
California Vascular Health Specialists #aorta #AortaEd #AAA #aneurysm #aorticdissection #carotid #CLTI #CLI #PAD #spinalaccess No disclosures.
Joined October 2019
- Tweets 2,722
- Following 1,671
- Followers 2,301
- Likes 4,749
142 Photos and videos














Devin Zarkowsky retweeted
A health system can own the hospital.
You only get to operate in it.
That asymmetry is written into law.
Stark and the 2010 freeze on new physician-owned hospitals pushed physicians away from ownership and toward employment.
You generate the cases.
You create the facility revenue.
The margin compounds on a balance sheet you will never control.
A raise has a ceiling.
Ownership compounds.
2
5
35
1,781
Devin Zarkowsky retweeted

Jun 13
This needs to be on a Times Square Billboard! 50% of health care spending is going to hospitals.
The majority of which pay no taxes, and their version of community benefit is:
1. Paying the CEO $30 million
2. Suing patients for unpaid bills that qualify for their
Financial assistance policy
3. Opening up offshore investment funds
4. Sponsoring professional sports teams
5. Closing down less profitable service lines like
labor and delivery units
6. Putting the 340B money into the general fund
7. Lapping up the facility fees
8. Spending more money on administration than patient
care
9. Having zero fear that the IRS will pull their nonprofit
status
There is NO justification for a hospital system to own hospitals across state lines!
Jun 12

Hospital care hit $1.635T in 2024 (31% of total NHE), but that undercounts the real footprint ✨significantly✨
With hospitals & health systems now owning/employing ~47% of U.S. physicians, they control a massive slice of the additional $1.11T in physician & clinical services too - pushing their total influence on healthcare spending well beyond the $1.6T headline.
Note that’s just the physicians and clinical services category. They own in every NHE category - that spend is never quantified correctly.
Vertical integration changes the math. Hospitals and health systems control ~49% of the total healthcare spend.
It’s enormous.
21
135
403
18,014

Great philosophy from a master musician with a unique technical skill on how to flourish professionally over 45 years. Essentially a template for independent medicine’s survival. @stevevai
@DutchRojas @DrBruggeman @cscla @HeathVeuleman @sdixitmd @mcuban
fb.watch/HGHcd3sNAq/?mibexti…
2
1
3
298
Devin Zarkowsky retweeted

The optimal amount of fraud is somewhere between zero and infinity.
Helpful analysis, I know, but hear me out.
If a system is so restrictive that it takes mountains of paperwork and diverts significant resources away from patient care just to catch a few additional fraud dollars, then we should just allow the fraud and let people focus on patient care. The optimal amount of fraud is not zero.
Conversely, if there are billions of dollars in fraud, some non fraudulent activities will get caught up in the regulatory process. For example, there are probably some people who will lose their coverage unjustly due to work requirements. But if the result of 10 people losing coverage is billions of dollars available for patient care that weren’t previously, that’s an acceptable, if regrettable, trade off.
Of course, politically, each side claims the other is only focused on the downside and not the upside of each debate. Larry knows this and is preempting the debate.
Jun 11

I'm going to make a guess now that any further health care changes Republicans propose will be described as going after fraud but will actually go well beyond that.
4
3
24
6,893
Devin Zarkowsky retweeted

Jun 10
We compare prices for gas, flights, and home repairs. Healthcare shouldn’t be the one exception.
Patients deserve clear, upfront pricing so they can make informed decisions and keep more money in their pockets. That's exactly what my Patients Deserve Price Tags Act will do.
15
11
72
16,469
Devin Zarkowsky retweeted

Jun 11
Day 4: The transparency we need but aren’t asking for
If the transparency we have built mostly serves payers and systems, what would transparency aimed at the real cost driver look like? It would make consolidation visible.
The single most useful disclosure in American health care today is not another posted chargemaster. It is a reliable, public answer to a simple question for any given service. Is the billing provider independent? Or is this physician employed by and billing through a hospital system? Is the service being delivered and billed as a hospital outpatient department? Today that answer is deliberately hard to find, and the difficulty is not an accident. It is the hidden process through which consolidation converts the same care into a higher bill.
Congress is thankfully already circling this. The Bipartisan Policy Center has highlighted the Fair Billing Act, S. 2497, introduced by Sens. Hassan and Marshall, which would require hospitals to use unique billing identification numbers at each off-campus location. That sounds boring and technical but it is foundational. Without distinct identifiers you cannot track where a service was actually furnished, you cannot measure how volume migrates from physician offices into hospital outpatient departments after an acquisition, and you cannot enforce site-neutral payment with any precision. MedPAC has documented the disparities, finding the same chemotherapy infusion reimbursed at a rate 186 percent higher in a hospital outpatient department than in a physician office. CMS has begun closing a narrow slice of that gap, extending site-neutral payment to drug administration in off-campus HOPDs beginning in 2026, a change CMS estimated would save roughly 290 million dollars in its first year. CBO has estimated that aligning payment for services commonly provided in physician offices across both on and off-campus HOPDs would save on the order of 157 billion dollars over a decade. That is the size of the prize sitting behind a billing identifier; a prize worth fighting for.
NASHP has developed site-neutral model legislation for states built on MedPAC's 2023 recommendation, and an analysis of New York's approach found savings of more than 1 billion dollars for commercial payers had they paid site-neutral rates for low-complexity services in 2022. The states moving on this understand something the federal price-posting debate keeps missing. The lever is not posting what a service costs on a wall. It is shining a light on where the service is billed from and who owns the provider billing it.
This is the transparency that would actually bend costs in a meaningful way. Not another file of negotiated rates for payers to mine, but structural disclosure of employment and billing site that lets patients, employers, and regulators see how referrals are kept inside systems and how acquisition turns a physician office into a higher-cost hospital outpatient department.

3
4
250
Devin Zarkowsky retweeted

Jun 10
𝐓𝐡𝐞 𝐡𝐨𝐬𝐩𝐢𝐭𝐚𝐥 𝐥𝐨𝐛𝐛𝐲 𝐬𝐚𝐲𝐬 𝐩𝐡𝐲𝐬𝐢𝐜𝐢𝐚𝐧-𝐨𝐰𝐧𝐞𝐝 𝐡𝐨𝐬𝐩𝐢𝐭𝐚𝐥𝐬 𝐜𝐚𝐧’𝐭 𝐛𝐞 𝐭𝐫𝐮𝐬𝐭𝐞𝐝.
HCA paid a $1.7 billion fraud settlement.
Tenet paid $2.5 billion.
UHS paid $122 million.
That is $4.7 billion from three Federation of Hospital (FAH) board companies.
But sure.
The danger is the surgeon who owns the building.

ALT Pop-art comic image depicting the CEO of FAH at a podium saying “We don’t oppose physician ownership!” while hiding a red “BAN” stamp behind her back. A physician in a white coat holds keys beside a small physician-owned hospital, emphasizing the gap between public messaging and lobbying against physician-owned hospital competition.
7
48
147
6,164
Devin Zarkowsky retweeted
Jun 9
A non-profit health system can refer a patient to its own MRI, its own lab, its own surgery center, and bill all three.
An independent does that once and it's a federal felony.
Same referral.
Same patient.
One of you goes to prison.
It's called Stark Law.
Read who's exempt.
The asymmetry is the whole business model.
16
101
384
9,435
Devin Zarkowsky retweeted
Why Doctors Aren't Allowed To Own Hospitals In America youtu.be/ZBQyOHgt59U?si=VFqT… via @YouTube The RealDocSpeaks Podcast episode with @HeathVeuleman is now live!
A few of the highlights:
• Discussion of the prohibition of POHs
• The origin of Stark laws and how hospitals use them
to arbitrage physician productivity
• How hospital chargemasters are calculated
• Advice for new doctors
• The need for physicians to organize
• Steps HHS can take TODAY to improve healthcare
• The need for physicians to speak up and take back
their power
@HeathVeuleman @HEALTHCOSTtruth @DutchRojas @DrCorriel @DrDiGiorgio @anish_koka @drdanchoi @Laffincrow @noahkaufmanmd
4
13
2,188
Devin Zarkowsky retweeted
1) we need to pay PCPs more
2) that doesn’t mean that we need to pay specialists or surgeons more
3) your implication that “specialists” rule the RUC has several flaws
- there are far more cognitive specialty votes that surgeons. It’s not even close
- the RUC is an advisory body. The government makes the final decisions
Let’s stop the infighting and attempts to try and show my specialty is more deserving than yours. I think we can all agree that
1) everyone needs more
2) the overall system is flawed and whatever influence/impact the RUC has is minimal compared to a litany of other issues
1
1
11
449
Exactly. That is my practice as well: no way in 2026 someone visits my office if the consultation is $1,000 .

This is why it’s important for doctors to retake independent practice.
A doctor will not charge thousands for a 15 min consultation. No independent practice could have prices that high and actually compete.
But a hospital, once it buys a clinic, can inflate that charge with facility fees and other coding shenanigans.
The patients think the doctor is charging that much but it’s actually the health system.
273
Devin Zarkowsky retweeted
This is why it’s important for doctors to retake independent practice.
A doctor will not charge thousands for a 15 min consultation. No independent practice could have prices that high and actually compete.
But a hospital, once it buys a clinic, can inflate that charge with facility fees and other coding shenanigans.
The patients think the doctor is charging that much but it’s actually the health system.

Are you sure about that? Some doctors charge thousands for a 15 minute consultation. I think they are overpaid.
Medicine should not be like some magic money tree. We all will have some sort of health problems, therefore that knowledge to help should be available at reasonable cost.
Certainly not thousands per 15 minutes!
I get it, for doctors the risk is high, but so are other professions.
15
26
171
22,310
Devin Zarkowsky retweeted
Mark and I disagree with USA Today.
Jun 6

All doctors are underpaid.
9
9
184
13,351
Devin Zarkowsky retweeted
Breaking news:
Trade association admits its facilities run too inefficiently to stay open without government largess.

Did you know that nearly 70% of Texas hospitals would close outpatient clinics if facility fees were prohibited?
13
20
137
8,654
Devin Zarkowsky retweeted
Jun 5
“We lose money on Medicare” is the most expensive sentence in American healthcare.
It is an accounting choice, not a fact.
Allocate overhead one way and the wing is a charity. Allocate it the other way and it’s a profit center.
The same CFO does both, in the same quarter, depending on who is reading.

6
16
104
17,943
Devin Zarkowsky retweeted
Jun 2
Nothing says “expanding access” like a tax-exempt health system protected by CON laws, federal exemptions, above-market reimbursement, and the freedom to roll up geography one press release at a time, while the ultimate liability lands on the New York taxpayer.
Good thing the NY Attorney General’s office has always been famous for aggressive nonprofit oversight.
Solid work.

As part of its comprehensive strategy to expand access to the highest-quality care across Long Island, NYU Langone Health today announced plans to build a world-class, state-of-the-art academic medical center in Melville: bit.ly/3PRzY58

5
13
120
7,364
Devin Zarkowsky retweeted

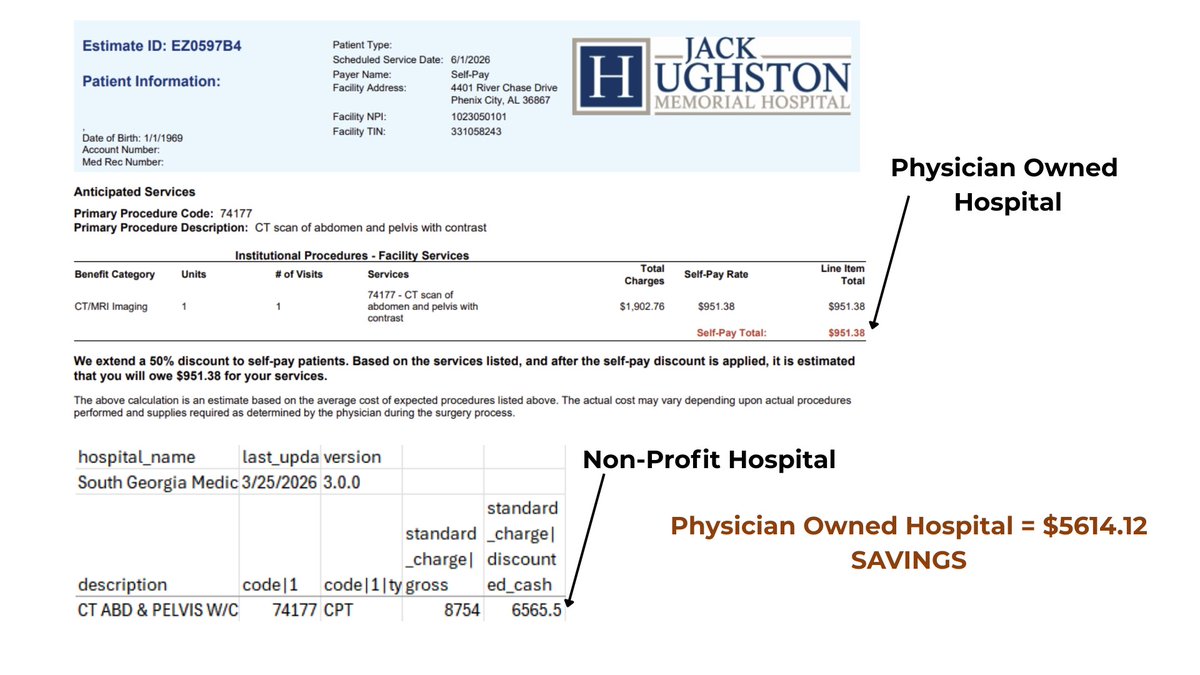
$5,614.12 saved on a single CT scan.
Same procedure code (74177 — CT abdomen and pelvis with contrast). Two hospitals. One bill.
Physician-owned hospital (pays real estate taxes, gets no grants): $951.38 self-pay.
Non-profit hospital (pays no real estate taxes, receives federal and state grants): $6,565.50 cash price.
There's a lot of discussion lately about whether physician-owned hospitals inflate charges as massively as non-profits. This is one example from my personal experience. The "non-profit" charged nearly 7x more for the same scan than the for-profit physician-owned hospital.
Section 6001 of the ACA froze new physician-owned hospitals in 2010. The hospital lobby called it patient protection. The data calls it competition suppression.
We all got screwed when they stopped physicians from owning hospitals.
Section 6001 should be repealed.
Do your homework. Support the hospitals that help us. Avoid the ones that don't. Simple as 1-2-3.
#healthcarecosts #POH
2
22
67
4,183
Devin Zarkowsky retweeted
Jun 1
“Nonprofit” is a tax status. It says nothing about how much the hospital keeps, what it pays its executives, or how little reaches a patient who can’t pay.
The community benefit it reports?
It writes the definition, grades itself, and files with an agency that audits almost none of them.
5
26
89
2,199
Devin Zarkowsky retweeted

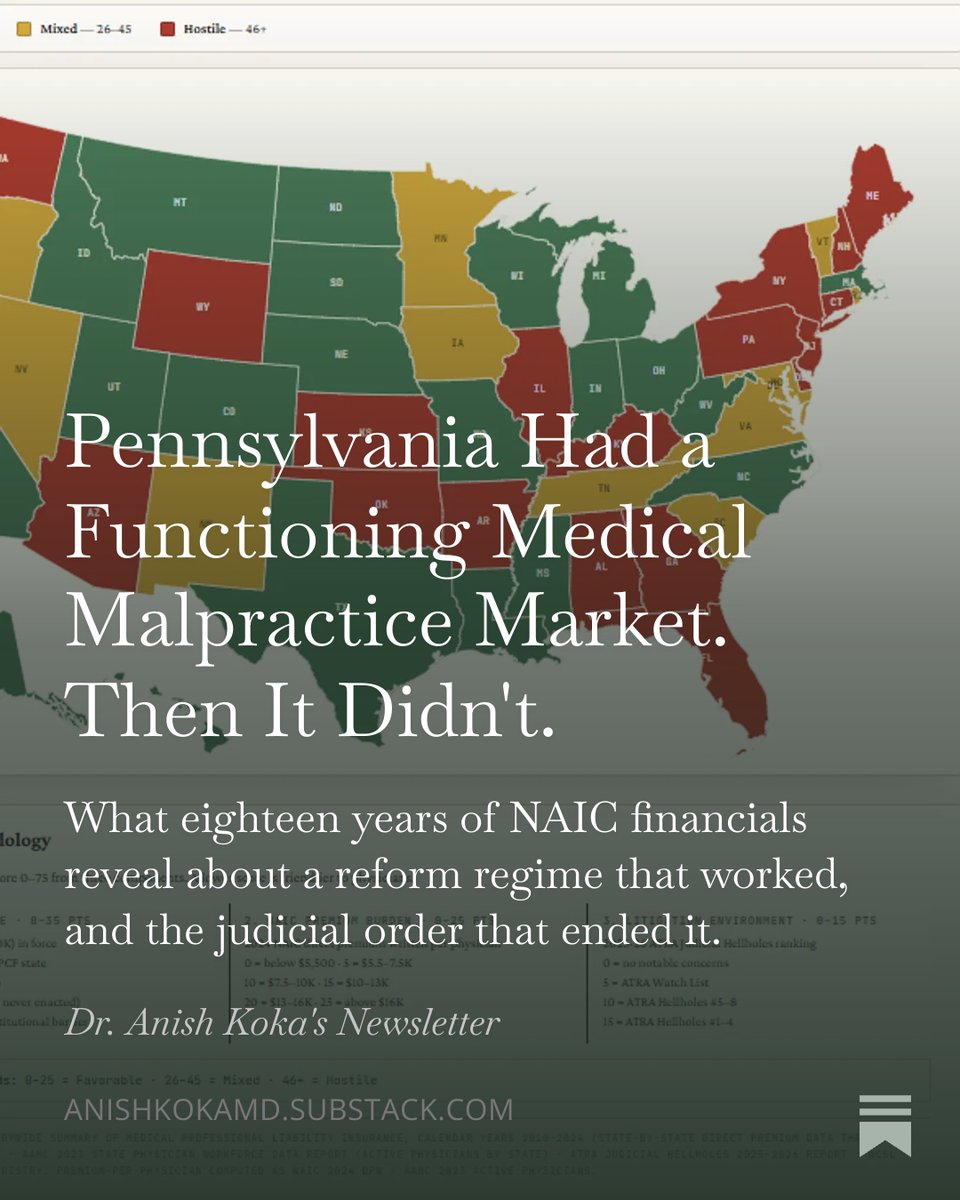
May 31
THREAD: The medical malpractice market is broken, and the data proves it.
A physician's interpretation of the insurance market on what's happening. 🧵

4
12
81
23,768
Devin Zarkowsky retweeted
This thread is a perfect example of Hayek’s fatal conceit.
Here a pro- central planning pundit points to one preferred version of price setting, declares that it “works,” and then treats every other failure of price setting as somehow unrelated.
Maryland has all payer hospital rate setting and global budgets. You like the outcome, so that counts as smart planning (not to mention Maryland has plenty of flaws).
Medicaid pays pediatricians far below commercial rates, patients struggle to find doctors who participate, and suddenly that is not a problem with rate setting per se. That is just the wrong rate setters, or the wrong politicians, or the wrong program. Or Medicare pays hospitals 5x what a doctors office charges. Just the wrong central planners again.
But the core problem is the same. No commission has access to the dispersed knowledge needed to set the right price at the local level.
It cannot know the capacity of each pediatric office, staff wages, rent, malpractice costs, supplies, local demand, physician burnout, opportunity cost, patient urgency, or how much a parent values being seen today instead of six weeks from now.
Prices are signals that coordinate resource use in the face of scarcity.
When planners suppress or manipulate prices, the cost does not vanish.
That is the unseen harm.
The fatal conceit is believing the problem is never central planning itself. It is always that the right central planners have not been put in charge yet.
If the concern is access, subsidize patients. Give people purchasing power. Do not pretend a commission can calculate the right price for every clinical situation from above.
There’s zero reason that every American can’t have access to pediatrician visits without any more government involvement than a means tested cash equivalent subsidy. There’s no more of a market failure there than with food.
But central planners don’t want that. They just want control.

Overly simplistic argument *designed* to cast ALL rate setting as "socialism."
Price controls don't invalidate rights. They're often used to protect rights when market power prevents genuinely voluntary exchange (ie: HC).
Should humans have different values based on income?
1
11
42
4,424