
#IoT security simplified. Protecting against #cyberattacks by safeguarding what matters most.
Joined April 2017
- Tweets 974
- Following 287
- Followers 384
- Likes 516
584 Photos and videos














You can't patch everything. So here's how CISOs actually prioritize: Risk
💥 Factor 1: Exploitability
Is this vulnerability actively being exploited in the wild? Or is it theoretical?
Active threat > theoretical vulnerability. This matters more than CVSS score.
💥 Factor 2: Device Criticality Position
A vulnerability on an isolated admin device is different from a vulnerability on an ICU monitor connected to your main network.
Context matters. Severity score doesn't.
💥 Factor 3: Your Ability to Remediate
Can you patch it? Segment it? Replace it? Or are you stuck with it?
Knowing what you can actually do changes your entire response strategy.
Most teams are drowning because they're treating all vulnerabilities equally. The CISOs
winning are the ones who've built a context-based prioritization framework.
The manual version takes weeks to build and constant updating. The smarter version automates this correlation.
How are you currently deciding which vulnerabilities to remediate first?
#healthcarecybersecurity #threatprioritization #IoT
26
Your security team gets on average 17,000 vulnerability alerts per week. They patch. They report. They stay busy.
But here's the truth: 🫣 most of those alerts don't actually matter for your environment.
Not because the vulnerabilities aren't real. But because the device isn't on the clinical network, it's already isolated, or it's not connected to a patient or processing patient data.
➡️ Here's the gap: your tools flag everything. Your team has to manually figure out what actually matters. That’s alert fatigue.
➡️ The SMARTER approach: prioritize by actual risk to patient care, not by severity score.
Which vulnerabilities affect devices impacting patient care? Which are actually exploitable in your network?
Answer those questions, and you stop guessing.
How would your response change if you could prioritize that way?
#healthcarecybersecurity #alertfatigue #IoT
18
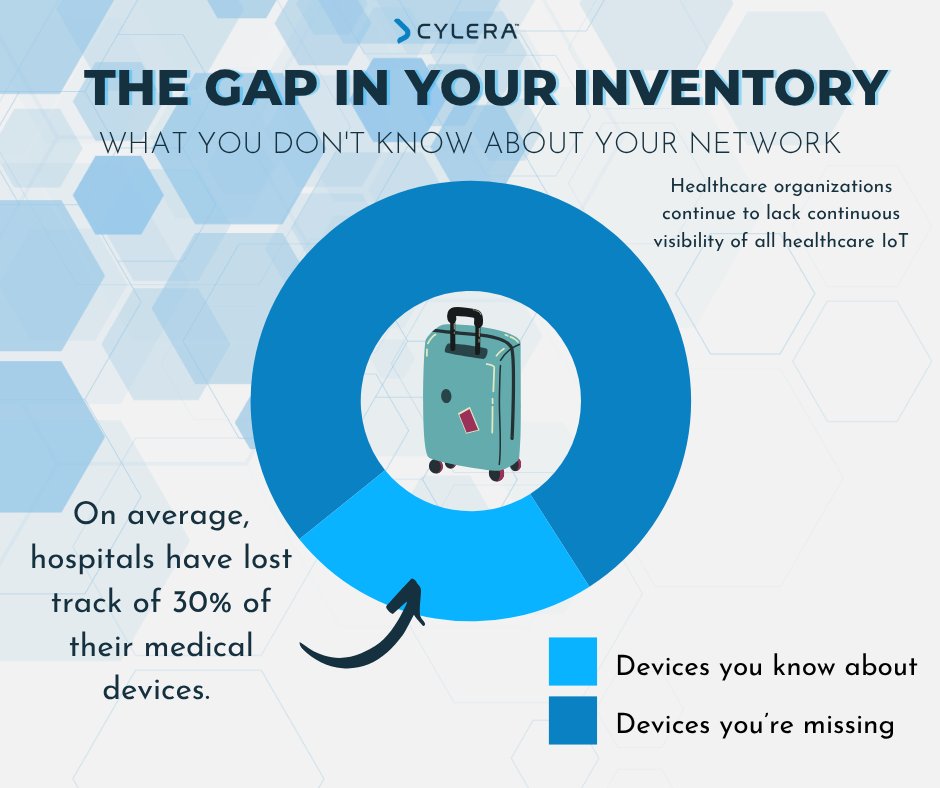
Most hospitals can't see all their connected devices.
A large health network across 300 sites discovered this the hard way. They had thousands of devices on the network but couldn't see them all. 🏥
They struggled to figure out: which networks are each device on and which devices that affect patient care are the most at risk?
That gap meant security exposure they couldn't tolerate. 🚨
So they changed their approach. They got complete visibility into every device, down to the OS, firmware, device behavior, and even usage.
✨ They knew where each one was and was able to see changes, anomalies, and security breaches in real time.
Here's what that enabled:
Security team could efficiently prioritize risks and vulnerabilities that actually affected patient care. Risk exposure dropped and operations became more resilient.
One of their leaders told us: "Before, we knew what we didn't know. Now we fully know what we have, in-depth, and how to manage those devices according to our business priorities. It's truly a game-changer."
That's what happens when you have visibility.
What would change for your organization if you actually knew what was on your network?
➡️Read the full case study for more: hubs.ly/Q03RYJql0
#healthcarecybersecurity #IoT #patientsafety
16
If you struggle with visibility into your device ecosystem, here's where to start:
1️⃣ Step 1: Map your current state
List out all of the devices on your network. Figure out who owns them.
Most importantly, name the gaps.
2️⃣ Step 2: Identify your crown jewels
Not all devices are equal. Start here: which connected devices are involved in direct patient care or processing ePHI? Which systems can you NOT do without?
ICU monitors. Medical imaging systems. Pathology. Ventilators. These are your tier-1.
Everything else is noise until you've secured these.
3️⃣ Step 3: Map Network Position
Knowing you have an infusion pump means nothing. Knowing it's on the clinical network connected to the main EHR running 2010 firmware = actual risk.
Document: device → network segment → what it connects to → firmware status.
4️⃣ Step 4: Establish Baseline for Active Threats
Document your network behavior (data flows, protocols, user and service access).
This shows what your device behavior SHOULD look like.
Then you can monitor for indicators of compromise (IoCs).
Alert fatigue kills programs. Focus detection on what matters.
Most teams tell us mapping tier-1 devices and their network position is their biggest blocker, how are you handling it? 👀
#healthcarecybersecurity #IoT #riskmanagement #Visibility
12
Here's a question most hospitals can't answer: "Do you know every connected medical device on your network?" Not estimate. Know.
Most teams stop here because the answer is no. It's not laziness. Medical device ecosystems are complex. 🤔
👉🏻 You have devices from 1997 next to 2025 tech.
👉🏻 Legacy systems.
👉🏻 New systems added by different teams.
Without continuous visibility into every connected device on your network, you're flying blind.
That means... you’re making security decisions blind. You're patching vulnerabilities that don't matter while missing the ones that do.🚨
Telling auditors you've got it while knowing you don't.
✨ The solution is not to just have visibility, it’s complete network visibility WITHOUT disrupting patient care.
What's your biggest blocker to getting full visibility?
#healthcarecybersecurity #cybersecurity #MedicalDeviceSecurity #CyberRiskManagement
16
Happy Halloween from Team Cylera! 🎃
While others are worried about ghosts and goblins, healthcare CISOs are losing sleep over something scarier:
"Do we actually know what devices are on our network?"
The real monsters aren't in the closet. They're the unknown vulnerabilities hiding in your infrastructure.
But here's the good news....visibility changes everything. No more sleepless nights wondering what you're missing or those pesky "ghost devices" lurking in your hospital network. 💥
Have a safe (and visible) Halloween! 👻
16
Cybersecurity shouldn’t depend on your zip code. 🏥🔐
If you’re leading cybersecurity at a rural or community hospital, the odds often feel stacked against you. Limited budgets, legacy systems, and a growing number of connected devices make defense harder by the day.
But here’s the truth:
💡 You don’t need more tools...you need the right ones.
💡 Ones built for real-time visibility, risk prioritization, and minimal staff lift.
💡 Ones designed for clinical environments, not just corporate IT.
Because protecting patient care shouldn’t require a 30-person SOC.
📖 Learn how modern IoT cybersecurity helps rural hospitals stay resilient:
hubs.la/Q03LldWg0
#RuralHospitals #HealthcareCybersecurity #IoTSecurity #PatientCare #HospitalIT
15
What if your device usage data could prevent downtime and cyber risk? 🤔
Hospitals are filled with connected devices—from infusion pumps to imaging systems—all generating usage data 24/7. But most institutions treat that data as operations-only.
What if it could do more?
IoT analytics can turn device usage patterns into actionable cybersecurity intelligence. For example:
👉🏻 Detect abnormal behavior like an infusion pump sending traffic to unknown servers.
👉🏻 Flag devices pending patch or overdue maintenance based on actual usage.
👉🏻 Identify underutilized assets, enabling smarter capital allocation and risk reduction.
In essence, analytics bridges the gap between uptime and proactive security. It helps CISOs and clinical ops teams spot risk before it turns into an incident.
The real ask: Are you using your healthcare IoT analytics only for operations—or also to fuel security, risk prioritization, and resilience?
🧠 IoT usage isn’t just data—it’s early detection.
Read the blog to learn more: hubs.la/Q03zmZb50
#HealthcareCybersecurity #IoTAnalytics #MedicalIoT #RiskPrioritization #OperationalEfficiency #PatientSafety
25
📰 1.4M patient records breached. Detection took 13 months.
Radiology Associates of Richmond just disclosed a breach from April 2024 affecting imaging files PHI.
However, this is more than just another breach.
1️⃣ Long dwell times aren’t just about tech, it's about architecture. This wasn’t a failure to react. It was a failure to see and the truth is: many clinical environments still can’t see what’s happening inside their own diagnostic systems.
2️⃣ Radiology and imaging are outside the security perimeter. Many hospitals still treat PACS, CT/MRI consoles, and imaging workstations as “infrastructure,” not as endpoints. 🚨 But attackers don’t care how you classify them.🚨 They care that they’re unmonitored, unpatched, and almost always left out of visibility tooling.
3️⃣ What can’t be seen can’t be audited... or protected. By the time the breach was discovered, a year had passed. At that point, it’s not just a data breach. It’s an operational one. How many diagnostics were performed on systems under attacker control? What else moved laterally while SOCs had no visibility?
👉 🔍 Healthcare IoT visibility isn’t a checkbox.
It’s an architectural imperative.
👇 How are you extending visibility into clinical imaging and diagnostic systems?
🗞️ News article: hubs.la/Q03y57yw0
#healthcarecybersecurity #IoTsecurity #medicaldevices #CISO #patientrisk #visibility #clinicalsecurity
31
⚠️ “HIPAA Requires Asset Identification” ≠ “You Have Visibility.”
Here’s the regulatory reality:
✅ HIPAA’s Security Rule requires an ongoing, accurate, and thorough risk analysis of potential threats to ePHI.
✅ That obligation necessarily includes identifying all systems and devices that create, receive, maintain, or transmit ePHI.
✅ Many hospitals meet this minimum by maintaining a static inventory spreadsheet to “check the box” for audits.
But let’s be clear:
Compliance ≠ security.
📌 Real visibility means understanding device behavior, communication paths, and clinical context in real time.
If your “inventory” doesn’t help you see lateral movement risk or detect anomalies, it doesn’t fulfill the spirit of HIPAA and it won’t secure your patients.
#HealthcareCybersecurity #HealthITSecurity #MedicalDeviceSecurity #CyberRiskManagement
25
📰 Russian ransomware attack now linked to patient death in NHS King’s College Hospital in London.
This isn’t hypothetical anymore. We need to treat this as the real-world consequence of security architecture failures.
✅ Clinical systems are critical systems. When a pathology network goes down, it’s not about IT inconvenience. It means transfusions, surgeries, chemotherapy regimens get paused. Critical labs can’t process. Downtime isn’t abstract, it’s life-critical.
But our networks weren’t built with that dependency in mind.
Many NHS Trusts and US hospitals still run flat or poorly segmented networks and without real-time visibility into their devices, networks, or potential threats. Clinical systems like lab analyzers, PACS, medical devices are accessible from the same VLANs as administrative IT.
➡️ Once threat actors breach via phishing or remote access, lateral movement is trivial.
➡️ Lab systems often use outdated, unsupported OSes with no EDR.
➡️ Vendors often have unmonitored remote access.
Cybersecurity leaders in healthcare must drive the message: this isn’t about protecting data, it’s about protecting care delivery itself. Attackers understand that. It’s time defenders did too.
👉 That means real-time visibility, segmentation, threat detection, and vendor access controls tailored for clinical environments.
👇 How are you evolving your segmentation and visibility strategies in light of events like this?
Read the full article: hubs.ly/Q03wvr7c0
38
In healthcare, seconds matter. So does visibility. Yet too many security teams still rely on point-in-time assessments to understand what's connected to their networks. That approach might have worked a decade ago, but today's reality is different.
In our latest blog, we explore why healthcare needs to move beyond static asset inventories to embrace continuous, real-time visibility that empowers early detection and faster, more informed responses.
📖 hubs.la/Q03wksHx0
#HealthcareCybersecurity #MedicalDeviceSecurity
14
Great conversations. Honest challenges. Real momentum. Last week’s Cisco Public Sector Solutions Summit in Birmingham delivered all of it. 🎉
Thank you to @Cisco for hosting such an important event and to everyone who visited our booth to talk about building safer, more resilient NHS services. Let’s keep these conversations going. 💪🏻
#NHSCyber #UKPublicSector #HealthcareSecurity #CyberResilience #AIReady #CiscoPartner #PatientSafety



27
🇺🇸 Wishing everyone a safe and restful Fourth of July!
As we celebrate Independence Day, we’re reminded that protecting what matters most requires both vigilance and collaboration.
In healthcare, that means safeguarding the systems, data, and people who deliver critical care every day. At Cylera, we’re proud to support the mission of securing healthcare IoT and medical devices so patient care can continue uninterrupted, even on the busiest holidays.
To our colleagues, partners, and friends: enjoy the celebrations, stay safe, and thank you for all you do.
#FourthOfJuly #IndependenceDay #HealthcareSecurity #PatientSafet
14
Still relying on spreadsheets to track your NHS estate?
You’re not alone, but it’s risky.
Many Trusts still lack a complete view of their connected environment, especially unmanaged IoT and medical devices.
Asset discovery is no longer a nice-to-have, it’s a requirement under DSPT and CAF.
At Cylera, we support NHS Trusts with automated asset inventory that updates in real-time and gives cyber teams the visibility they need.
Learn More: hubs.la/Q03vxF2N0
18
NHS Digital has issued an alert for a critical vulnerability in MicroDicom DICOM Viewer.
Exploitation could allow attackers to gain remote access, escalate privileges, and move laterally across connected clinical systems.
This is another clear reminder: IoT and medical devices aren’t isolated—they’re deeply integrated into hospital networks. Securing them requires more than patching alone.
Effective defence means combining patch management (where possible), network segmentation, and behaviour-based threat detection to contain and respond to threats before they impact patient care.
📖 Read the full NHS Digital alert:
hubs.la/Q03vcs9J0
#HealthcareCybersecurity #NHS #IoTSecurity #MedicalDeviceSecurity #ThreatDetection #PatientSafety
1
26
How many connected devices are on your network? Now ask yourself...how many do you know about? 👀💡
In a single hospital, tens of thousands of IoT and medical devices are silently operating, some critical, others forgotten. But every unmanaged or unknown device represents a potential risk.
Imagine a hospital where every device is visible, every vulnerability is identified, and risks are mitigated. That’s what Cylera enables with IoT Discovery and Inventory: a complete, real-time picture of your network.
Visibility isn’t just data; it’s power. Power to protect patients, secure systems, and build trust.
Is your asset inventory as complete as you think it is?
#HealthcareCybersecurity #AssetVisibility #IoTSecurity #HospitalIT
14
A ransomware attack has now been linked to a patient’s death in the UK—a devastating reminder that cybersecurity in healthcare is not optional. It’s critical to patient safety.
According to BBC reports, a June 2024 cyberattack on NHS pathology services delayed blood test results, contributing to a patient’s death. The attack disrupted over 10,000 appointments, canceled surgeries, and leaked nearly 400GB of sensitive data.
This wasn’t just a breach of systems—it was a breach of care.
At Cylera, we believe that secure, reliable care delivery depends on resilient digital infrastructure. When pathology systems go down, when devices are compromised, when data is held hostage—patients pay the price.
Healthcare organizations must act now to strengthen their cyber defenses. Because every second counts. And every patient matters.
Read the full article: hubs.la/Q03tQrPz0
#HealthcareCybersecurity #PatientSafety #CyberResilience #Ransomware #ConnectedCare #Cylera
51
Capital planning in healthcare has never been more complex—or more scrutinized.
Procurement teams are being asked to do more with less. But many are still making decisions based on static inventories or incomplete device data.
📆 Tomorrow at 10:00 AM ET, join Cylera’s Steve Brigden and Maureen Sahualla to explore how health systems are using IoT analytics to:
✅ Uncover hidden utilization gaps
✅ Identify over- and under-purchased device types
✅ Align real-world device usage with long-term procurement strategy
When procurement leaders have access to live device intelligence, strategy becomes precision.
🔗Save your seat: hubs.la/Q03swXMc0
#IoTCybersecurity #HealthcareIoTAnalytics #HealthcareIoTCybersecurity

20
Thousands of connected devices. Dozens of departments.
But every day, critical assets sit idle—untracked and underutilized.
This isn’t just waste—it’s risk.
Mismatched fleets drive up capital costs, obscure compliance gaps, and strain clinical operations. Most healthcare systems don’t have the analytics to spot the pattern until the budget cycle forces their hand.
On June 25 at 10 AM ET, our experts will explore how leading health systems are using IoT data to:
✅ Optimize device availability across sites
✅ Reduce capital strain
✅ Improve scheduling, staffing, and compliance readiness
All without clinical disruption.
🔗Save your seat: hubs.ly/Q03swVG_0
#IoTCybersecurity #HealthcareIoTAnalytics #HealthcareIoTCybersecurity

15