
Enterprise Head & Neck Disease Group Chair @MayoCancerCare. Head & Neck Division Chair @MayoRadOnc.
Joined October 2019
- Tweets 525
- Following 503
- Followers 1,270
- Likes 2,444
50 Photos and videos













Daniel Ma retweeted

15 Oct 2025
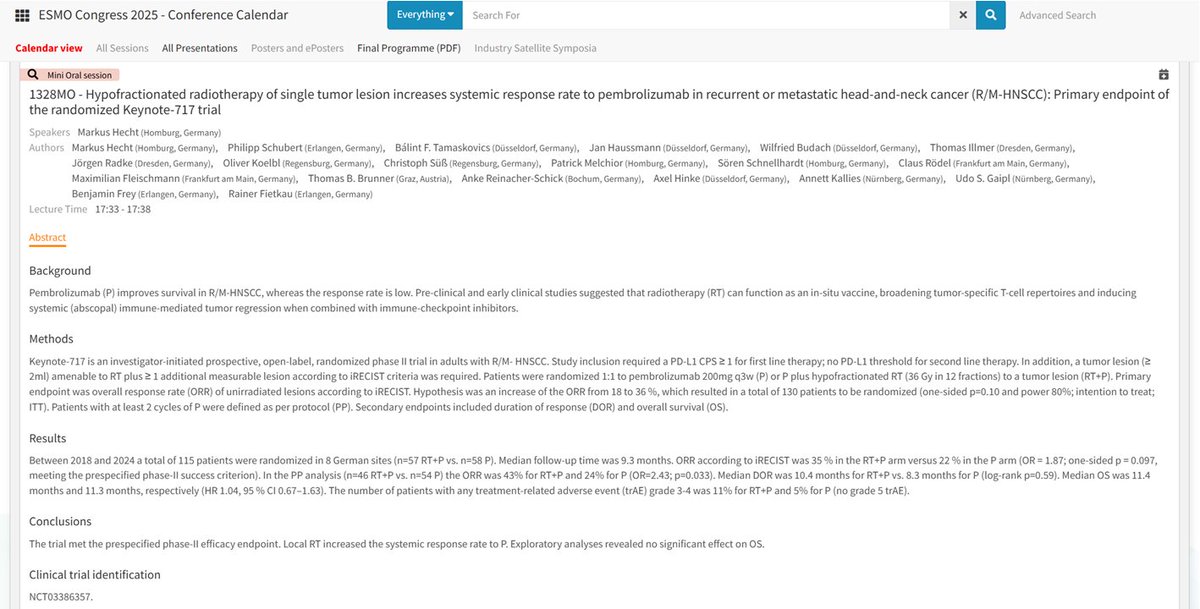
🗣️☢️Intriguing abstract #ESMO25 - possible increased systemic response after hypofractionated RT (36Gy/12fx) with pembro for R/M-HNSCC?
Looking forward to more details!
1
4
29
2,099

30 Sep 2025
3
4
36
4,721
30 Sep 2025
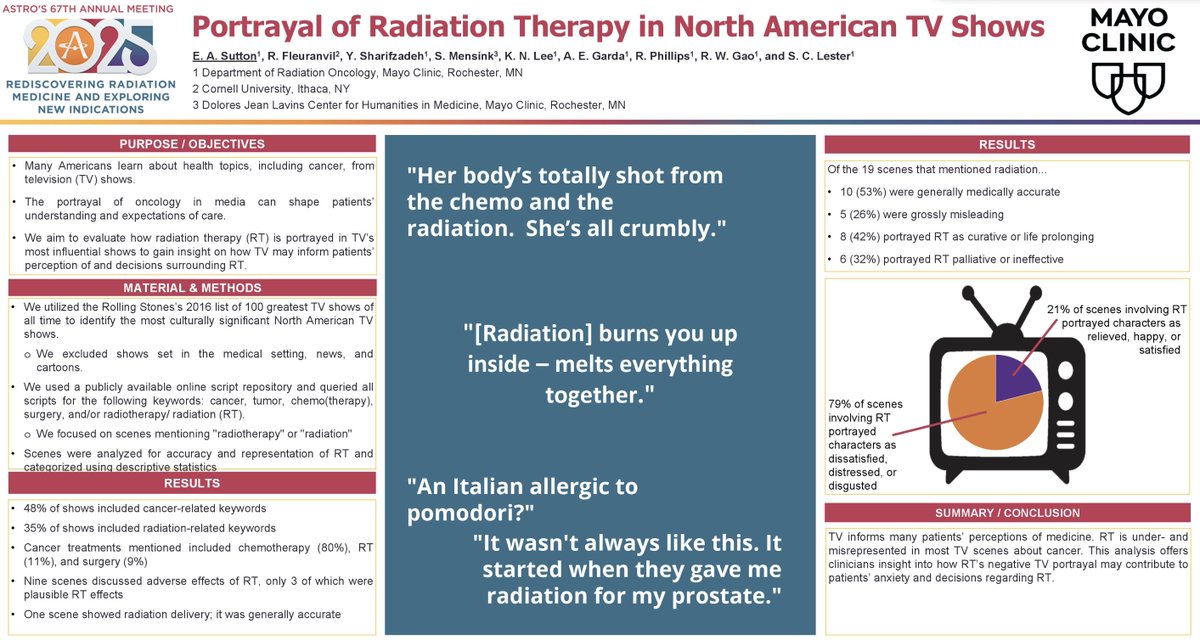
Great work by @MayoRadOnc emphasizing our specialty’s need to engage with the cultural perception of radiation.
Congrats to Drs. Elsa Sutton, Scott Lester, and the study team for this unique perspective. #ASTRO2025
27 Sep 2025

An intriguing poster at #ASTRO25 demonstrates that major North American TV Shows are leading viewers to believe radiation might cause "internal melting, burning, or crumbling, or even a food allergy". @ASTRO_org @PRJeffWhite @NehaVapiwala @sueyom poster.astro.org/astro/2025/…
3
6
1,296
29 Sep 2025
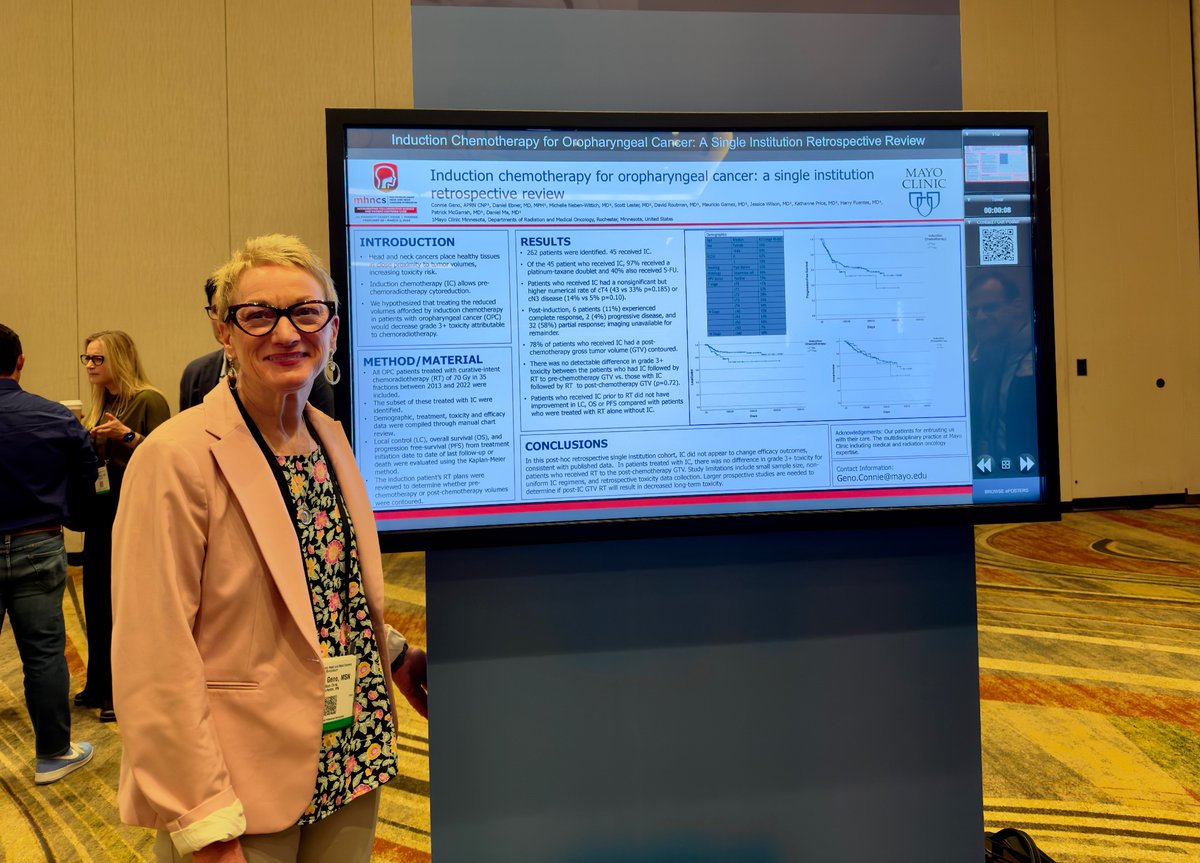
Congrats to @DavidRoutmanMD @KatieVanAbelMD @LindaXYinMD and our stellar MS4 Cecelia Hidalgo for presenting our real world data with DART (30-36 Gy) for HPVOPC.
282 patients and 97% PFS for int risk group. DART is a standard tx for int risk pts @MayoCancerCare
#ASTRO25
1
8
29
2,179
11 Sep 2025
Thank you @DavidSherMD and the other commentators for their insightful thoughts concerning MC1675 (DART).
It's a pleasure and privilege to respond back to their astute observations, which I'll include below.
7 Sep 2025

It was such a pleasure to read the results of this juicy and terrific randomized trial of postop RT dose de-escalation for HPV OPSCC from @DanielMaMD and colleagues at @MayoRadOnc.
The field has been waiting for the formal results, and this paper does not disappoint.
thelancet.com/journals/lanon…
3
7
29
3,549
11 Sep 2025
5. Finally, more research in biological selection is needed. Whether it's functional imaging ala @imrtlee, ctDNA ala @DavidRoutmanMD, AI-assisted involved node selection ala @DavidSherMD, or chromosome instability ala @pipcosper (and many more strategies!), we need better data.
2
6
421
11 Sep 2025
This is a population that continues to grow with the ongoing HPV epidemic, one that doesn't look to end soon. We owe it to them to continue exploring better options.
Grateful as always to @MayoRadOnc @MayoCancerCare @MayoClinicENT and esp our pts for supporting this work.
5
280
11 Sep 2025
Absolute numbers for recurrence were small, so perhaps we were unlucky. But it's challenging for me to reconcile a difference in primarily distant control based upon differences in locoregional RT dose.
I would stress our thoughts on cis vs doce are hypothesis generating.
1
65
11 Sep 2025
Concerning the int risk (ENE-) cohort, the AJCC 7 table regrettably requires a correction.
The majority of of int risk pts were AJCC N2b. AJCC staging changed mid study which introduced some confusion in the CRFs. This was caught post-pub and a correction is actively pending.
3
4
258
11 Sep 2025
We were very happy to report a statistically sig difference in grade 3 toxicity, and like David points out, a large difference in grade 2 toxicity. This is reflected in the SS difference in patient QOL even at 2 years. Grade 2s really do matter.
1
71