
Core EM is the official blog and podcast of the NYU/Bellevue EM Residency. #FOAMed @NYULangoneEM
Joined January 2015
- Tweets 2,061
- Following 309
- Followers 15,873
- Likes 1,860
857 Photos and videos


🚨 Post-ROSC Pearl:
Code-dose epi (1mg IV) wears off in ~3 minutes.
That’s your rearrest window.
Have push-dose pressors at the bedside BEFORE the crash comes.
Don’t wait for the monitor to tell you what you already know.
Have a listen for more pearls:
coreem.net/podcast/episode-2…
1
18
78
5,504
💉 Naloxone Tips:
Titrate to respiratory effort, NOT full consciousness.
Start low 👇 (0.04-0.1 mg IV) and repeat.
Slamming a full 2mg can trigger acute withdrawal, vomiting, aspiration, pulmonary edema, and a combative patient.
Less is more. Titrate up 👆.
Full article (oldie but goodie): coreem.net/core/naloxone-mas…
15
47
3,142
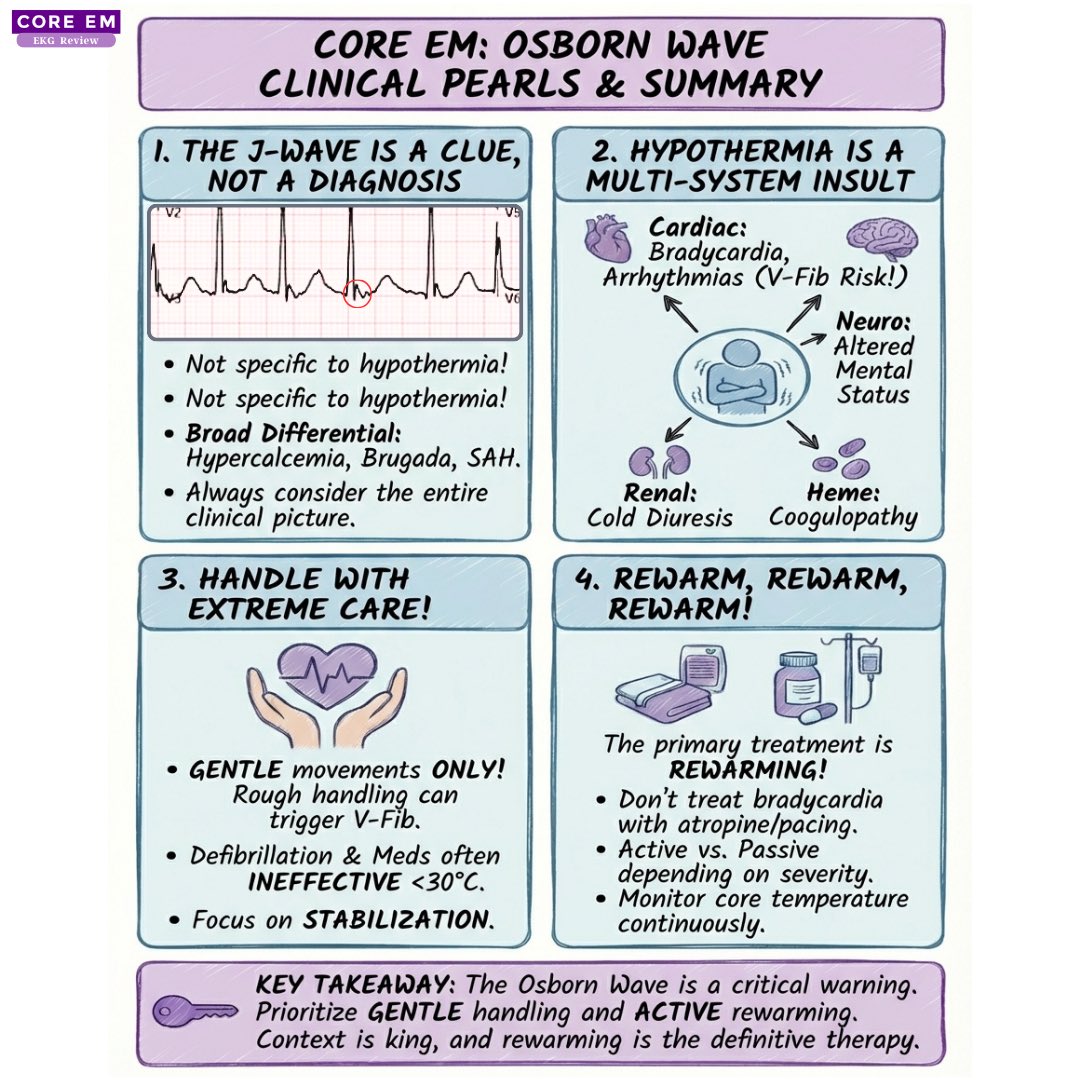
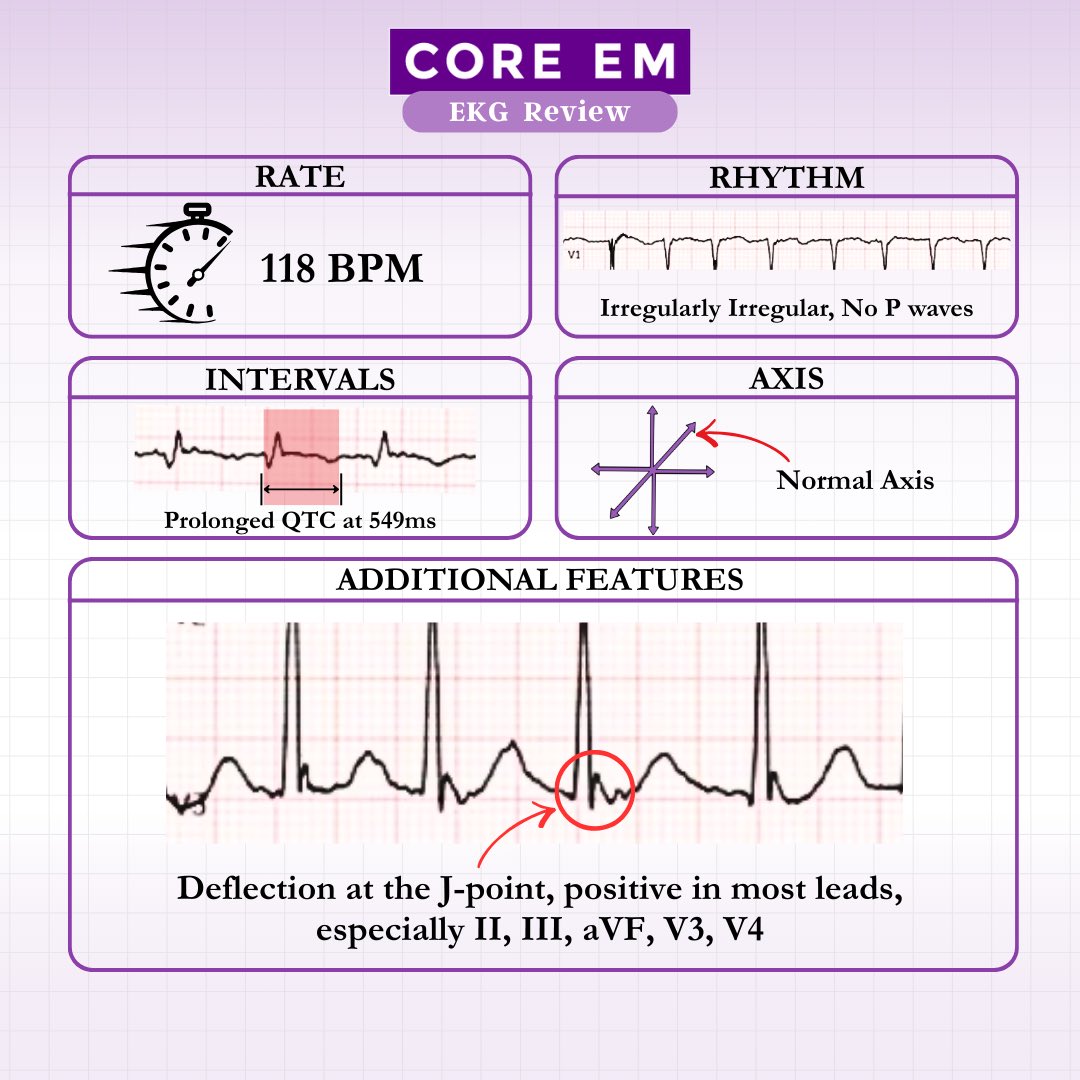
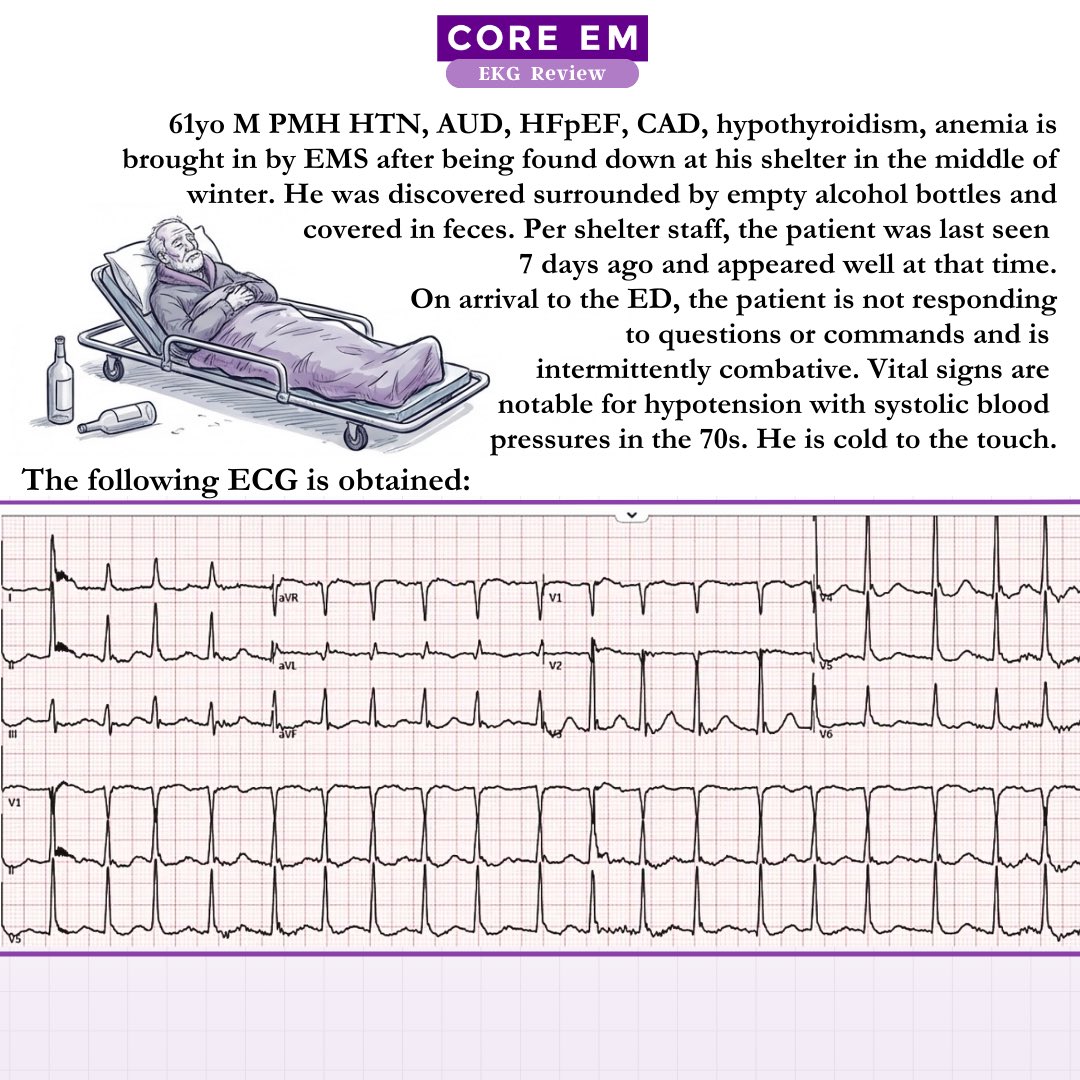
head over to our site for the complete review, and stay warm out there ❄️☃️
coreem.net/ekgs/a-cold-heart…
227
Low-risk PE mortality: <1%
Intermediate-risk mortality: 3-15%
High-risk (massive) PE mortality: 25-65%
If SBP <90 for >15 min or requiring pressors → activate your PERT team immediately 🚨
Don't miss our full breakdown ⬇️ coreem.net/podcast/episode-2…
16
66
3,885
Our mission has always been to bring you high-yield, evidence-based content that you can use immediately on your next shift. We know your time is valuable, which is why we’re proud to officially launch the Core EM Modular CME Course.
coreem.net/blog/medical-educ…
2
532
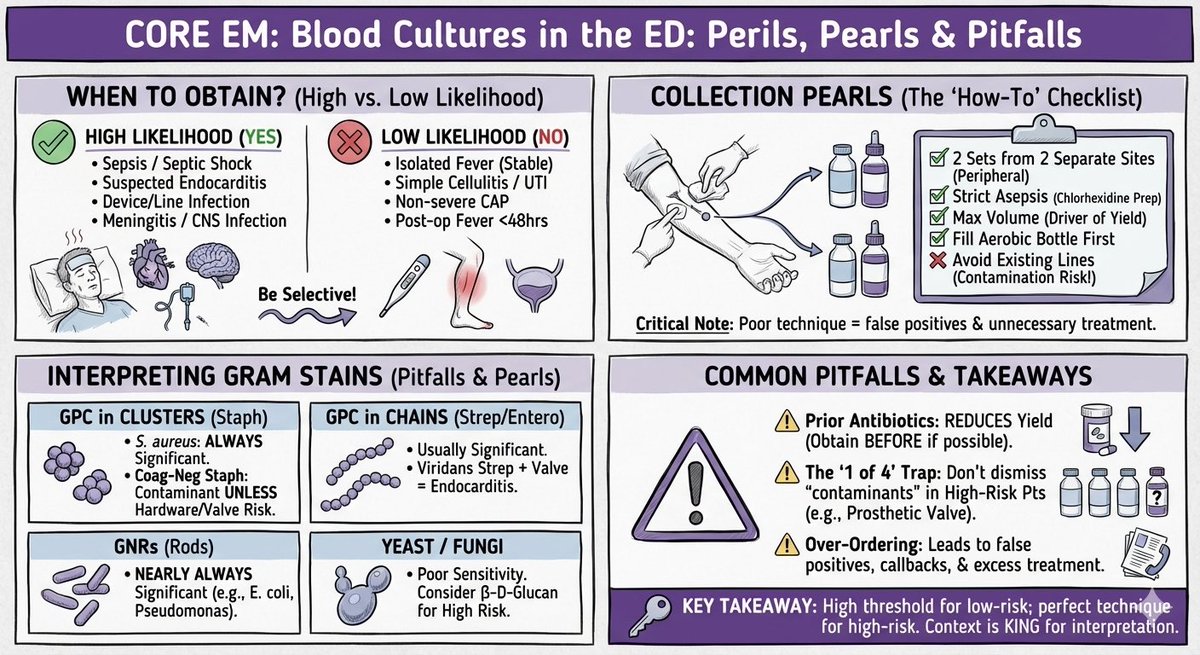
Read our full blog post on the topic 🩸
coreem.net/core/blood-cultur…
1
1
304
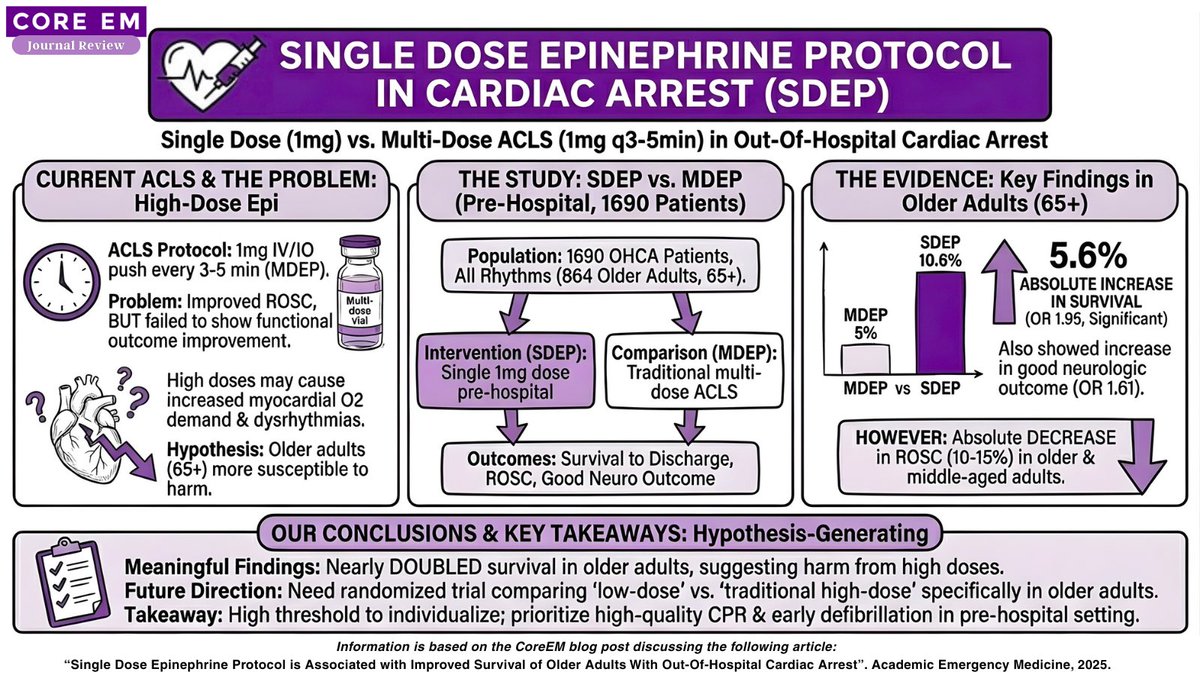
Head over to our site for the full review!
coreem.net/journal-reviews/s…
361
Not only should you know what a QuickTrach is, you should definitely know how to use it..
Don’t worry, just sit back, relax, and we’ll teach you in three minutes..
youtu.be/K4BfdTlmzX8?si=0mgq…
4
838
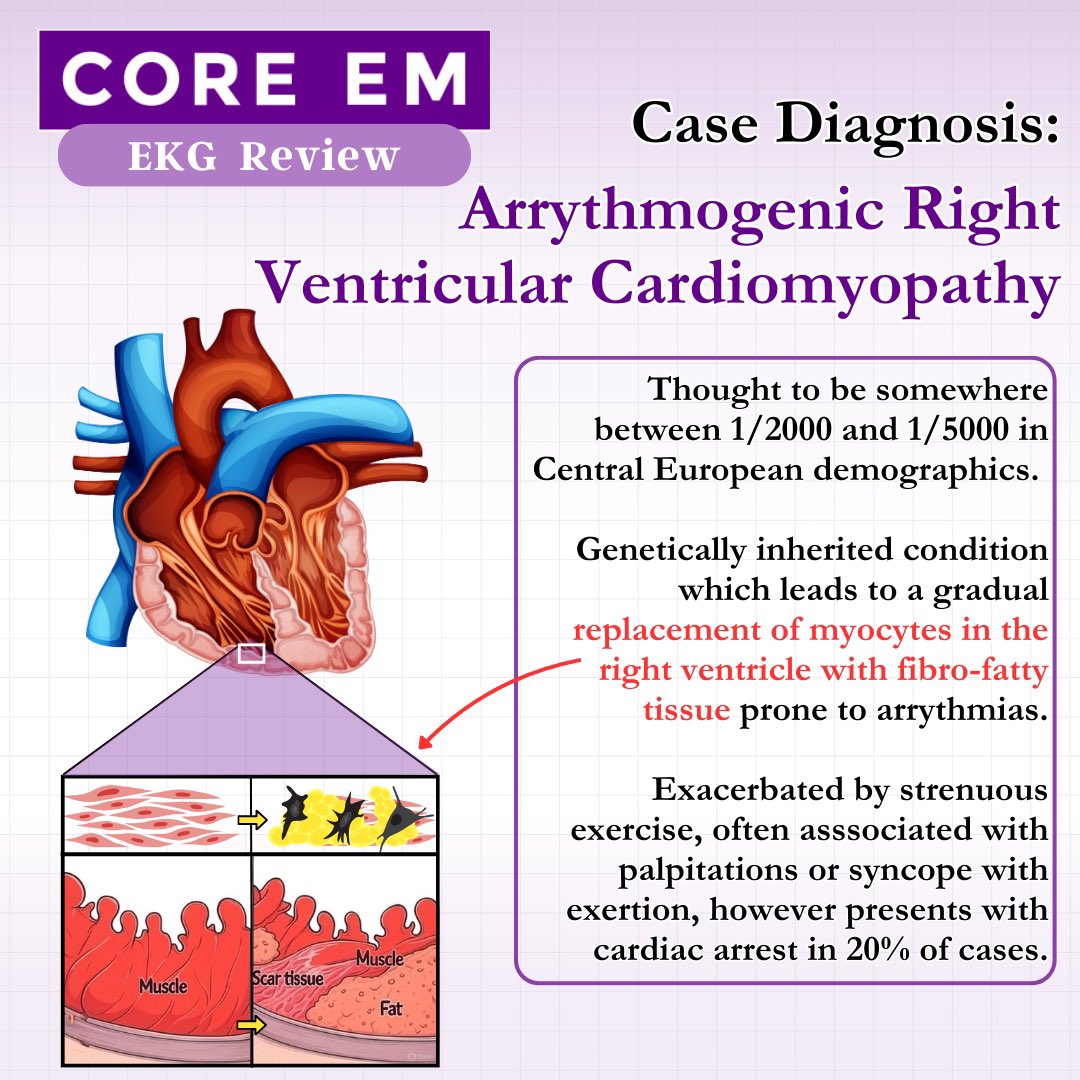
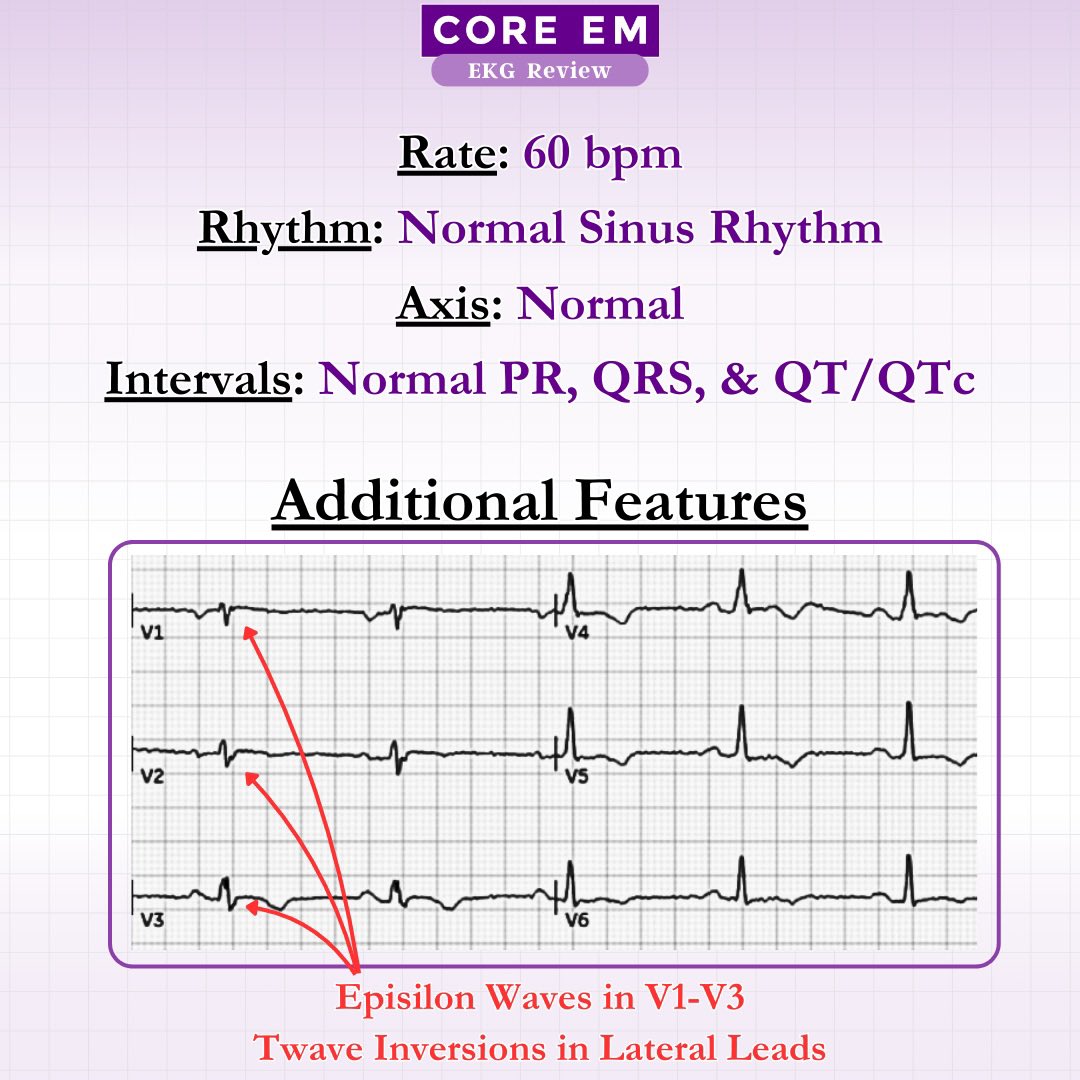
Head over to our site for a deeper dive into the diagnostic criteria and management of this cardiomyopathy ❤️🩹
coreem.net/ekgs/something-is…
548
Give us a follow on Bluesky for more educational content!
bsky.app/profile/coreem.bsky…
1
1
763
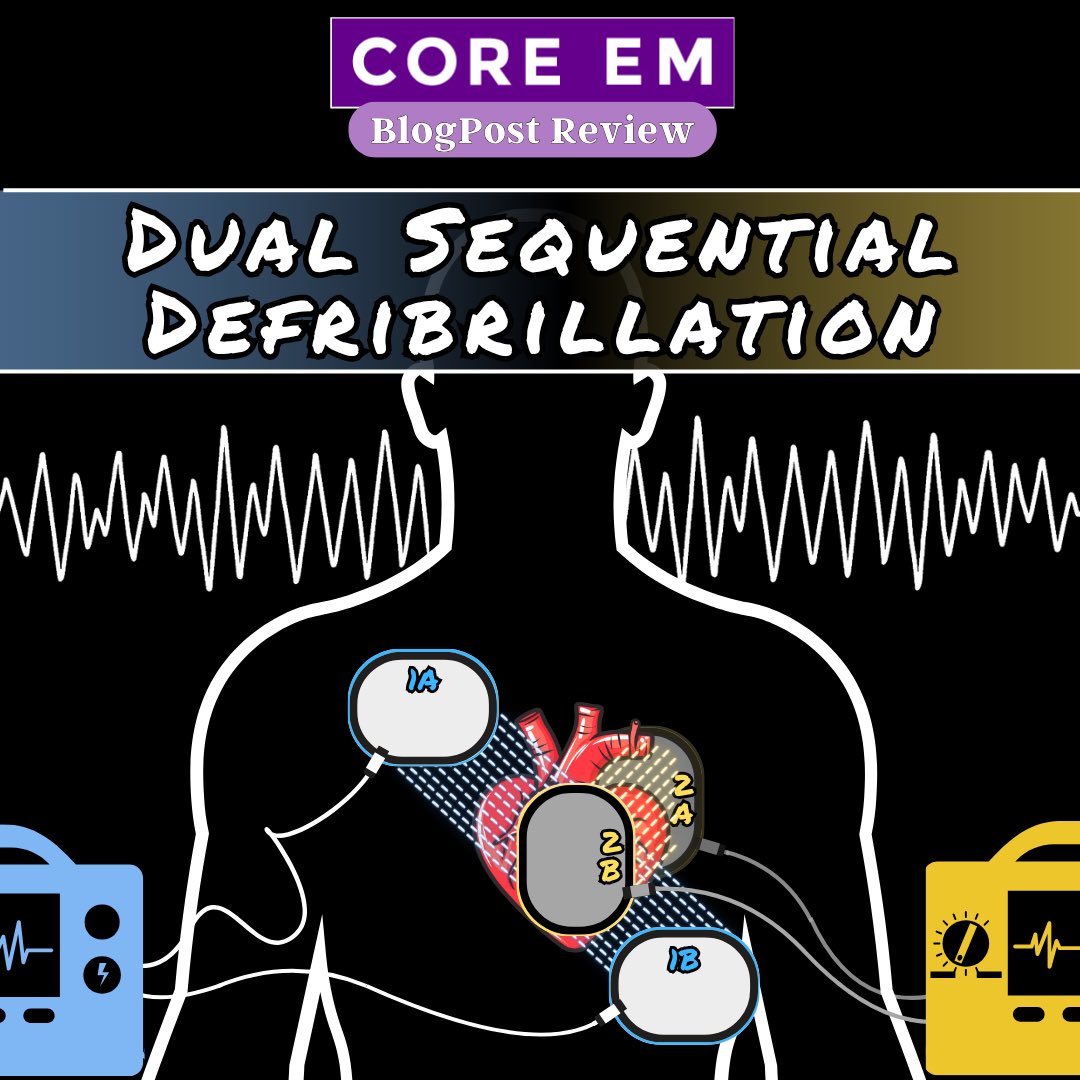
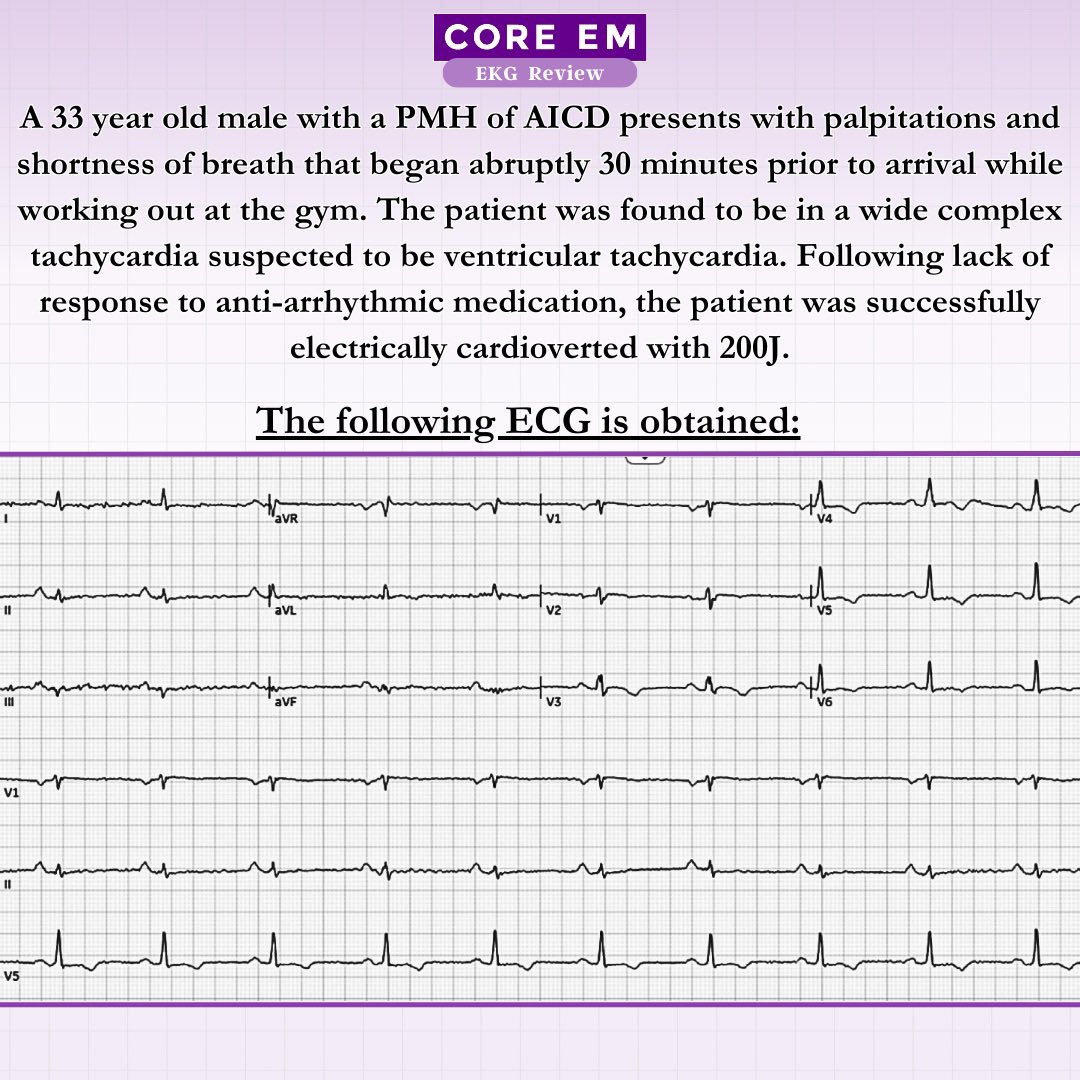
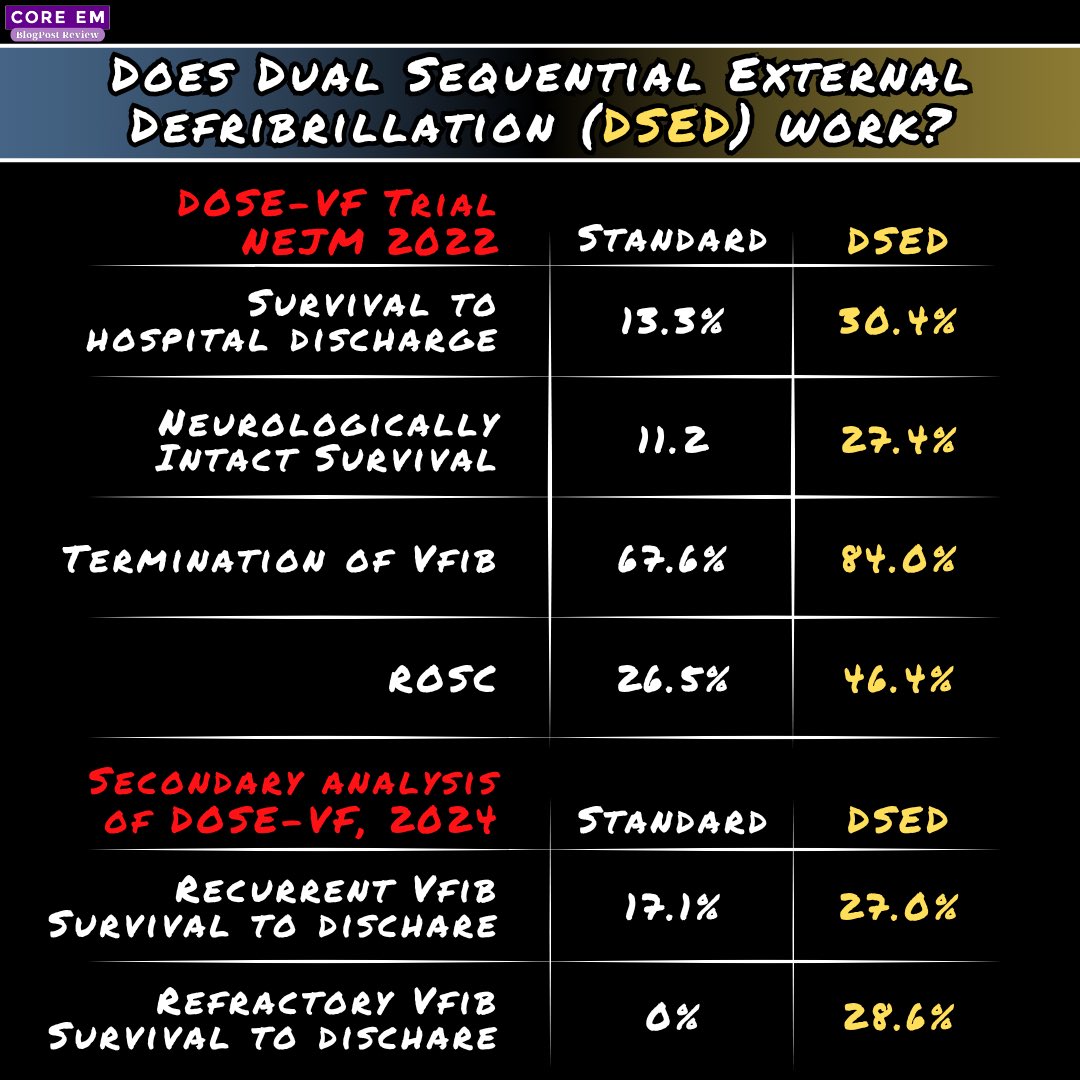
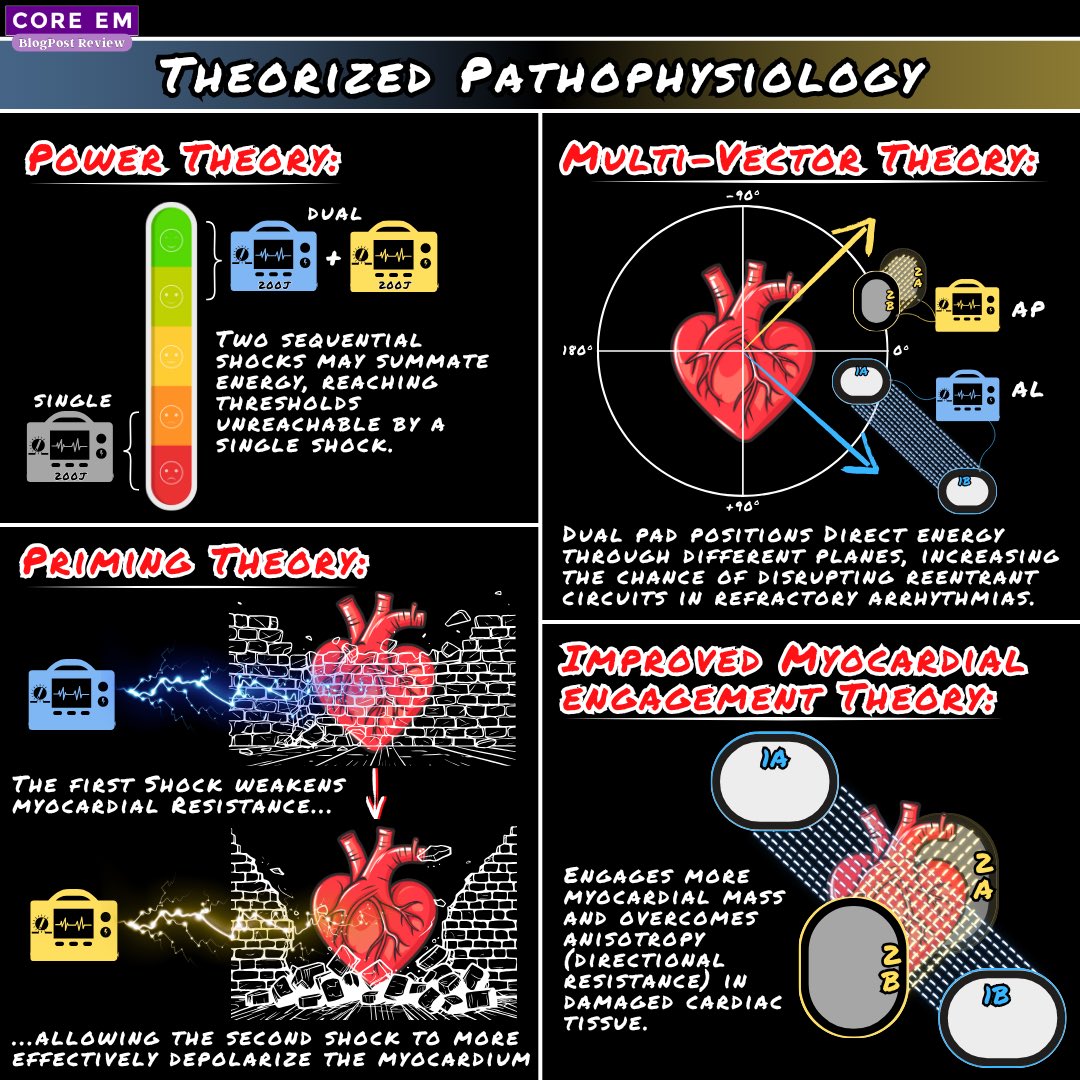
Head over to our site for the complete discussion and further reading, let us know if you’ve tried it!
coreem.net/core/dual-sequent…
2
1
629
And if you want a refresher on managing refractory ventricular arrhythmias, take a look through our podcast review on Electrical Storm or listen to the whole podcast episode for a deep dive

Have you listened to our podcast on VTach Storm? This is a phenomenon you want as much knowledge of as possible PRIOR to having to treat it.
Here’s a brief summary ⬇️🧵1/5 #MedEd
1
952