
McMaster Critical Care Update. An annual half-day, in-person CPD conference with a networking dinner.
Joined November 2018
- Tweets 62
- Following 125
- Followers 163
- Likes 2
27 Photos and videos






Only 10 days left to register for the 5th Annual McMaster Critical Care Update on Wed, Dec 11/24 @LIUNAStation. 🌟 Expand your critical care knowledge & network at this in-person CPD event. Register today 🔗 cpd.healthsci.mcmaster.ca/cr… #MacCPD #CritCareCPD
35

26 Nov 2024
Don’t miss the 5th Annual McMaster Critical Care Update on Wed, Dec 11/24 @LIUNAStation! 🌟 Learn, connect & grow your critical care network at this in-person CPD event. Register now 🔗 cpd.healthsci.mcmaster.ca/cr… #MacCPD #CritCareCPD
24
22 Nov 2024
#CritcareCPD will be recorded, & the recordings will be accessible to all registrants for 6 months. Only registrants who attend will be eligible to receive a certificate of attendance for CME credits.
View the brochure register today!
🔗 cpd.healthsci.mcmaster.ca/cr…
#MacCPD
26
21 Nov 2024
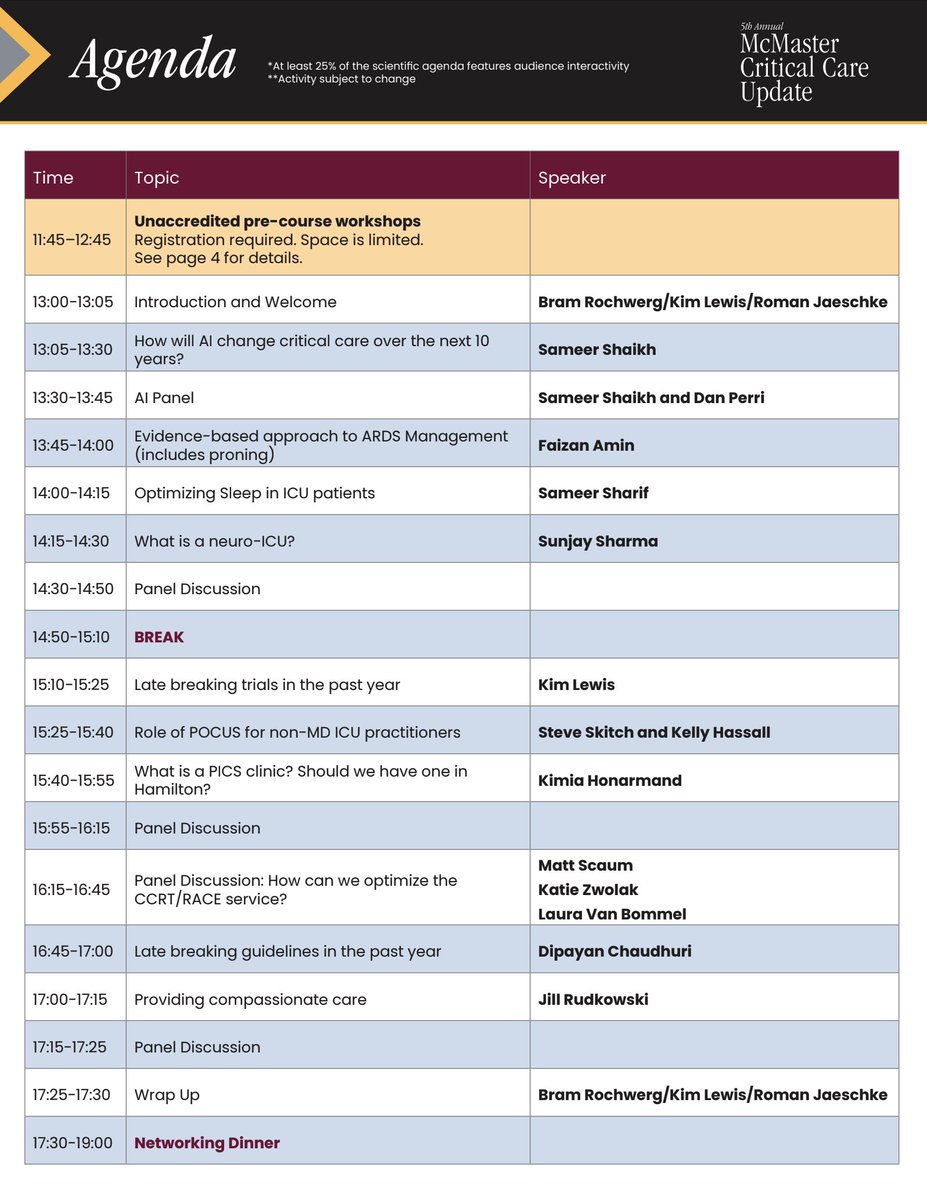
View the agenda & expert speakers for the McMaster Critical Care Update on Wed, Dec 11/24 @LIUNAStation! View the brochure register 🔗 cpd.healthsci.mcmaster.ca/cr…
#MacCPD #CritCareCPD
ALT Critical Care agenda
28
20 Nov 2024
Register now for the 5th Annual McMaster Critical Care Update and join us on Wed, Dec. 11/24 @LIUNAStation.
This in-person CPD is an opportunity to learn, connect, & expand your critical care network.
Register 🔗 cpd.healthsci.mcmaster.ca/cr…
#MacCPD #CritCareCPD
ALT 5th Annual McMaster Critical Care Update brochure cover
2
3
293
28 Apr 2022
Thank you everyone who attended the McMaster Critical Care Update Day, for those who have followed along here, and of course to our amazing speakers!
We hope to see everyone again in Hamilton next year! Stay well~
@mcmasterchse // #critcareupdate2022
2
7
27 Apr 2022
Dr. Suzanne Turner's pearls from "Managing chronic opioid dependency in the ICU"
1. Fentanyl analogues do not come up on urine drug screens
2. Patients who use high doses of fentanyl, especially injection, go into withdrawal VERY quickly (within a couple hours)
1
2
7
27 Apr 2022
3. Consider adjuncts in PWUD (persons who use drugs)
- Nicotine replacement therapy
- THC replacement (nabilone) anecdotally may be helpful
- Keep Narcan at bedside (2/3rd of pts willing to accept a Narcan kit offered in ER)
- Make patients aware of Needle & Syringe programs
1
1
27 Apr 2022
4. Goals:
A. Maintain opioid tolerance in hospitalized patients to minimize post-discharge accidental overdoses
B. Avoid unexpected discharges
C. Initiate opioid agonist therapies (OATs)
If Addictions Specialist services are available at your hospital, consider a consult!
1
27 Apr 2022
Dr. Belley-Côté's (@ebelleycote) pearls from "When should we be starting inotropes?"
1. Two situations to consider: Cardiogenic shock (pump failure) and mixed shock ('relative' pump failure). Necessary in the "cold & wet" patient
1
9
24
27 Apr 2022
2. Two common options (in Canada): Dobutamine & milrinone. Dobutamine is "on-fast, off-fast," but is arrhythmogenic. Milrinone causes fewer arrhythmias, but has a slower onset and can drop BP (especially as a bolus, so keep a vasopressor [i.e. NorE] handy)
1
1
5
27 Apr 2022
3. Check out the DOREMI study (Mathew et al., 2021, NEJM; nejm.org/doi/full/10.1056/NE…): Among patients with cardiogenic shock, there were no significant differences in cardiovascular or renal outcomes between milrinone and dobutamine.
1
7
27 Apr 2022
Dr. Roman Jaeschke's (@jaeschke3) pearls from "Surviving Sepsis 2021 Update":
2021 Sepsis guidelines available here: journals.lww.com/ccmjournal/…. Table 1 provides an at-a-glance summary of recommendations
1
4
27 Apr 2022
Selected key updates:
- Capillary refill time may be used as adjunct to guide resuscitation [ANDROMEDA-SHOCK; Hernández et al., 2019, JAMA]
- Balanced crystalloids as initial fluids; although debate remains in literature on true impact on balanced crystalloid vs. normal saline
1
1
27 Apr 2022
Misc extracts; weak recommendations: Steroids in refractory shock, stress-ulcer prophylaxis in at-risk patients, initiation of enteric nutrition by 72h
27 Apr 2022
Dr. Simon Oczkowski's (@Simon_Ocz) pearls from "Triage in the ICU"
1. Triage preparation ( target) requires: Broad community awareness (pts families), creation of a "triage team" & necessary training (clinicians), and have a central oversight / monitoring committee (hospital)
1
1
4
27 Apr 2022
2. Lack of consensus on best triage criteria: Short-term survival? Long-term survival? Limited number of validated prognostication tools
3. Triaging for a disease with an unknown prognosis?: Changing epidemiology, new treatments, and learning curve
1
27 Apr 2022
4. Multi-specialist approach: Legal, policy, ethics, and clinical experts are necessary to minimize the harms of triage, while protecting patients/families
"Despite preparation, we will never be 'ready' for triage."
27 Apr 2022
Dr. Bram Rochwerg's (@Bram_Rochwerg) pearls from "Evidence-based COVID treatments"
1. Compiling evidence is no easy feat: Continually adding to ""living guidelines"", found in the BMJ (bmj.com/content/370/bmj.m298…; Siemieniuk et al., 2020)
1
1
9
27 Apr 2022
2. Severe COVID: Corticosteroids for hospitalized pts (ward or ICU) [RECOVERY]; EITHER IL-6 inhibitors (Tocilizumab, sarlumab) or JAKi2 inhibitors (baricitinib) when patients deteriorating. Combination of IL-6 and JAK-2 not recommended (?over-immunosuppression).
1
2
27 Apr 2022
3. Antivirals: Best if given within 5 days of symptom onset, and recommended only in those with >10% risk of hospitalization. Paxlovid showing most promise currently
1