
Medical Director of the Inflammatory Bowel Disease Program at Froedtert and the Medical College of WI dedicated to caring for Crohn's and Colitis patients
Joined August 2013
- Tweets 752
- Following 447
- Followers 1,260
- Likes 668
45 Photos and videos










Daniel J. Stein retweeted

3 Dec 2025
A dream came true - I matched into GI at Medical College of Wisconsin! 🌟
So grateful for my mentors, family, and friends who made this journey possible.
Dr. Yaseen Perbtani @EndoAthlete @docbraymd #GIMatch #GI #MCW #NRMP
34
10
384
15,841
Daniel J. Stein retweeted

19 Jun 2025
First year of GI fellowship ✅
✨ Honored to receive the Dodds-Shaker Research Excellence Award
🎓 Congratulations to the graduating class of 2025!
#WomenInGI #MCWGI



15
6
120
8,519
Daniel J. Stein retweeted
4 May 2025



4
11
699
Daniel J. Stein retweeted

10 Jan 2025
Congratulations to our fellows and faculty on being awarded the Edmund M. Barbour, MD, Endowed Research Fellowship in Gastroenterology Fund for their research!
We look forward to the impact of their work!
#MCWGI
2
6
1,251
Daniel J. Stein retweeted
11 Oct 2024
Milwaukee GI Society IBD Debate
MCW fellows 🤝 Aurora Fellows
“Medical vs surgical management of a complex UC patient”
Excellent debate by both teams moderated by Sumona Saha, MD and @BeniwalPatelMD, proud of our 2nd year GI fellows Judie Hoilat and Mary Nemer!
#MCWGI #IBD



3
10
1,528

20 May 2023
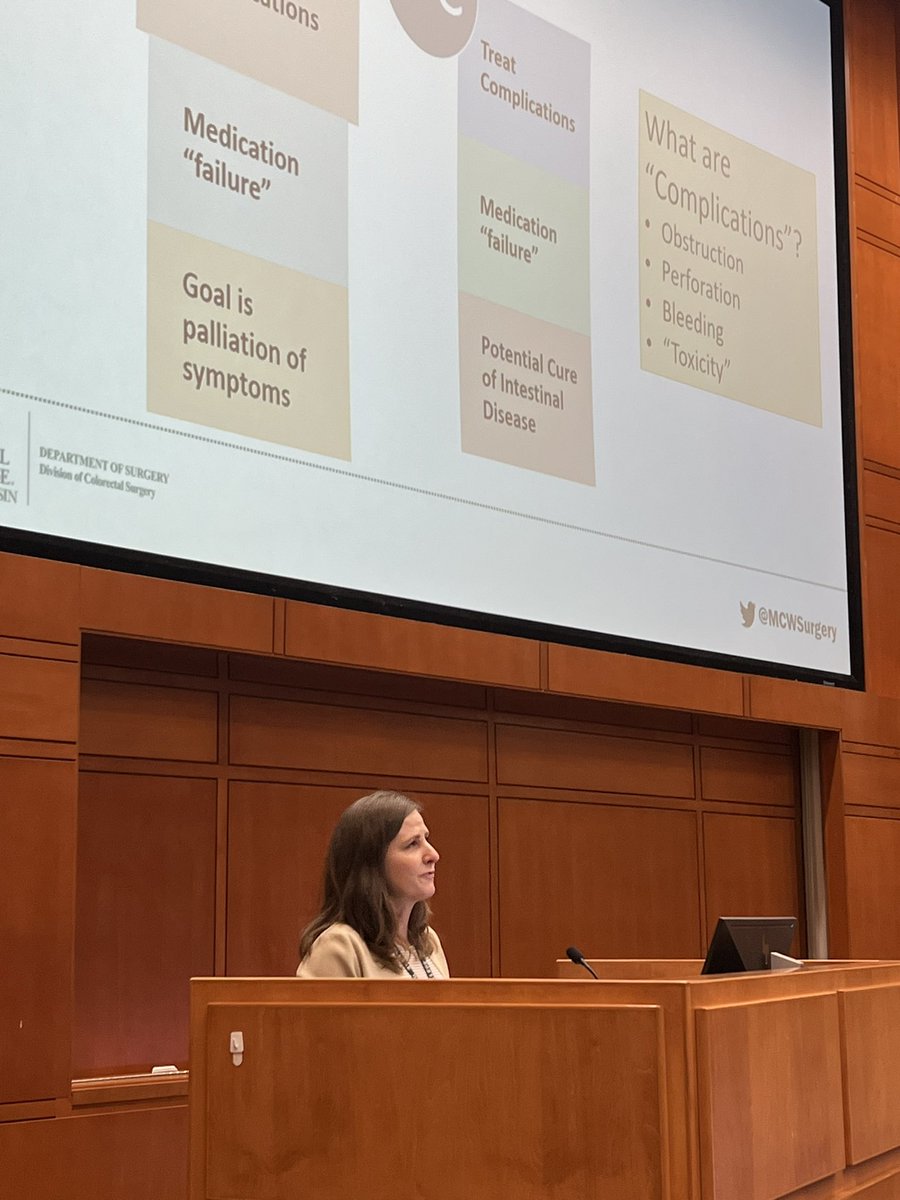
Dr. Carrie Peterson from @MCWSurgery talking about when to call your colorectal surgeon in #IBD #Crohns #ulcerativecolitis
2
5
9
1,292
20 May 2023
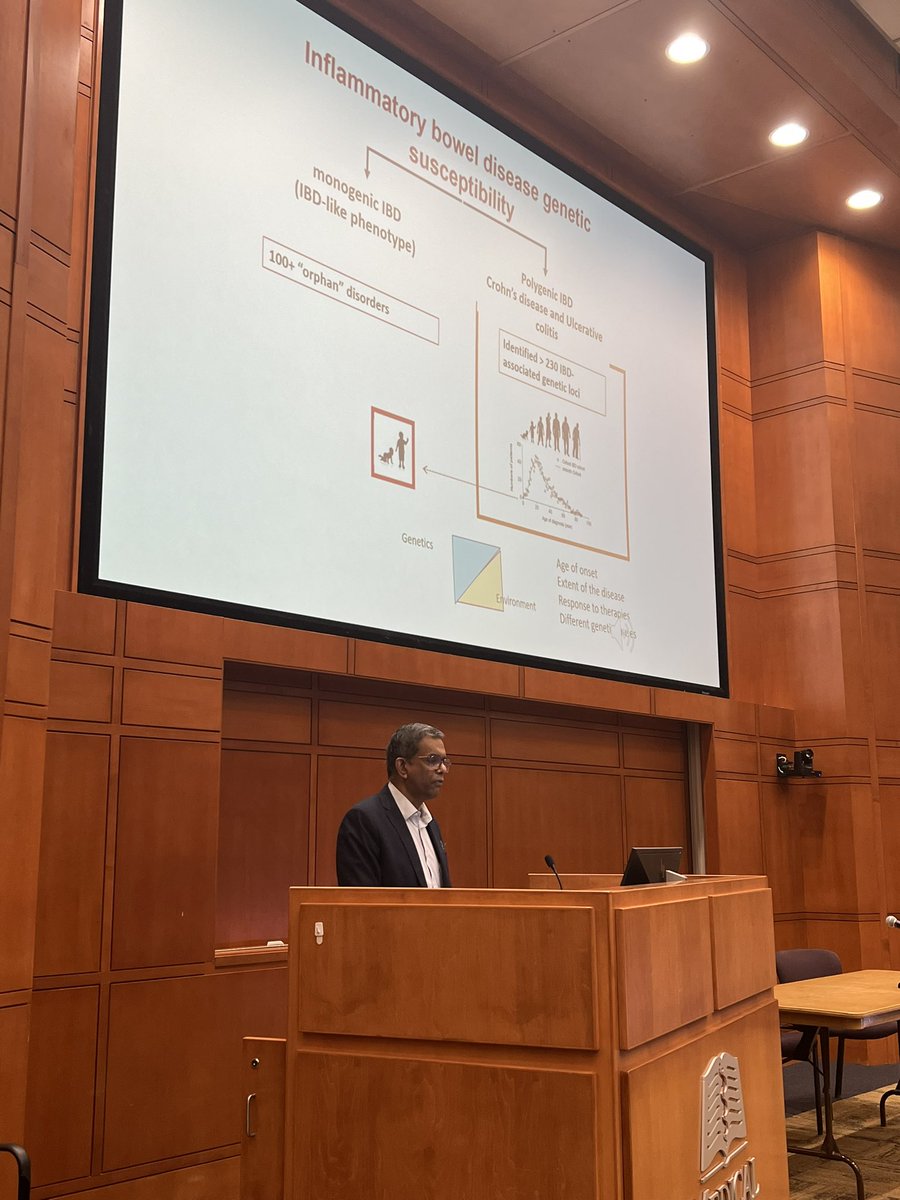
Dr. Subra Kugathasan Genetics and #IBD at @MedicalCollege @CrohnsColitisFn Patient and Provider Conference. Whole genome sequencing will be a game changer for the future of #CrohnsDisease therapy
2
7
865
Daniel J. Stein retweeted

9 May 2023
Some of our star fellows killing it @DDWMeeting @DDW2023 #MCWFellows #MedicalCollegeofWisconsin @w_pagani

2
6
595
Daniel J. Stein retweeted

5 May 2023
#IBDMasterClass @NorthwesternMed
@ibdgijami
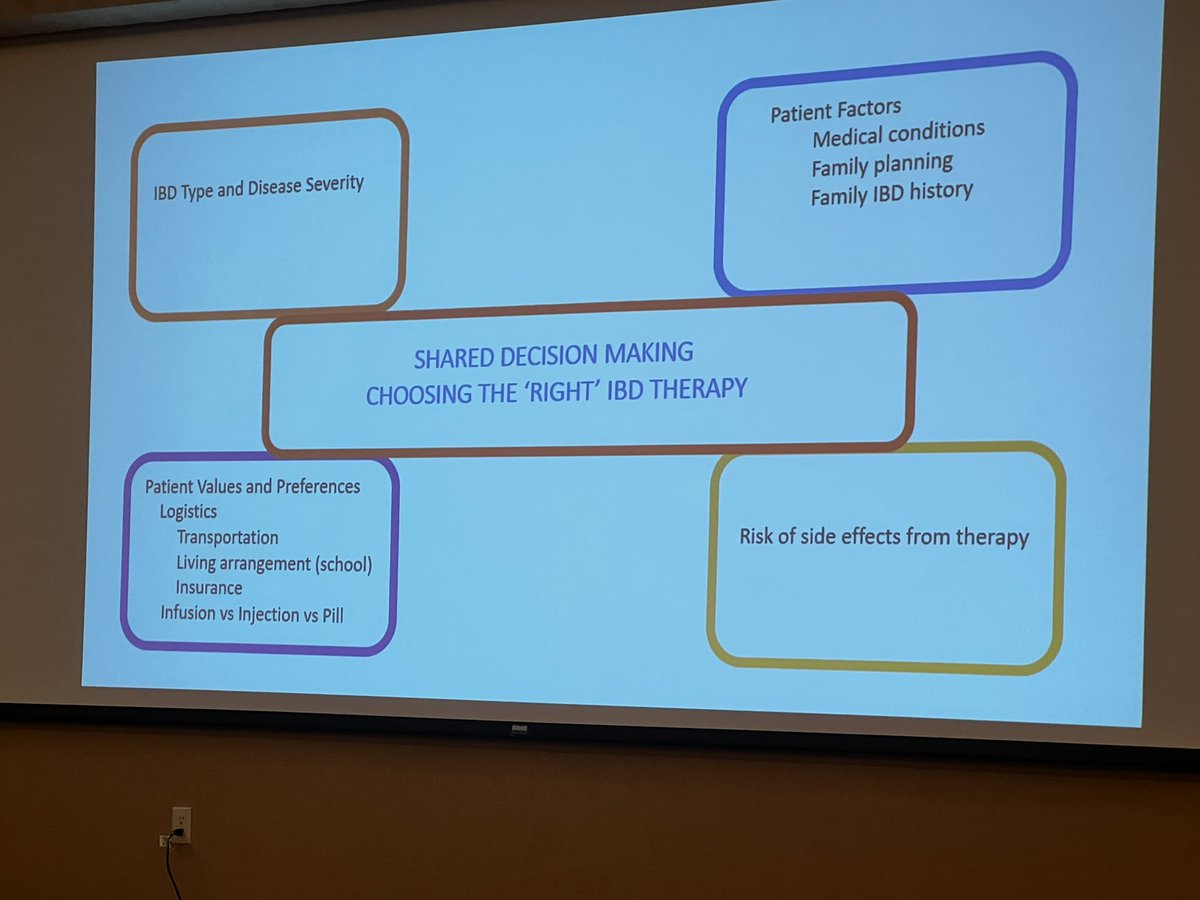
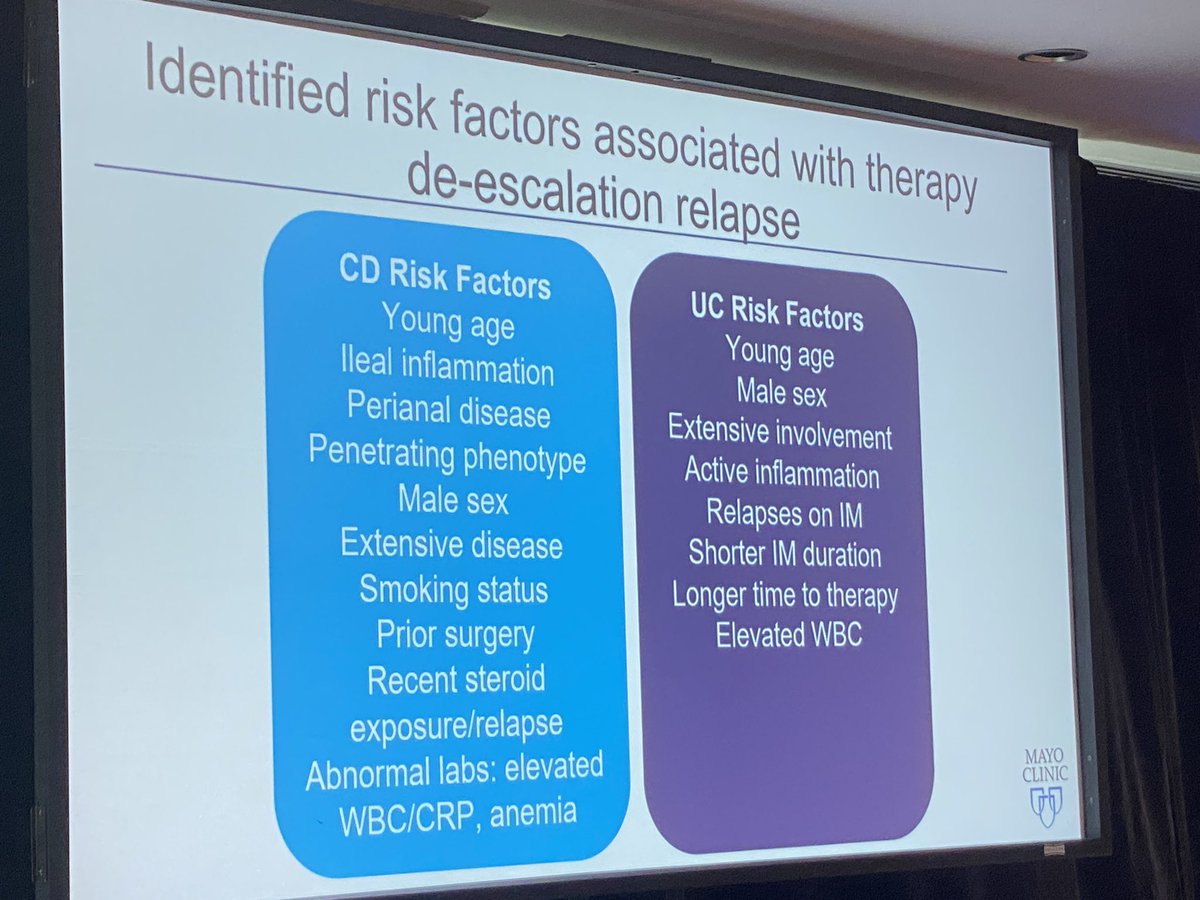
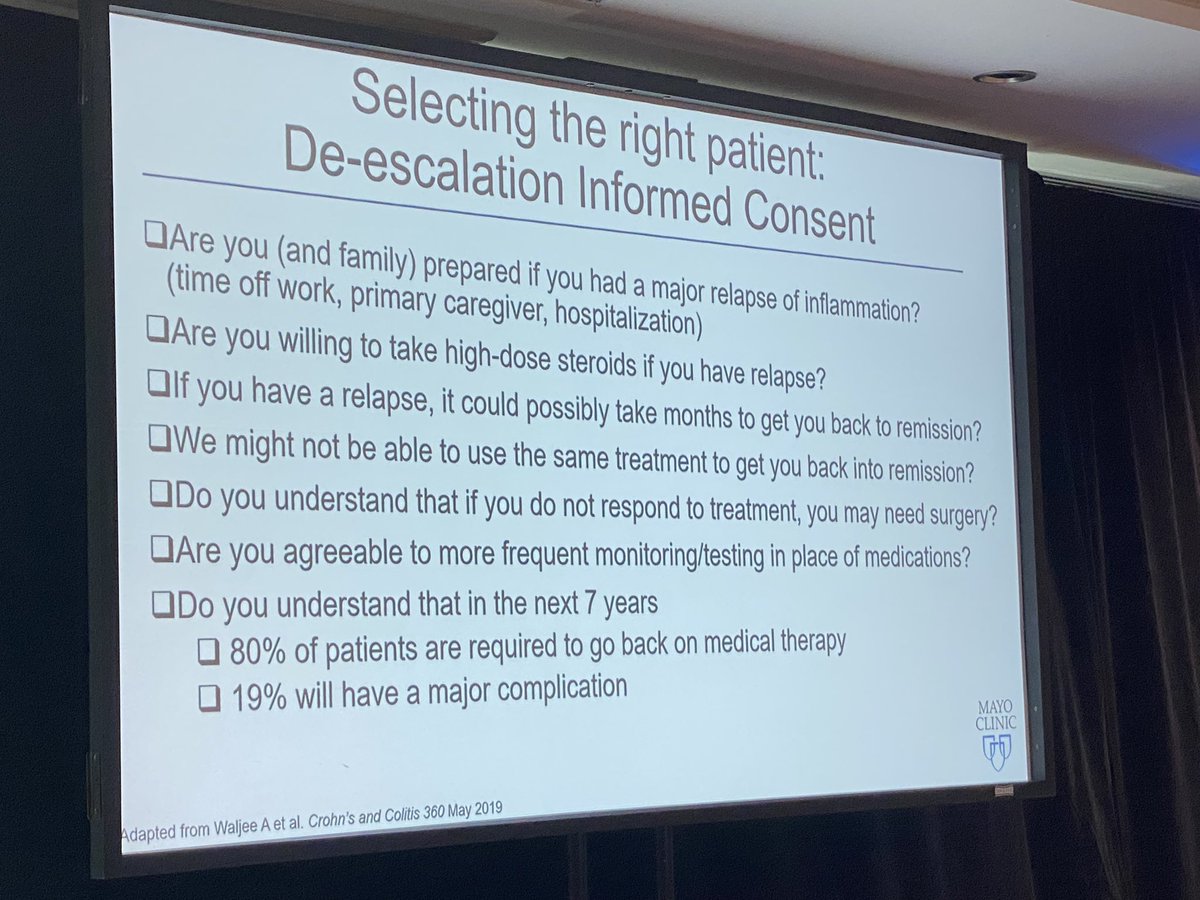
💎Who is NOT a good candidate for #IBD therapy de-escalation? 📸 👇🏽
💎#DrKinnucan shares her ✅ list when having this convo w the patient 📝 👇🏽
@ShahidaDin1 @ibddoctor
1
4
12
1,267
Daniel J. Stein retweeted
2 May 2023
Thread 2/4 Key points: Need to consider SB ACA in CD pt with change in phenotype. Crohn's about 10Xs gen pop for SB ACA. RFs: ♂️, young age at Dx, long disease duration, multiple resections, diverted bowel, immunosuppressive use. All of which our patient had.
1
2
5
842
Daniel J. Stein retweeted
2 May 2023
Thread 1/4 NL CRP,⬇️🔥 on CT 🚫 response to IV steroids🟰fibrotic stricture. CT angiography neg.. Enteroscopy not attempted d/t dilated SB. ALSO phenotype change: melena and weight loss raised 🚩🚩. So ✂️ and found to have jejunal adenoCA, 🚫nodes or metz.
1
2
4
820
Daniel J. Stein retweeted

2 May 2023
Nutrition is also a huge part of managing this case. Depending upon how much weight he has lost and how little he is eating, may need to start TPN. This would also help optimize nutritional status if he needs surgery.
1
5
277
Daniel J. Stein retweeted
2 May 2023
Active UGI bleeding a concern here. Have people seen this in #crohns patients and what’s it from?
Where are my MCW/UW peeps?
@ibdnaik @BeniwalPatelMD @dr_fcalderaibd @SinhIBD
28%
Active inflammation
46%
Anastomotic ulcer
18%
Malignancy
8%
PUD
39 votes • Final results
2
5
450
Daniel J. Stein retweeted
1 May 2023
32 w SB #Crohns x15yrs, ICR jejunal✂️for sympt strictures 3 yrs ago. Presents w SBO, CT: jejunal🔥->IV steroids started IFX 10mg/kg.
4mos later: Wt loss, abdo pain, melena. Hgb 6,CRP nl, IFX 10. CT: SBO, jejunal thickening, ⬇️🔥. Not better on IV steroids x48hrs.
What's next?
16%
TPN & change Rx
19%
EEN change Rx
24%
Enteroscopy/Bx/Dilation
41%
✂️Surgical Resection
148 votes • Final results
11
9
18
6,984
Daniel J. Stein retweeted

1 May 2023
#GITwitter Join us now for a convo w @DSTEINGIMD @DCharabaty
🎯How do you approach Recurrent/Refractory/Progressive SB stricturing #Crohns
🗳️#IBDPoll👇🏽,RT & Share your 💬 !
🆓#CME👉🏼bit.ly/3k6SHG8
Supported by educational grants @AbbVie @TakedaPharma
1
11
22
7,490
Daniel J. Stein retweeted

30 Apr 2023
Join @DSTEINGIMD from @MedicalCollege TOMORROW 🗓️ 5/1 for #MondayNightIBD ‼️
Come learn about #SmallBowel #Crohns management 📝🤓
#IBD #GITwitter #IBDTwitter
@Mcw_Medchiefs @MondayNightIBD
30 Apr 2023

#GITwitter Let’s flex our #IBD 🧠 before DDW !
🗓️Join the Convo May 1 w @DSTEINGIMD
🎯Recurrent/refractory SB stricturing #Crohns
🗳️#PreConvo #IBDPoll👇🏽
🆓#CME👉🏼bit.ly/3k6SHG8
Supported by educational grants @AbbVie @TakedaPharma
📌Where are you in your career?
2
8
1,989
22 Apr 2023
Great thread
21 Apr 2023

The ACIP recently recommended additional updated bivalent dose for adults ages 65 years and older and for people who are immunocompromised.
1) At this time while some patients with IBD may qualify I think most patients don't need an additional dose know.
@AmCollegeGastro
279
Daniel J. Stein retweeted

16 Jan 2023
The risk of CV disease in JAK inhibitors is controversial Hyperlipidemia might have to be factored in. Although lipid abnormalities trend back to baseline over time. pubmed.ncbi.nlm.nih.gov/3287… @BeniwalPatelMD @DCharabaty @dr_fcalderaibd @EdwardLoftus2
3
1
7
415
Daniel J. Stein retweeted
16 Jan 2023
56 yo M, #BMI of 54, Hyperlipidemia, Pan-UC, LOR to IFX due to anti-drug antibodies, now symptomatic on vedo Q 4 weeks. Albumin 3.2. Flex Sig: Mayo 3 left sided colitis.
What's the best next option?
13%
Adalimumab 6 MP
42%
JAKi (Upa or Tofa)
39%
Ustekinumab
6%
Colectomy
267 votes • Final results
11
11
16
7,523