Electrophysiologist @OKHeartHospital @HeartRhythmOHH | @theArrhythmics ICD Support Group | Recreational Basketball Player
Joined December 2008
- Tweets 5,278
- Following 911
- Followers 1,138
- Likes 1,649
881 Photos and videos





Pinned Tweet

14 Sep 2021
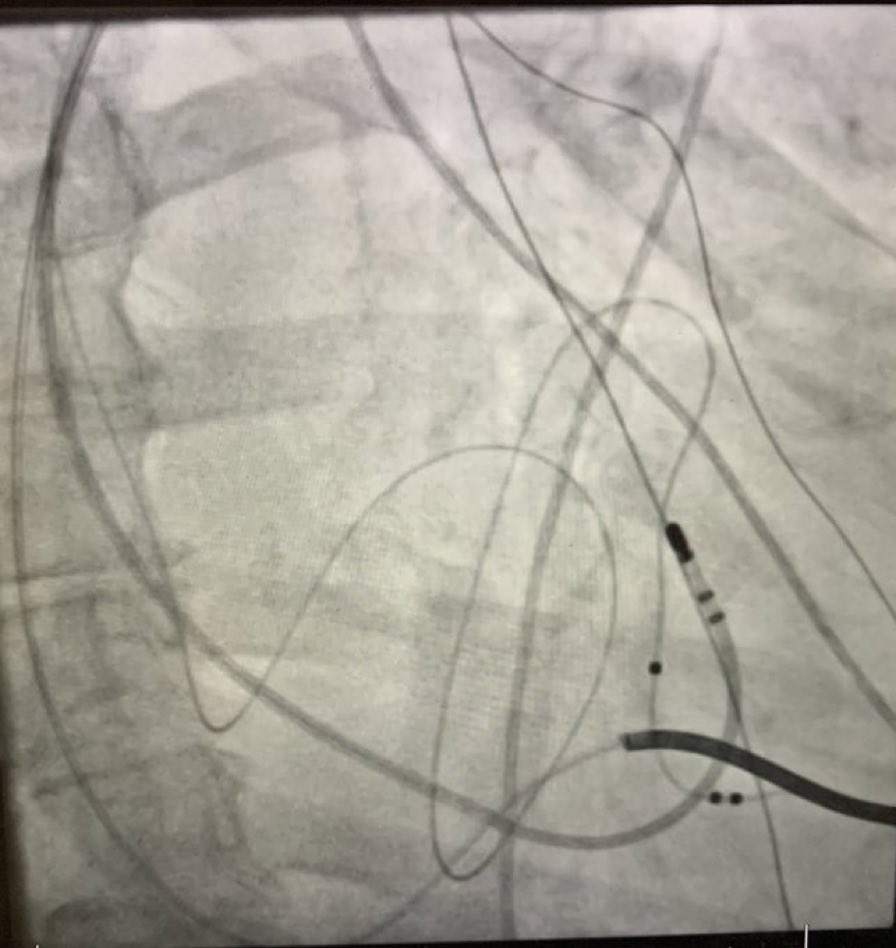
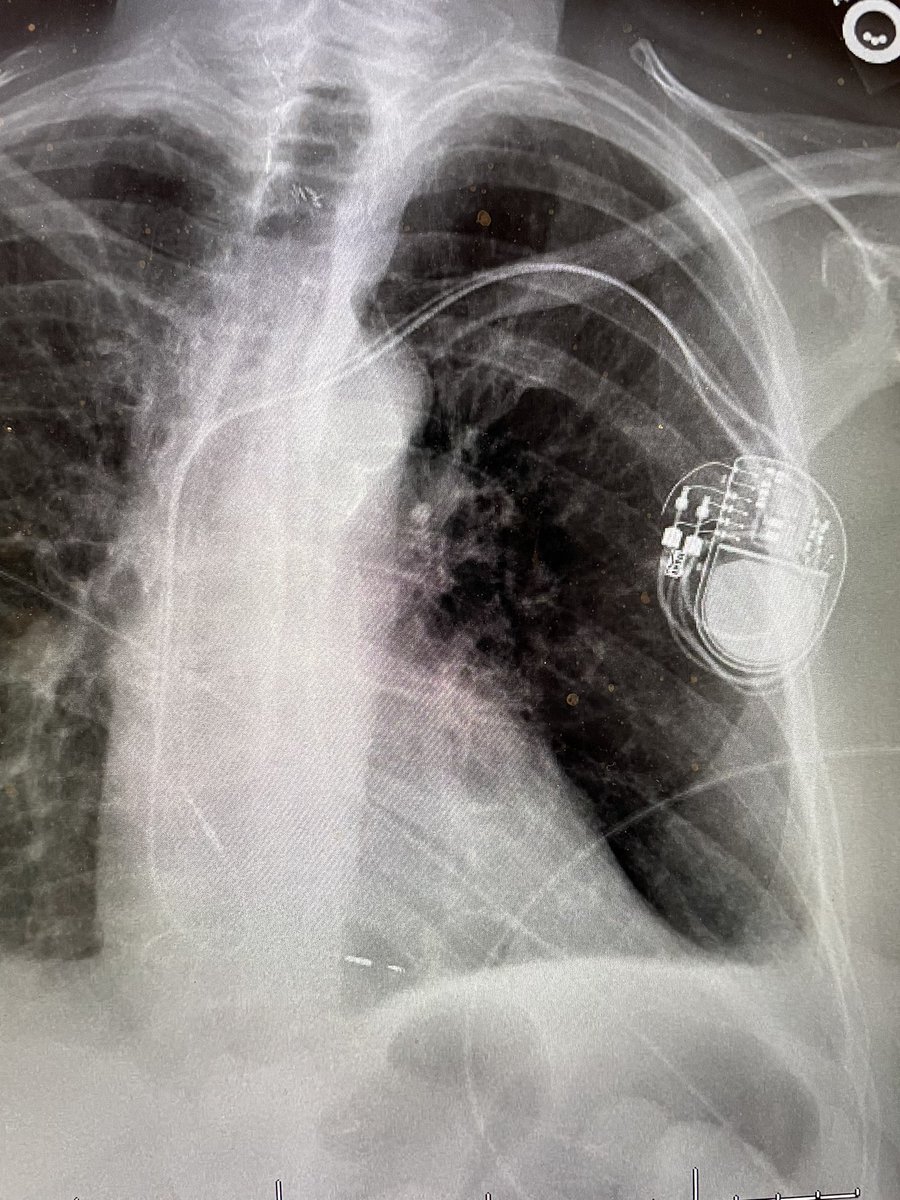
You too can make ablate and pace (CSP) an elegant procedure, approx 1hr procedure time.
Make pocket.
Get access.
Place lead.
Ablate from pocket.
Add atrial lead. (If necessary)
Tie down lead(s).
Irrigate.
Attach device and tie down.
Close pocket.
h/t @SergioPinski
3
1
18
Apr 26
Posterior wall ablation ≠ posterior wall isolation. And it’s easy to map.
We all have pretty post-ablation maps.
New rule: required, if you’re sharing one on X or LinkedIn, show the scale and settings.
Apr 25

🧵Should we use unipolar post wall mapping during AF ablation? Is endocardial silence in AF = posterior wall isolation?
Nice study in @CirculationEP by @Ed_Gerst et al. challenging both assumptions with human endo-epi mapping. Post wall = 3D substrate
ahajournals.org/doi/full/10.…
6
14
4,053
Apr 26
Pradaxa is generic. Industry won't tell you, for obvious reasons.
Dabigatran 150 mg, 60 caps: $23.80 at Cost Plus.
We swap AF patients to warfarin over cost. We push LAAO without knowing it's better.
A $24/mo generic reframes both.
#AFib #Anticoagulation #EPeeps #LAAO
3
7
39
6,966
Apr 19
What does the left atrial appendage really do? What happens when it's gone? Does it matter how it was removed/occluded/closed?
Funday Activity, stick this prompt in your favorite AI and find out.
@drjohnm
gist.github.com/charles-te/3…
1
132
Apr 4
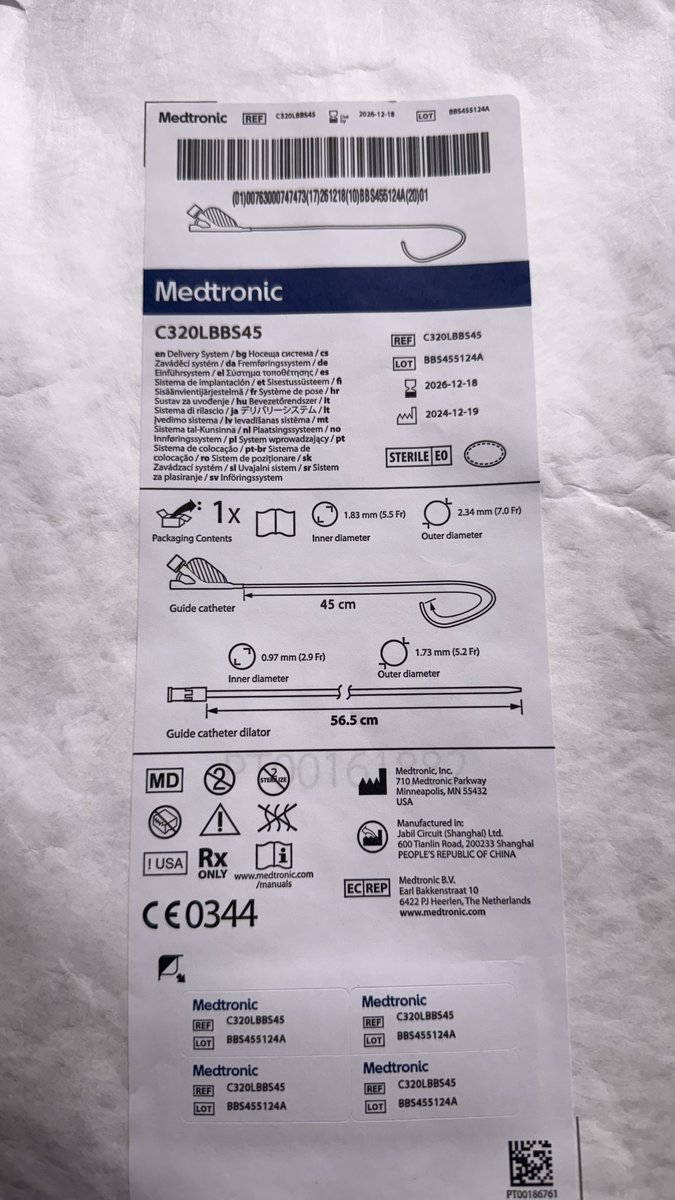
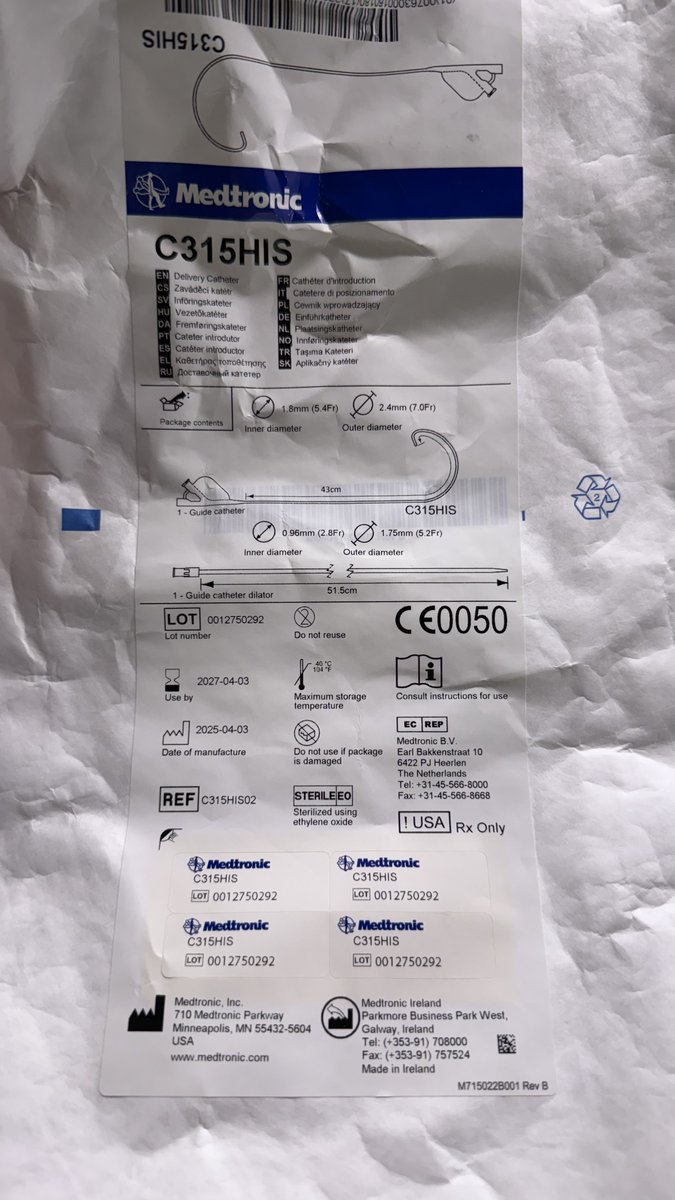
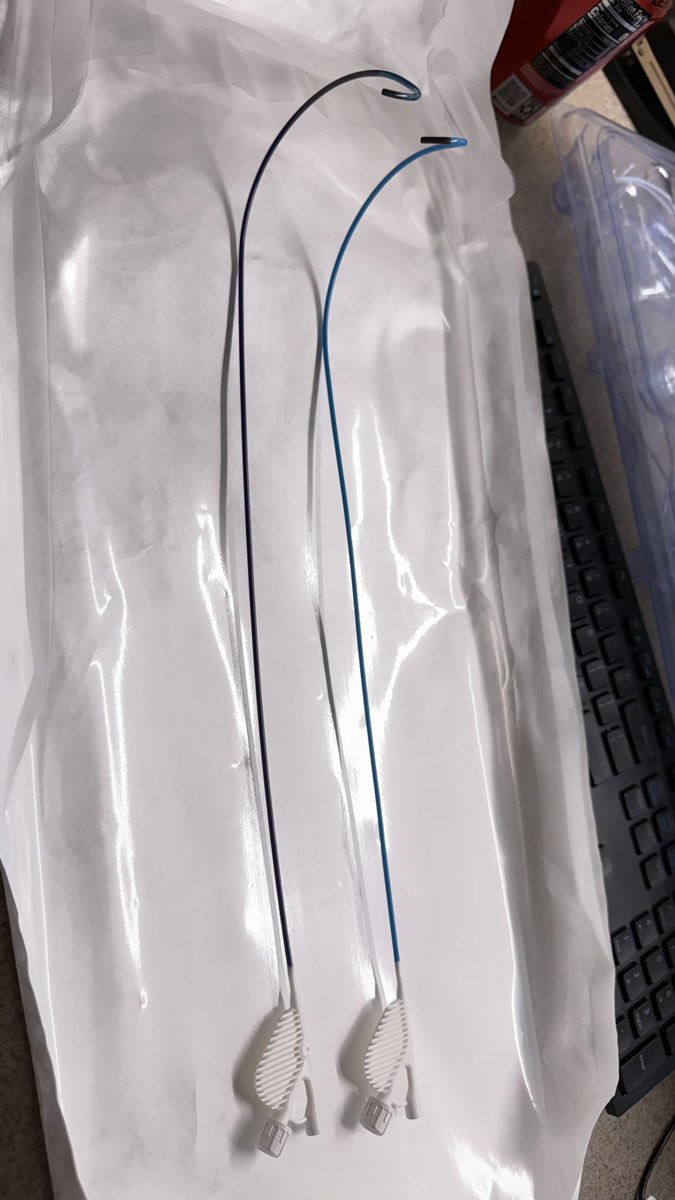
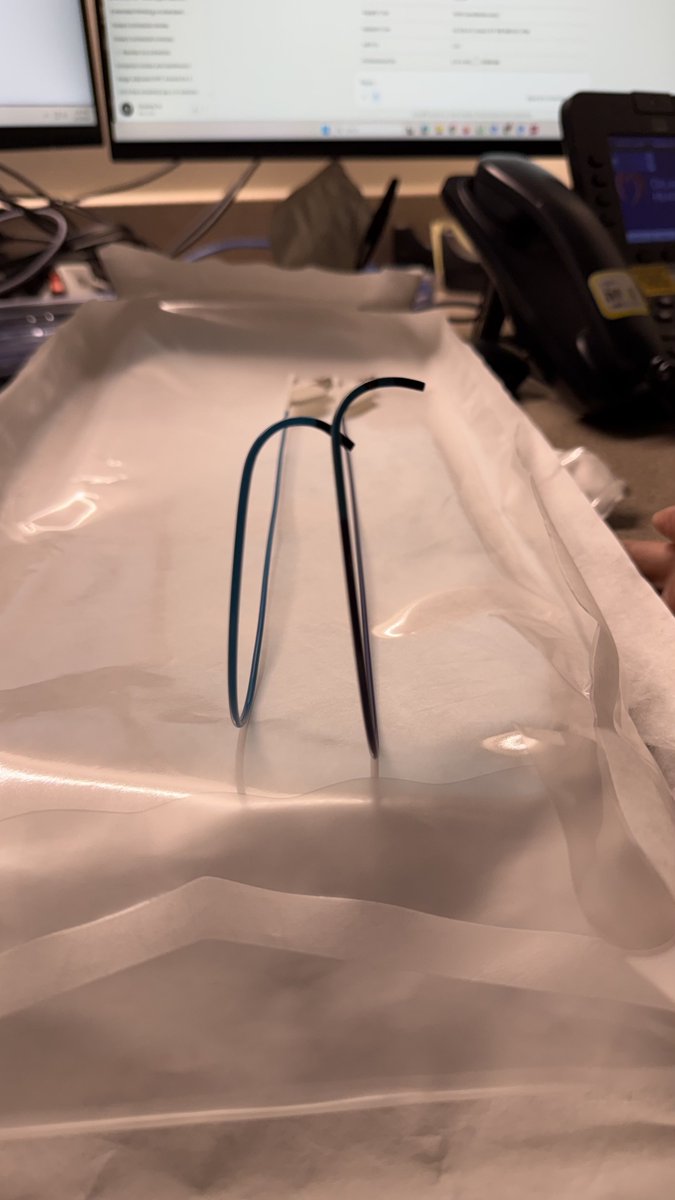
My first look at Medtronic’s new C320LBBS45 for LBBAP. Double-braided, 2 cm longer, redesigned septal curve. #EPeeps #LBBAP #ConductionSystemPacing
4
6
31
4,512
Mar 29
CHAMPION-AF is here. NEJM. 3000 patients. The biggest question in LAAC finally has RCT data.
Noninferiority: met. Bleeding reduction: real. Net clinical benefit: favorable.
Great abstract. But the devil is in the details.
2
1
504
Mar 29
Then there's the stroke signal. 50 strokes in the device arm vs. 33 with NOACs. HR 1.46. It didn't reach statistical significance, but the trial was never powered to detect a stroke difference. Not significant is not the same as not real.
1
128
Mar 29
This isn't anti-LAAC. The procedure works, the bleeding data are real. But if we're going to practice evidence-based medicine, we have to read past the abstract.
claude.ai/public/artifacts/7…
#CHAMPIONAF #LAAC #TrialDesign #Noninferiority #Cardiology #NEJM
1
162
Charles Te retweeted

19 Aug 2025
We’d like to introduce the new 👉 editorial series with narrated videos and illustrated images:
Fundamental Anatomy and Its Impact on Clinical Practice in ‘Da Vinci’ Anatomy Corner @JACCJournals #JACCCaseReports
The first subject: Myocardial Bridging
eur02.safelinks.protection.o…
1
20
46
4,869
Charles Te retweeted

26 Jun 2025
Transventricular VT Ablation Guided by LBBAP Lead in a Patient With Mechanical Double Valve Replacement
Thank you very much for your inspiration
@drtopaloglu @ACH_epteam @ozcanozeke @ElifhandeMD @drfiratozcan
14
22
114
29,030
Charles Te retweeted

27 Apr 2025
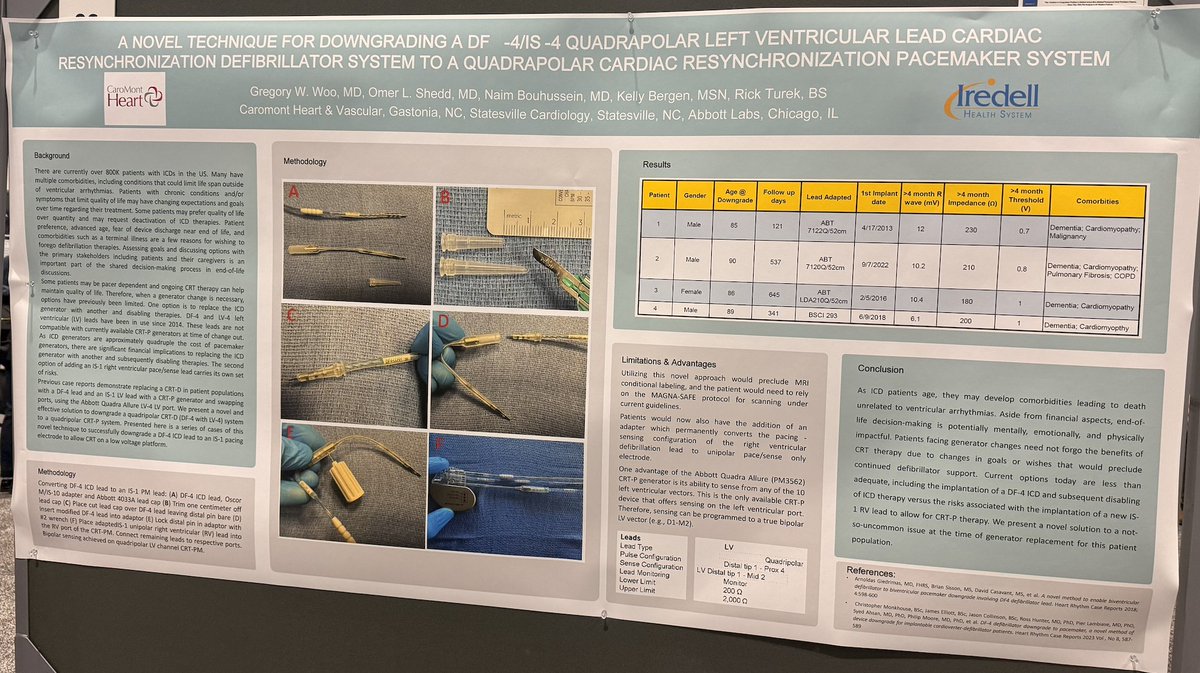
Love the poster sessions at #HRS2025
Highlight was this MacGyver solution to DF-4 ICD lead downgrade to CRT-P problem. Since industry won't give us adapters, we have to get creative.
5mm Uni to IS-1 adapter with cut lead cap as insulator turns DF-4 ICD lead into unipolar pacing lead.
-- Woo et al, including my friend and NP superstar Kelly Bergen.
#HRS2025
4
20
70
9,390
Charles Te retweeted

30 Mar 2025
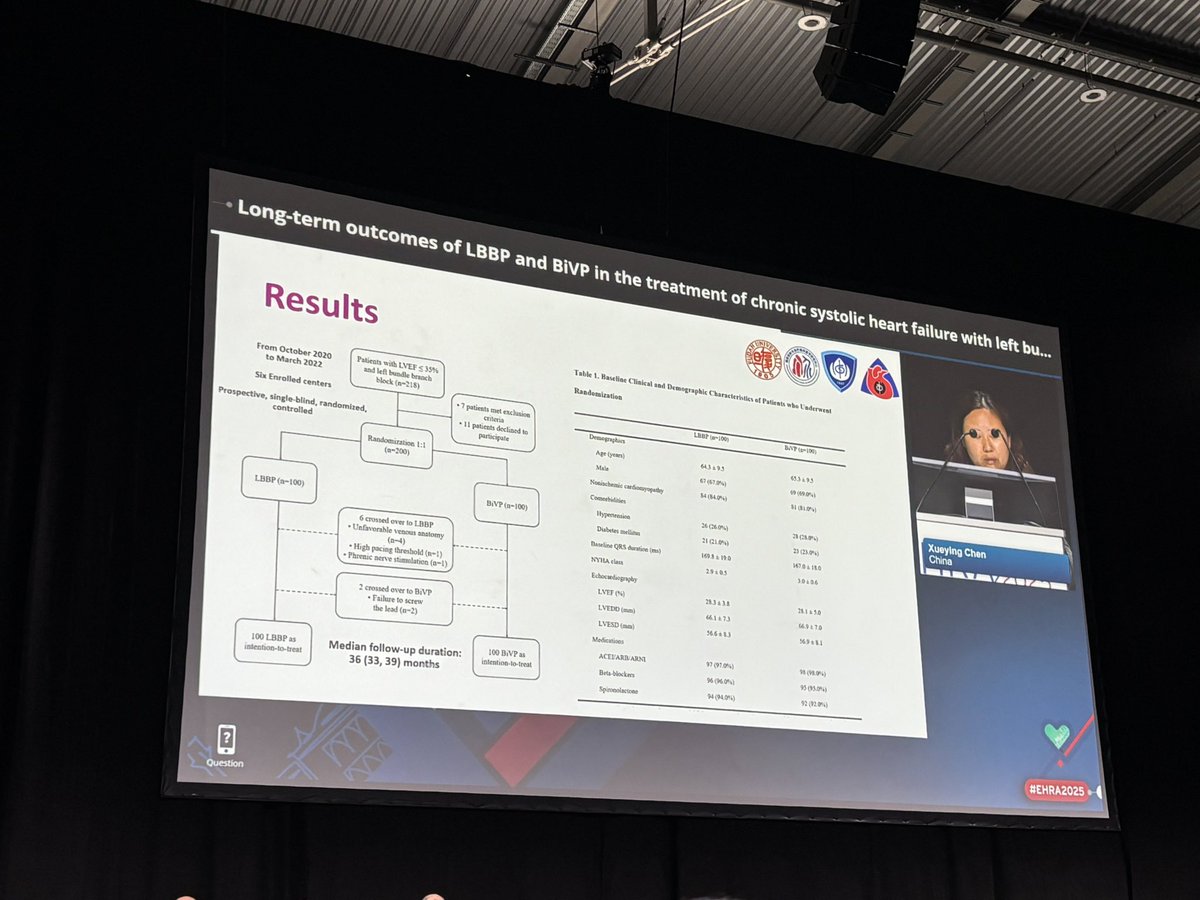
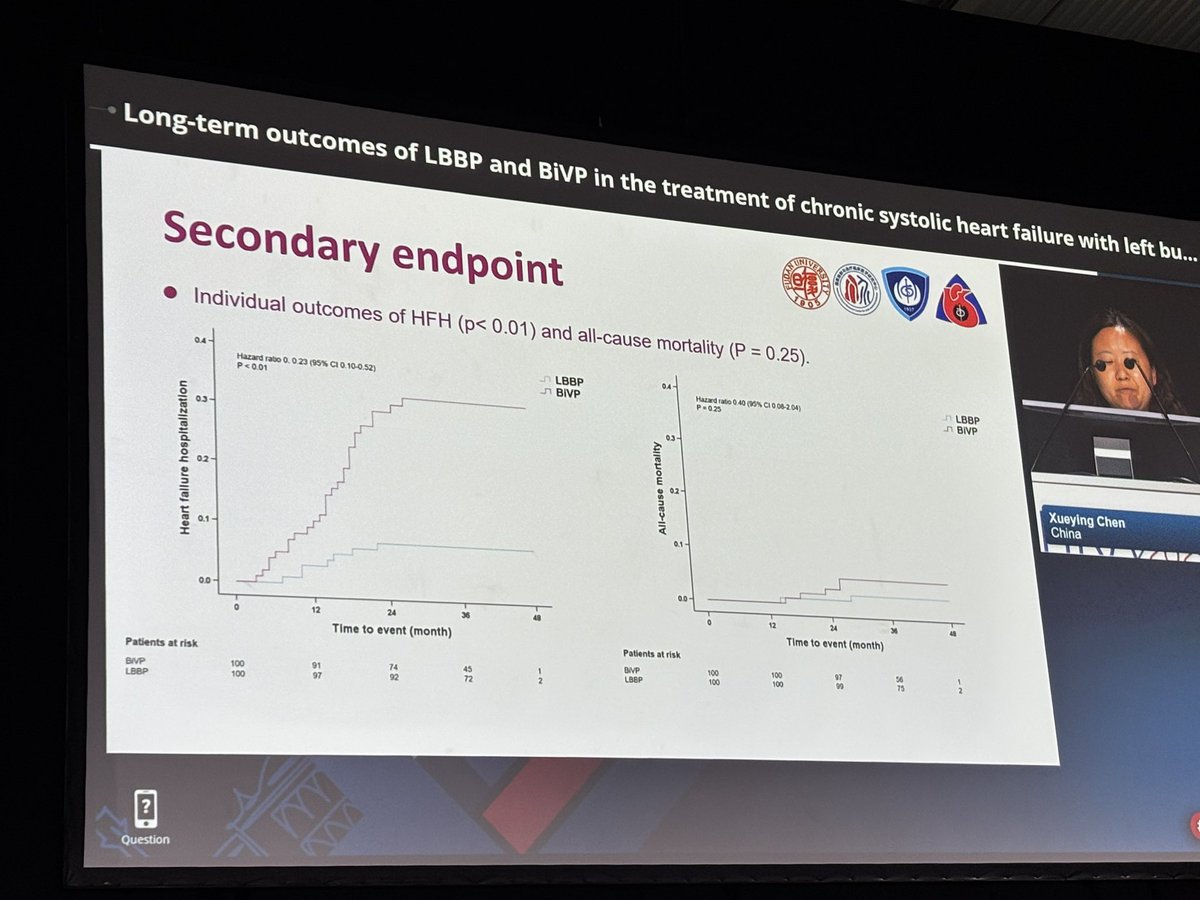
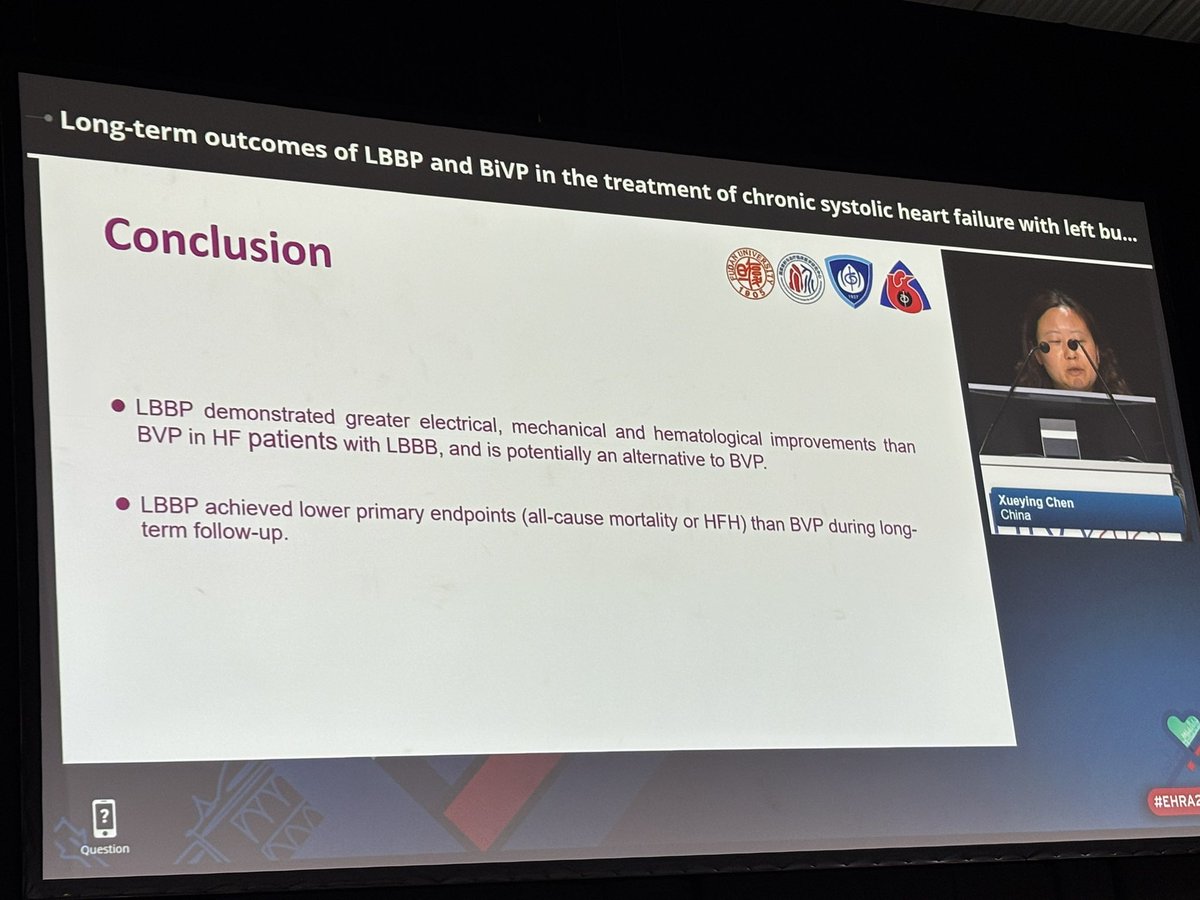
🔥 LBCT #EHRA2025
Heart Sync-LBBP
CRT vs LBBP in systolic #HF: prospective, RCT
200 pts, 1:1
⭐️LBBP bests BiVp for:
♥️ narrower QRS duration
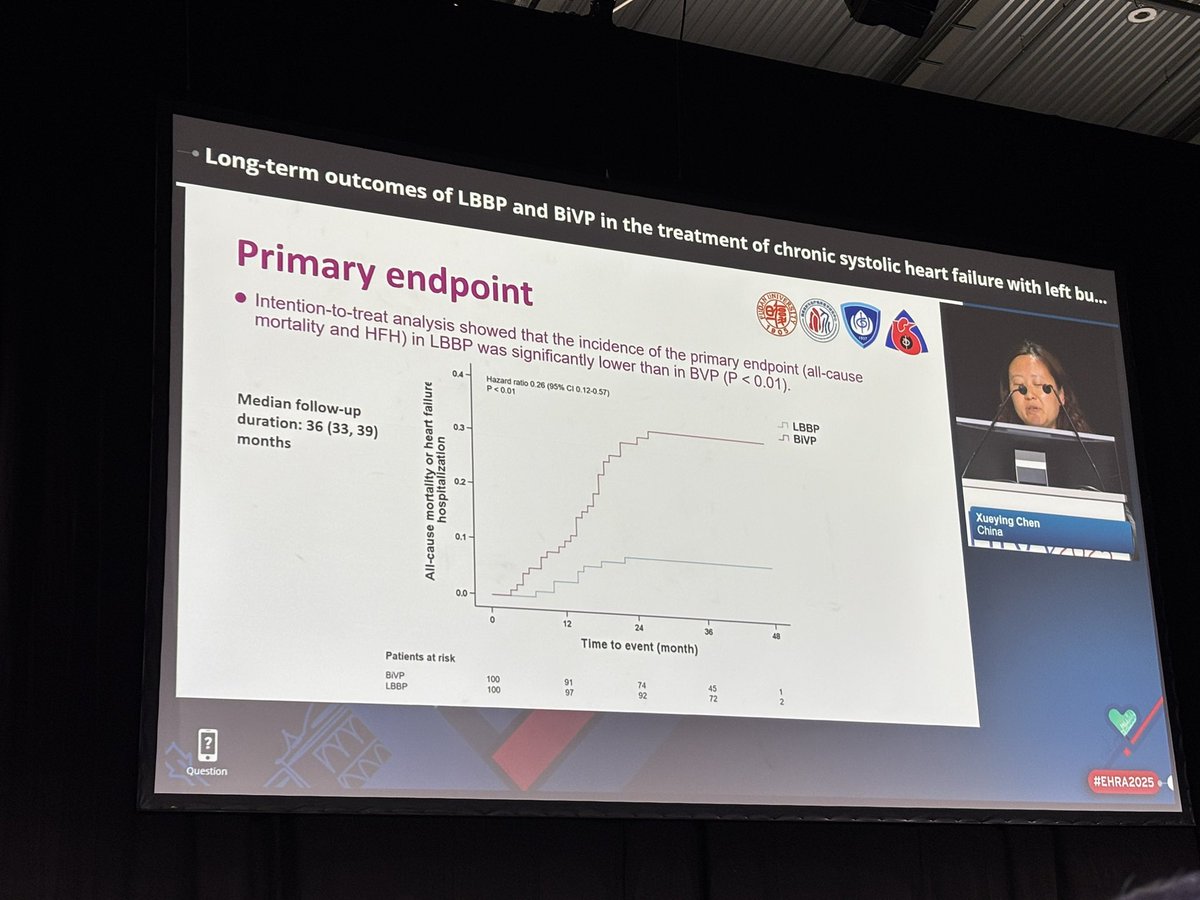
♥️ primary endpoint of combined #HF death as well as 2ndry individual endpoints
(mostly male, nonischemic, ⬇️ mortality)
10
33
90
9,698
Charles Te retweeted

1 Apr 2025
* BREAKING* ABIM loses copyright infringement case against Dr. Jaime Salas-Rushford AND loses effort to seal opinion. Depositions, tactics, ABIM attorney insults, secret agreements: entire docket. All public now. medtees.com/content/SEALED%2… medtees.com/content/DNJ Se…
18
47
223
43,437
Charles Te retweeted

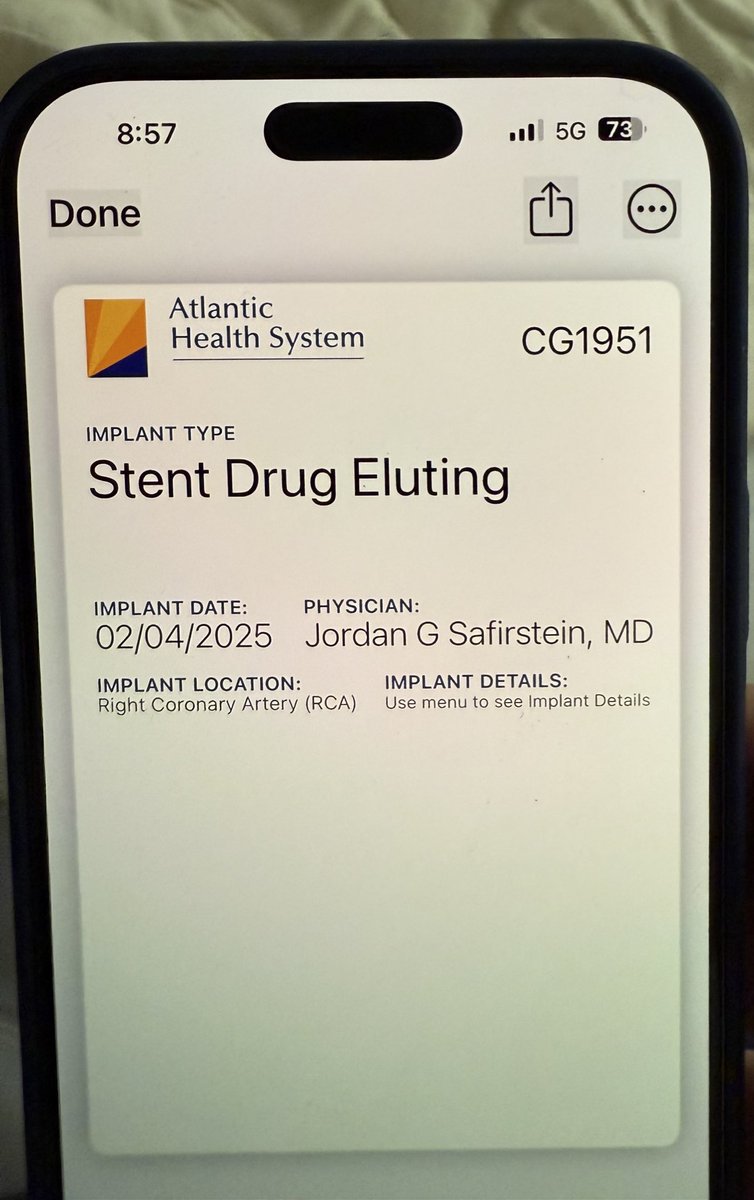
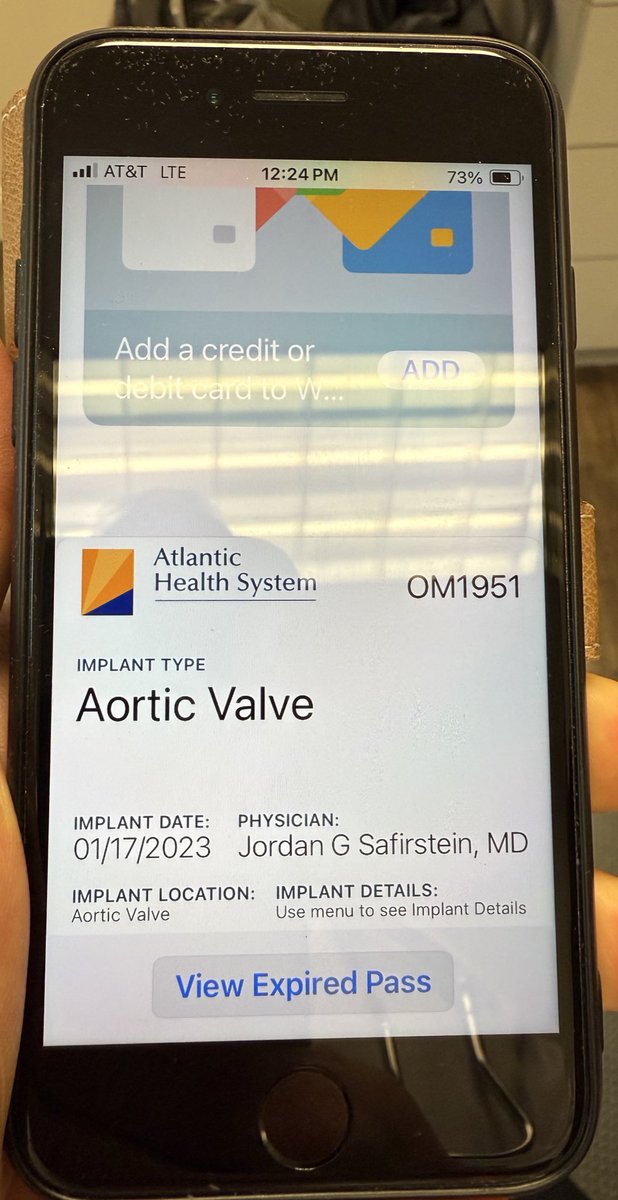
6 Feb 2025
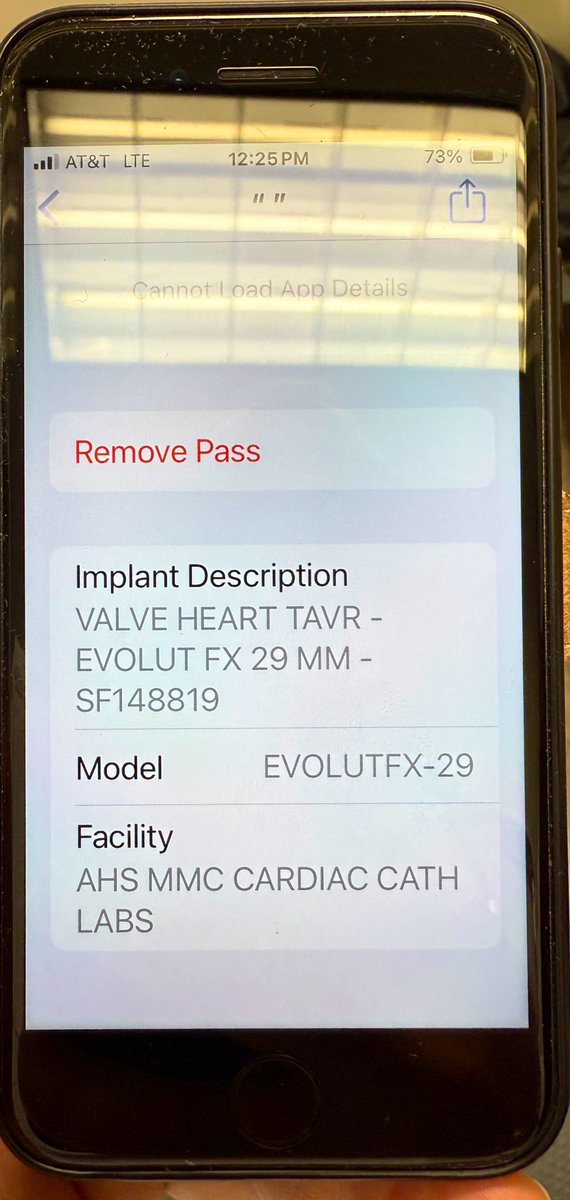
Imagine if your patients had their implant cards sent to their #iPhone immed’ly after their #RadialFirst coronary stent or #TAVR? Implants stored forever with legible, durable, transferable data that may prove essential. Stent size/length & serial number on back!
14
30
216
38,150
Charles Te retweeted

17 Nov 2024
The long-term incidence of stroke in AF is low, especially after ablation of paroxysmals. Stroke scores are from another era and were not developed or validated in this population: CHADSVASC was derived from 20-year old data with ONE YEAR of follow-up.
The treatment effect of statins, BP control, and reduced risk of HF may be contributing more to fewer strokes in AF. Recent AF screening trials have all shown stroke event rates lower than historical. We need a clever and cautious way to redefine risk stroke in contemporary AF patients before assuming that the historical reduction is all from therapy. #AHA24
17 Nov 2024

This is another huge takeaway from the OPTION trial: how low the incidence of stroke is post modern AF ablation.
The CHADSVA tool is meaningless in this cohort, where AF burden has been substantially reduced with ablation
6
17
96
18,240

Charles Te retweeted

10 May 2024
Elias Sports Bureau reports tonight is the first Red Panda 5-bowl, MidFirst halfcourt shot combo
3
6
152
18,392
Charles Te retweeted

29 Apr 2024
Iconic Figures: The first catheter ablation
Free to all!
heartrhythmjournal.com/artic…
1
49
116
17,928