet in the beautiful Porto for day 1 of the @CLASSICAproject plenary meeting.
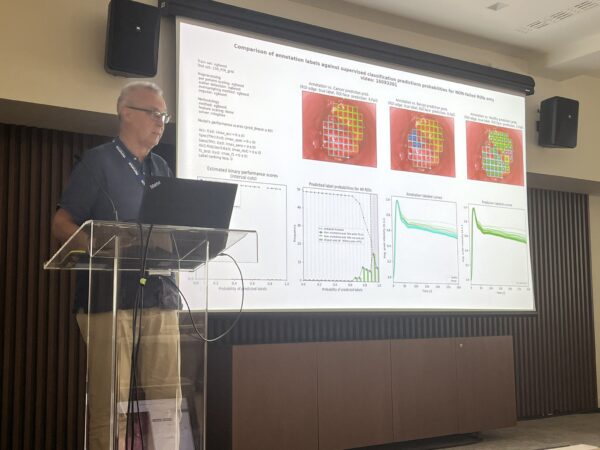
We will open the meeting with discussions on our #AI classifier and results from in-situ endoscopic classification of rectal neoplasia.
🔗 Check out our recent article in press, 𝑨𝒓𝒕𝒊𝒇𝒊𝒄𝒊𝒂𝒍 𝒊𝒏𝒕𝒆𝒍𝒍𝒊𝒈𝒆𝒏𝒄𝒆 𝒄𝒍𝒂𝒔𝒔𝒊𝒇𝒊𝒄𝒂𝒕𝒊𝒐𝒏 𝒐𝒇 𝒓𝒆𝒄𝒕𝒂𝒍 𝒏𝒆𝒐𝒑𝒍𝒂𝒔𝒊𝒂 𝒃𝒚 𝒆𝒏𝒅𝒐𝒔𝒄𝒐𝒑𝒊𝒄 𝒇𝒍𝒖𝒐𝒓𝒆𝒔𝒄𝒆𝒏𝒄𝒆 𝒑𝒆𝒓𝒇𝒖𝒔𝒊𝒐𝒏 𝒂𝒏𝒂𝒍𝒚𝒔𝒊𝒔 nature.com/articles/s41598-0…
@EU_HaDEA #HorizonEU
4
5
244
Jan 27
#AI is transforming healthcare, but who's liable when it gets a diagnosis wrong?
Professor @gerke_sara's @classicaproject research on "nutrition labels" for AI medical devices is sparking crucial conversations in @MedEconomics and beyond about transparency, accountability, and the future of medical malpractice.
Read a recap of the recent media flurry ❄️ here: classicaproject.eu/2026/01/p…
1
2
45
CLASSICA retweeted

Focus. Cancro colon-retto. Chirurgia e screening con robotica ed Intelli... youtu.be/nSfSp4fQ5hQ?si=3YPg… via @YouTube
1
2
3
119
Jan 20
🇪🇺 Tomorrow we meet in Porto for the next @CLASSICAproject plenary meeting!
Thank you to @EAES_eu for graciously hosting us. Nearly four years on, there’s still plenty to discuss on the clinical use of AI for perfusion assessment.
#HorizonEU #HealthTech #SIS2026

3
6
314
Jan 19
Digital health tools generate massive amounts of sensitive data, but without transparent consent mechanisms, people won't share it, limiting care & research potential. New framework in @npjDigitalMed explores how blockchain, self-sovereign identity & de-identified tokens can enable secure, self-determined health data sharing.
Building trust is key to unlocking digital health's promise while protecting privacy.
classicaproject.eu/2026/01/c…
1
4
214
Jan 14
The @classicaproject has been mentioned in the 2025 Annual Report of the European Association for Endoscopic Surgery (@EAES_eu ) by President-elect Professor Dr @albertoarezzo, @unito 🇮🇹, who serves as Principal Investigator for the CLASSICA project.
This recognition in the EAES Annual Report highlights the significance of CLASSICA's work within the endoscopic surgery community and underscores the project's contribution to advancing the field.
We extend our sincere thanks to Alberto for his continued leadership and support, and for bringing CLASSICA to the attention of the wider EAES membership through this important annual publication.
Read more: classicaproject.eu/2026/01/c…
1
6
193