
Psychiatrist by training. Science communicator by choice. Making mental health make sense in English, Marathi, and plain human. 🧠 Cricket enthusiast| Kolhapur
Joined March 2016
- Tweets 3,060
- Following 289
- Followers 357
- Likes 1,387
212 Photos and videos










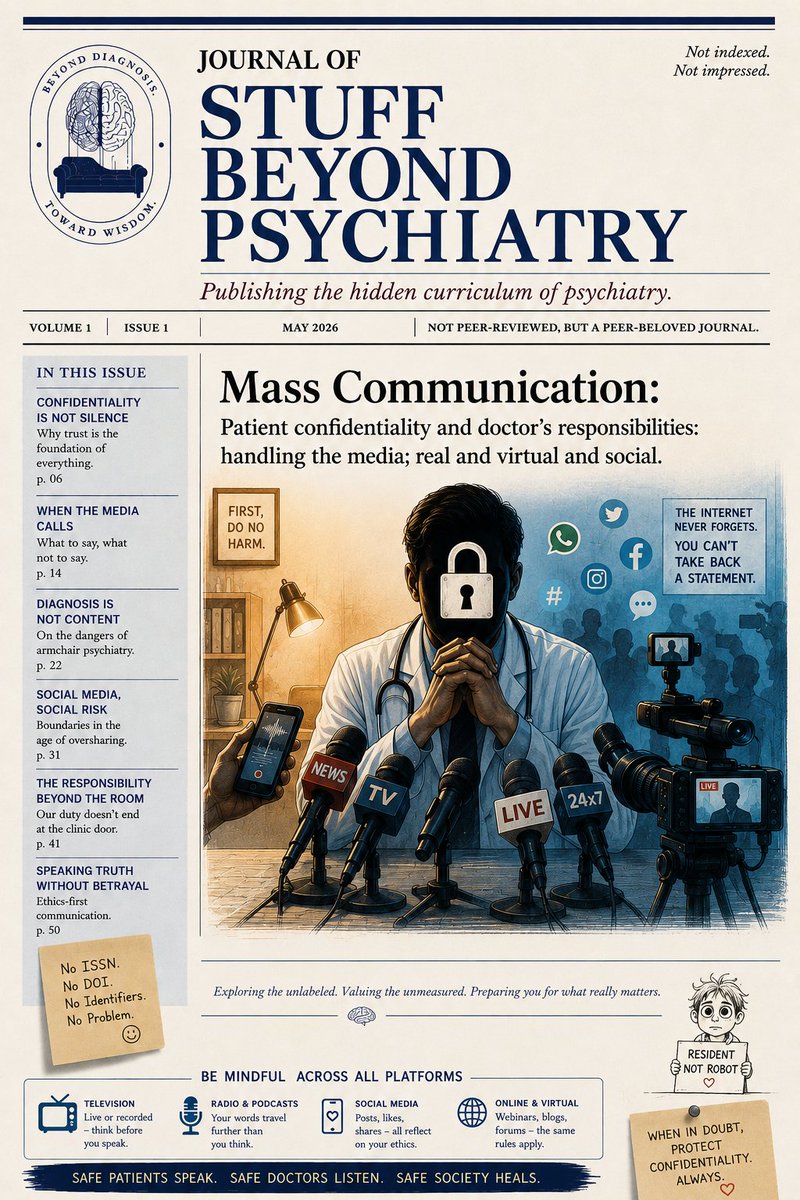

The Journal Of Stuff Beyond Psychiatry
May 2026. Volume 1, Issue 2.
THE GEOMETRY OF CONFIDENTIALITY
Or: how a single sentence can collapse an entire profession.
Psychiatrists, rather all doctors often worry about saying the wrong thing to a patient. Far fewer worry about saying the wrong thing to a journalist.
That is strange. The damage from a careless media interaction is usually much larger, more permanent, and impossible to take back.
◆ ◆ ◆
Confidentiality is not just about "not revealing secrets." It is about protecting a boundary so absolute that patients can speak without calculating future consequences.
The moment that boundary looks negotiable, psychiatry changes shape.
A patient who fears exposure does not stop suffering. He stops speaking.
◆ ◆ ◆
A common myth: confidentiality is breached only when a doctor names a patient. False.
You can breach it without naming anyone.
▪️ "An actor I treated..."
▪️ "A well-known politician once told me..."
▪️ "A famous cricketer with depression..."
▪️ "A celebrity from this city..."
Even hinting that someone was your patient can be a breach. Confidentiality protects not just the content of treatment, but the existence of the relationship itself.
"Yes, he consulted me" is already confidential information.
Many clinicians believe vagueness protects them. It does not. The media runs on triangulation. Tiny fragments become identity.
Age, city, diagnosis, timeline, profession, family, hospital, one quoted sentence. Each detail narrows the circle.
People become recognizable once enough narrative crumbs are scattered.
Journalists know this.
Audiences know this.
Doctors should know it too.
◆ ◆ ◆
The performance of proximity.
There is another temptation. Some doctors subtly signal closeness to powerful people to borrow their prestige.
"I cannot disclose names, but many celebrities consult psychiatrists."
This is usually dressed up as awareness-building. Often it is advertising wearing ethical clothing.
The doctor looks trustworthy while hinting at access to important people. A strange contradiction: "Trust me because I keep secrets. Here is a small sample of the secrets I keep."
◆ ◆ ◆
The safest principle is surprisingly simple.
▪️ Never discuss identifiable patients.
▪️ Never confirm or deny relationships.
▪️ Never offer "off the record" anecdotes you would hate to see on tomorrow's front page.
Because they might.
◆ ◆ ◆
This matters most after suicides, crimes, celebrity deaths, divorces, addictions, or public controversies. The media urgently wants psychiatric interpretation.
A psychiatrist is suddenly expected to be translator, profiler, and moral narrator all at once. That pressure produces some of the worst ethics in medicine.
Doctors speculate on diagnoses from TV interviews.
Comment on medications.
Discuss personality traits.
Analyse people they have never met.
Or worse, imply insider knowledge.
Psychiatry then slowly turns from a medical discipline into entertainment commentary.
The audience may enjoy it.
The profession rots from it.
◆ ◆ ◆
So what should a psychiatrist actually do with the media?
Speak in principles, not particulars. Disorders, not patients. Patterns, not identities. Public education, not private histories.
Good media psychiatry sounds almost disappointingly general.
▪️ "What can families watch out for?"
▪️ "How does addiction affect judgement?"
▪️ "What myths exist about bipolar disorder?"
▪️ "When should someone seek help?"
These educate society without sacrificing individuals.
◆ ◆ ◆
A useful test.
If the patient were sitting beside you while you spoke to the media, would they feel protected?
Not flattered.
Protected.
Because patients do not just hand over information. They hand over vulnerability, trusting it will stay contained.
Confidentiality is not silence. It is containment.
And once containment cracks, people stop bringing fragile things into the room.
That is the real cost of careless media behaviour.
Not embarrassment.
Not lawsuits.
Not disciplinary action.
The real cost is that future patients begin editing themselves before they speak.
◆ ◆ ◆
WHEN THE MEDIA CALLS
✓ Speak in principles, not particulars.
✓ Discuss disorders, not patients.
✓ Educate the public, reduce stigma.
✓ Protect identity, always.
✓ Neither confirm nor deny relationships.
✓ Ask: would the patient beside me feel protected?
✗ Do not name or identify patients.
✗ Do not hint, imply, or allude.
✗ Do not share anecdotes or stories.
✗ Do not discuss cases from your practice.
✗ Do not speculate on the diagnosis or behaviour of anyone you have not examined.
✗ Do not share "off the record" information.
◆ Confidentiality protects not only what is said, but the fact that someone is your patient.
◆ Your duty to your patient continues outside the clinic.
◆ In the age of realtime news and social media, responsibility is continuous and public.
- Dr Devavrat Harshe
@psychidiaries, here you go.
Sorry, I forgot to upload this one as promised earlier.
#MedTwitter
#PsychTwitter
#Neurotwitter
5
171

Jun 14
ओदिशा.
नावातच दिशा आहे.

🚨 Odisha has announced free education from kindergarten (KG) to postgraduate (PG) level in all government-run institutions across the state. 👏🏼

1
45
Jun 13
The Evolution of a Liar
Erikson and Piaget, explained through one boy, his imaginary cat, and a lifetime of steadily improving fiction
Psychiatry loves developmental theories. Every resident memorises two of them the night before an exam.
Piaget described how a child's thinking changes with age. Erikson described what each age is emotionally busy with. Both tables get forgotten the moment the exam ends, because tables do not move. Children do.
So here is a trick to remember both, permanently. Pick one skill and watch it grow up across the stages. We picked lying.
A good lie needs almost everything the developing brain acquires: memory, the ability to imagine, impulse control, logic, and a sense of what other people know and don't know. Meet Chintu. We will follow his lies through life, and at each stage, notice the exact new skill that upgrades the lie.
◆ ◆ ◆
Age 2: The Terrible Truth
Sensorimotor · Trust vs Mistrust → Hope
Chintu has eaten half a box of biscuits. Crumbs all over his face.
"Chintu, did you eat the biscuits?"
"Yes."
Said bluntly, with an innocent smile. No lie here, because he does not yet have the skill that makes lying possible.
🔹 The skill still missing: mental representation. To lie, you have to hold two versions in your head at once, what really happened and a different version you say out loud. Chintu cannot do that yet. He has only just figured out that things still exist when they are hidden (object permanence). His mind deals only with what is right in front of him. There is no second version to offer.
At this age, honesty is not a virtue. It is a hardware limitation.
◆ ◆ ◆
Age 4: The Imaginary Cat
Preoperational · Initiative vs Guilt → Purpose
The biscuit jar is empty. Who ate them?
"The cat."
The family does not own a cat. But this is real progress. A whole set of new skills just came online:
🔹 Theory of mind — He now understands that other people have their own thoughts, and that those thoughts can be wrong. Which means they can be made wrong on purpose. This is the single skill that makes lying possible at all, and it arrives around age four.
🔹 Symbolic thinking — He can now let one thing stand for another. The same skill that lets a stick become a sword in play lets him conjure a cat that does not exist.
🔹 Imagination — He can picture a scene that never happened and describe it.
🔹 Language — The lie now has a little story, not just a flat "no."
🔹 The skill still missing: logic. So nobody checks the story against reality, least of all Chintu. He has the idea of a lie but no way to keep it standing. One follow-up question knocks it over:
"I didn't eat the biscuits."
"Then how do you know there were biscuits?"
It collapses, because he cannot yet think two steps ahead or keep his story consistent.
◆ ◆ ◆
Age 8: Evidence-Based Fiction
Concrete Operational · Industry vs Inferiority → Competence
Chintu sneaks chocolates from the fridge. Before anyone notices, he bins the wrappers, washes his hands, and goes back to his homework wearing the face of a boy who has been studying all evening.
"I don't know who ate them."
Now we are seeing planning. The new skills:
🔹 Logical, cause-and-effect thinking — His mind now follows real rules about how the world works, so his story actually holds together.
🔹 Reversibility — This is the big one. He can run a sequence backwards in his head. If I say this, she will check that, so I should deal with that first. This is the same skill that lets him solve "if 5 3 = 8, then 8 − 3 = 5." Here he uses it to cover his tracks before he speaks.
🔹 Second-order theory of mind — He tracks not just what you believe, but what you believe he believes. So he can perform innocence, not just claim it.
The lies have become less artistic and more procedural. Successful lying, he has worked out, is mostly about managing the evidence. Parents start to miss the imaginary cat.
◆ ◆ ◆
Age 15: Strategic Communication
Formal Operational · Identity vs Role Confusion → Fidelity
School reports poor attendance. Father asks why he was absent.
"We had project work outside school."
He has screenshots. He has briefed two friends. He has prepared for the follow-up questions. Every single word is technically defensible. The new skills:
🔹 Abstract and hypothetical thinking — He can now reason about situations that have not happened yet. What does Dad already know? What might he check? How do I stay one step ahead? He plays out the whole interrogation in advance.
🔹 Hypothetico-deductive reasoning — He can start from a principle and work out the consequences. He has figured out an abstract rule: a sentence with no false words in it cannot be proven false. So he switches from inventing lies to leaving things out and saying technically true things.
And here is the part that matters in clinic: much of childhood lying evolves with motives, specific to each developmental stage. In the first two stages, it is about avoiding consequences. In teenage, it is boundary-drawing. An attempt to keep a private self where an identity can be built without a parent watching. The four-year-old lied to escape consequences. The fifteen-year-old often lies to protect a self under construction. Same behaviour, different job.
◆ ◆ ◆
Age 25: The Grain of Truth
Intimacy vs Isolation → Love
Chintu is twenty minutes late to dinner with his fiancée.
"Traffic was terrible."
The traffic was fine. He left late because he was watching cricket highlights.
Piaget has nothing left to add. The thinking machinery was finished in adolescence. What adulthood adds is not a new skill but better calibration. This lie has a grain of truth in it, asks her to verify nothing, and protects the relationship rather than himself. Adults eventually learn that the most believable lies are mostly true, and the most forgivable ones are mostly small.
◆ ◆ ◆
Age 45: The Educational Lie
Generativity vs Stagnation → Care
Chintu now has a son who is avoiding homework.
"When I was your age, I always finished my homework before playing."
This bears only a passing resemblance to events documented earlier in this thread.
The lie is no longer self-protective. It is aimed forward in time, at a child who will one day use the exact same sentence on a child of his own. It is educational. Or so Chintu claims. Somewhere, an imaginary cat smiles.
◆ ◆ ◆
The Irony
We describe child development as the steady arrival of wonderful skills. Perspective-taking gives empathy. Imagination gives creativity. Planning gives achievement. Abstract reasoning gives science.
Every one of those skills also improves lying. A good lie runs on the exact same parts as healthy development:
🔹 Imagination, to invent an alternative
🔹 Theory of mind, to predict what the other person will believe
🔹 Reversibility and planning, to cover the tracks
🔹 Memory, to avoid contradicting yourself
🔹 Social skill, to make it land
So children do not learn to lie despite development. They learn to lie because of it.
The good news: the very same skills that allow deception also allow honesty, empathy, and real relationships.
◆ ◆ ◆
For the clinic, two quick notes:
🔹 Clumsy lying around age 3 to 4 is a milestone, not a moral emergency. It is the sign that theory of mind has arrived, right on schedule. Parents who turn up worried about a "defect" can usually be reassured.
🔹 The quality of a lie is a rough readout of thinking ability. An eight-year-old whose lies still fall apart on the first follow-up question, or who cannot lie at all, may be worth a closer look.
Piaget tells you what equipment the child has. Erikson tells you what the child is building with it.
Chintu, meanwhile, would like it on record that he has never lied in his life, and that this thread misquoted him.
#MedTwitter
#PsychTwitter
#NeuroTwitter
@psychidiaries
2
4
14
1,515


Case in point.
Take a look at this pitch.
x.com/i/status/2063531369779…

Too much talk about good and bad pitches.
Here is a different perspective.
Cricket is a game where the weather and the pitch play a crucial role.
Let's create a system where randomly, every team will play on say, 5 bad pitches in a season.
The quality of bad pitch can be standardized, just as we select the type of pitch and depth of cracks while playing Cricket on PS4.
Cricket rankings will include players' performance on Good and bad pitches, with more weight to their skills on a bad pitch.
Just like an entrance exam, where solving difficult questions carry more marks and weight.
Because, when one says, No 1 ranked batter, they are not just talking about number of runs, or boundaries, or averages. They should also mean skills, temperament.
What say, @ICC
@AMP86793444 @ABsay_ek @ajarrodkimber
#cricket
#ranking
Image courtesy
Google.
63
Too much talk about good and bad pitches.
Here is a different perspective.
Cricket is a game where the weather and the pitch play a crucial role.
Let's create a system where randomly, every team will play on say, 5 bad pitches in a season.
The quality of bad pitch can be standardized, just as we select the type of pitch and depth of cracks while playing Cricket on PS4.
Cricket rankings will include players' performance on Good and bad pitches, with more weight to their skills on a bad pitch.
Just like an entrance exam, where solving difficult questions carry more marks and weight.
Because, when one says, No 1 ranked batter, they are not just talking about number of runs, or boundaries, or averages. They should also mean skills, temperament.
What say, @ICC
@AMP86793444 @ABsay_ek @ajarrodkimber
#cricket
#ranking
Image courtesy
Google.
2
240
Journal Of Stuff Beyond #Psychiatry
June 2026. Volume 1, Issue 5
The Ollivander Phenomenon: Choosing the Right Drug for the Right Patient, and Why the Drug Sometimes Chooses the Patient
When Harry Potter first walks into Ollivanders, he expects to buy a wand the way he might buy a quill. Instead the old wandmaker tells him the relationship works the other way round. The wand senses some affinity that it alone can feel, and the wand picks him. Harry tries many wands. Most do nothing, and some make things worse. Only one gives off the warmth and the sparks of a real match. It is a useful and slightly playful image for a problem that sits close to the heart of clinical psychiatry. We talk about choosing a drug for a patient as if the choice ran one way and the patient just sat there. But even the most carefully evidence-based choice can fall flat, or do harm, in a given person, while a less obvious one can suddenly come to life. In a real sense, the drug chooses the patient too.
The simile is chosen on purpose. Efficacy shown in a trial population is a statement about the average of a group, whereas the patient sitting in front of us is one particular person, with their own physiology, beliefs and temperament, all of which decide whether the match holds. We use amitriptyline as our example because it captures the problem so well. It genuinely works, yet it carries so many adverse effects that it is often the wrong wand for the wizard.
The candidate molecule: amitriptyline
Amitriptyline is a tricyclic antidepressant (TCA) that blocks the reuptake of both serotonin and noradrenaline. It is approved for depression in adults, but these days it is used far more often off-label: for chronic pain, diabetic and post-herpetic neuropathy, fibromyalgia, migraine prevention, irritable bowel syndrome and insomnia. Its pain-relieving and sedating effects at low doses keep it useful decades after newer drugs arrived.
The trouble is that its pharmacology is far from clean. On top of the intended action on monoamines, amitriptyline also has anticholinergic, antihistaminic and alpha-adrenergic blocking effects, and together these produce its familiar list of side effects. To borrow the wandlore image, it is a powerful instrument with a temper of its own. It suits some hands and fights against others.
Efficacy weighed against safety
Nobody really doubts that amitriptyline works. The questions are about how well it is tolerated and how safe it is. It is no longer a first-line treatment for depression precisely because its side-effect load is heavy. Instead it tends to be kept for severe or treatment-resistant depression, or for patients who also have chronic pain or insomnia, where the sedation and pain relief become an advantage rather than a problem.
The common side effects are dry mouth, blurred vision, drowsiness, dizziness, constipation, difficulty passing urine, weight change and a drop in blood pressure on standing. The more serious worries include QT prolongation and the risk of dangerous heart rhythms, which make it a poor choice for many patients with cardiac disease, and overdose can be fatal. It can bring on or worsen narrow-angle glaucoma, and like other antidepressants it can tip a vulnerable patient into mania. The American Geriatrics Society Beers Criteria specifically advise against using amitriptyline in older adults because of its strong anticholinergic load.
Choosing badly: the wrong wand for the wizard
Amitriptyline's problem is rarely that it does not work. The problem is giving it to the wrong person. Hand it to a frail older patient, someone with heart disease, or someone at risk of overdose, and an effective drug turns into a dangerous one. Researchers are aware of this, which is why some have run systematic, placebo-controlled meta-analyses across many indications, trying to work out how much of the anticholinergic and other adverse-event burden comes from the drug itself rather than from the underlying illness or from nocebo effects. That effort is itself a quiet admission that the side effects we pin on a molecule belong partly to the patient and the setting.
When the patient shapes the side effects
This is where the Ollivander image really pays off. Two patients given the very same tablet can have very different experiences. Some of that is pharmacogenetics, but a good deal of it is expectation, which can produce symptoms on its own. This is the nocebo effect: expecting harm makes the harm more likely to be felt, and existing or unrelated symptoms get blamed on the new drug. What a patient expects, including the expectations we create during consent and counselling, has a strong effect on the side effects they then notice. A clinician's own doubts about a drug can make this worse.
Suggestibility and expectation
Several psychological traits have been studied as predictors of how a person responds to placebo and nocebo. The evidence here is mixed and should be read with care. Traits such as optimism, empathy and suggestibility have been linked mainly to placebo responses, while pessimism, anxiety and catastrophising have been linked mainly to nocebo responses. Neuroticism is the awkward case. Some experimental work has grouped it with the placebo-linked traits, but across the wider review literature it shows up far more consistently on the nocebo side, which is the finding we return to below. The practical message is simpler than the trait lists suggest. A patient who leaves the consulting room primed to expect a dry mouth and dizziness has, in part, been handed the script for those very symptoms.
Personality
When the focus narrows specifically to side effects and the nocebo response, the picture becomes much clearer. In reviews of nocebo risk factors, neuroticism is the trait most consistently and positively linked with the nocebo response, with pessimism and low optimism not far behind. A recent study went a step further and described how this works. People high in neuroticism report more bodily complaints even before any treatment begins, expect more side effects beforehand, and then show a stronger nocebo response afterwards. Crucially, the link between neuroticism and that response runs partly through those prior expectations rather than being separate from them. So temperament and expectation are not two rival explanations. They are two links in the same chain, and this is the sense in which neuroticism belongs on the nocebo side.
The evidence is not all one way. At least one case-control study found no clear link between neuroticism, health anxiety or common pharmacogenetic variants and self-reported trouble tolerating antidepressants, a reminder that these are tendencies rather than fixed rules. Even so, the broad weight of evidence points to something we can act on in the clinic: who the patient is helps decide whether a drug will suit them.
Prescribing as matching
If side effects are written jointly by the molecule and the patient, then good prescribing looks more like Ollivander's craft than a transaction at a vending machine. Three practical lessons follow. First, look at the wizard, not just the wand. Cardiac status, age, glaucoma and overdose risk are firm reasons to avoid amitriptyline, while temperament and expectation are softer factors that still sway how well it is tolerated. Second, frame expectations with care. Because the wording we use during consent can itself bring on symptoms, how we explain the risks is part of the treatment, not a neutral formality. Third, be ready to try a different wand. A poor match is information, not failure, and the right fit sometimes shows up only on the second or third attempt.
Conclusion
Ollivander's line, that the wand chooses the wizard, is a neat reversal of how we usually imagine authority working. Psychiatry holds the same reversal. Amitriptyline is effective, but its real safety and side-effect burden mean it is the right wand only in certain hands, and even then the patient's expectations, suggestibility and personality help decide whether the match will spark or just smoulder. Our job is not only to choose a drug. It is to recognise when a drug and a patient have chosen each other.
References:
Columbus C (director). Harry Potter and the Philosopher’s Stone [Sorcerer’s Stone]. Warner Bros. Pictures; 2001. Based on the novel by Rowling JK.
Faasse K, Petrie KJ. The nocebo effect: patient expectations and medication side effects. Postgrad Med J. 2013 Sep;89(1055):540-6. doi: 10.1136/postgradmedj-2012-131730. Epub 2013 Jul 10. PMID: 23842213.
Corsi N, Colloca L. Placebo and Nocebo Effects: The Advantage of Measuring Expectations and Psychological Factors. Front Psychol. 2017 Mar 6;8:308. doi: 10.3389/fpsyg.2017.00308. PMID: 28321201; PMCID: PMC5337503.
@psychidiaries
2
7
1,191
All of us have seen this. Headphones in a drawer. When pulled out, knots formed. Frustrating, right?
Science finds out the cause, and the solution.
Scientists dropped a string in a box, spun it for 10 seconds, opened it up, and a knot fell out. They did this 3,415 times.
The findings, which explain why your earphones hate you:
→ Under ~46cm: almost no knots. Too short to misbehave.
→ 46cm–1.5m: knot odds shoot up fast.
→ Past 1.5m: plateaus near 50%, not 100%, because a long string jams itself against the walls and stops tumbling.
Why it happens: a string can't pass through itself, so knots only start at a loose END. Confined, the string coils up, laying parallel strands beside the tip. Every jostle, the free end randomly weaves over and under them. Accidental braiding.
Floppy long lots of jostling = guaranteed tangle. (Flexible string knots 85%.)
How to beat it:
🔷keep cords short,
🔷coil them loose,
🔷pick stiffer over floppy, and
🔷don't leave them loose in a bag.
Tame the loose end, beat the knot.
#Science
#Physics
#Music
#Life
#Wisdom
Image courtsey: ChatGPT
1
2
102
Full paper:
Raymer DM, Smith DE. Spontaneous knotting of an agitated string. Proc Natl Acad Sci U S A. 2007;104(42):16432-16437. doi:10.1073/pnas.0611320104
1
87
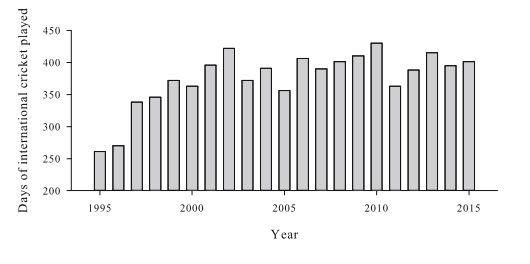
Nervous nineties in cricket: Is it really a thing?
For generations we have called it the nervous nineties. The bit where a batsman on 94 supposedly turns into a quivering mess, pokes, prods, and gifts his wicket five runs short of glory.
Four researchers in Melbourne decided to stop assuming and actually check. The data has a rude surprise for the commentary box.
What they did
No interviews. No vibes. They went to cricsheet, pulled ball-by-ball data from 712 test matches played between 2004 and 2022, and ended up with more than 1.4 million deliveries to chew on.
Then they zoomed in on every innings where a batter passed through somewhere between 70 and 130 runs. That left 366 players and nearly 1,400 centuries to study.
For every single ball they noted three simple things. How many runs came off it. Whether it went to the fence. Whether the batter got out.
They used a method called regression discontinuity. Forget the jargon. You park yourself right at the 100 line and ask one question. Does anything suddenly jump the moment a batter crosses it? If behaviour snaps exactly at 100 and nowhere else, then reaching the century is what caused the change. Same trick economists use on a pass mark. Compare the student who scored 39 with the one who scored 41 and you learn what the line itself does.
What they found
Turns out the nineties are when batters floor the accelerator.
Runs per ball climbed steadily on the way up, from about 0.59 at a score of 77 to 0.71 at 99.
Boundary chances rose right alongside, from roughly 6 percent to nearly 9 percent by the time they hit 99. The closer to the century, the harder and faster they went.
Then they reach 100. The brakes come on. Scoring drops, boundaries fall by about three percentage points, and the batter eases into a calmer rhythm.
And the wickets? The thing we are all so certain spikes in the nineties? Flat as the Chepauk pitch on day one. Around a 1.3 percent chance of getting out per ball before 100, at 100, and after 100. No spike. No carnage. The famous nervous collapse simply never shows up in the numbers.
Translation: most batters do not seize up at 95. They go chasing the finish line, get the job done, then relax once it is safe.
Why do we think about nervous 90's?
Most likely, it is because our emotional involvement in the game. We forget the 50 centuries Sachin scored successfully, and remember the one he missed.
Do you agree? @imVkohli @stevesmith49 @root66
@Cricketologist @bestcricstories
#Cricket
#Batting
#Century
1
1
4
519
Full paper here:
Roberts L, Little DR, Jackson M, Spittal MJ (2023) Test cricketers score quickly during the ‘nervous nineties’: Evidence from a regression discontinuity design. PLOS ONE 18(6): e0287700. doi.org/10.1371/journal.pone…
56
Everyone thinks fast bowlers break down because they bowl too much. Half right. The research says bowling too LITTLE injures them too.
A 2016 systematic review (McNamara, Gabbett, Naughton) went through the literature on what actually wrecks elite fast bowlers.
They started with 751 papers, threw out duplicates, pre-2005 studies, abstracts and anything not done on real bowlers in the field, and were left with 17 solid studies covering 984 players.
Caveat worth saying out loud: 82% of that research is Australian. So this is the gospel according to Cricket Australia's sports science department.
What they found is more interesting than "rest your bowlers."
The number that matters is not how much you bowl. It's how SUDDENLY you ramp it up.
Researchers split workload into two:
Acute load = what you bowled in the last 7 days (your fatigue)
Chronic load = your rolling 4-week average (your fitness)
When the acute spikes way above the chronic, the bowler gets hurt. Often in the week right after the spike. Sometimes the injury shows up 3 to 4 weeks later, which is why nobody connects the dots.
The bowler looks fine, plays two more games, then snaps a hamstring and everyone blames the hamstring.
Some hard thresholds from the data:
Bowl over 50 overs in a single match and your injury risk jumps for the next 21 days.
Bowl heavy in the second innings (over 30 overs) and per-over injury risk climbs over the following 28 days.
And here's the bit selectors hate: a bowler who has been UNDER-bowled is also fragile. A low chronic load means no built-up resilience, so the first proper spell becomes a spike.
This is why wrapping your strike bowler in cotton wool before a big series can backfire. You didn't protect him. You just made his comeback the most dangerous spell of his season.
The injury types even sort themselves by workload history:
Tendon injuries = high recent load on top of a high previous season
Bone stress (the dreaded lumbar fracture) = high medium-term load but LOW career load, basically a young bowler ramped up too fast
Joint injuries = the high-mileage veterans
Then T20 walked in (first international, 2005) and scrambled everything. GPS data showed T20 and one-dayers demand 50 to 100% more sprinting per hour than multi-day cricket. Higher intensity, lower volume, and the same bowler now switching between all three formats in a single month. Try building a clean chronic load through that.
Summary for cricket fans:
High volatility in fast bowlers' load has the potential to wreck their rhythm.
Resting them without a thought might add to the volatility.
Basically;
If you want to climb, control the angle of the ramp.
#Cricket
#Science
#Injuries
@bestcricstories @AMP86793444
Image courtsey:
McNamara DJ, Gabbett TJ, Naughton G. Assessment of Workload and its Effects on Performance and Injury in Elite Cricket Fast Bowlers. Sports Medicine. 2016;46(11):1525-1538. doi:10.1007/s40279-016-0588-8
1
3
235
May 31
Something to ponder on the No Tobacco Day.
Your dog might be anxious because you smoke. Not metaphorically. Measurably.
A study of 304 dogs in Tehran just put a number on something owners never think about: the dog is breathing your cigarette too. And its behaviour shows it.
Researchers split the dogs into two matched groups of 152, one living with smokers, one without.
Owners rated each dog's personality on a validated Persian translation of the Dog Personality Questionnaire (the DPQ, a real instrument, not a vibe check).
Cross-sectional, owner-reported, but properly powered and properly matched on age, sex, neutering.
The odds ratios are the story. Dogs in smoking homes showed:
Anxiety: OR 7.25
Trainability (worse): OR 3.42
Aggression toward other animals: OR 3.40
Reduced activity: OR 1.77
Fearfulness: OR 1.73
Aggression toward people: OR 1.68
That anxiety figure is not a typo. A sevenfold jump.
The mechanism is the interesting part. Nicotine and the cocktail in sidestream smoke aren't just lung irritants they're neuroactive. Chronic low-dose exposure activates the same stress machinery that governs threat response and arousal. A dog can't tell you it feels on edge. It just becomes harder to train, quicker to snap, slower to settle. The behaviour is the symptom report.
We talk about second hand smoking in people.
Let's not forget pets.
#notobaccoday
#31May
#MedTwitter
#PsychTwitter
#Animals
#pets
1
90
May 31
Full paper
Alaie M, Sheikhi Narani M, Jamshidi S, Tamimi NSM, Akbarein H. Behavioral changes in domestic dogs associated with exposure to secondhand smoke: a cross-sectional study. J Vet Behav. 2025
59
May 31
#GT did not bowl body-line against #VaibhavSooryavanshi.
1. They could bowl only 2 bouncers per over.
2. They can't place a ring of fielders around the leg side as Jardine had.
3. Vaibhav was not bound by a compulsion to play defensive cricket, as he is a modern batter, using a modern bat, and playing a T20 game.
Vaibhav is special, but, let's not discredit GT with baseless allegations.
#cricket
#science
#ipl
#gtvrr
1
220
May 30
Nothing but stone cold Australian professionalism.
Brilliant. Too bad it failed.
May 30

A forgettable and depressing match!
#OnThisDay in 1999, Australia, led by Steve Waugh, sparked one of the World Cup’s biggest controversies.
Chasing a modest target against West Indies at Old Trafford, Waugh crawled to 19 off 73 balls and Michael Bevan made 20 off 69 as Australia scored just 12 runs in the final 10 overs.
The deliberate slowdown was aimed at helping West Indies qualify ahead of New Zealand on net run rate, which would have allowed Australia to carry extra points into the Super Six stage.
The plan ultimately failed when New Zealand crushed Scotland in their next match, but the game remains one of the most debated tactical moves in World Cup history.
84
May 30
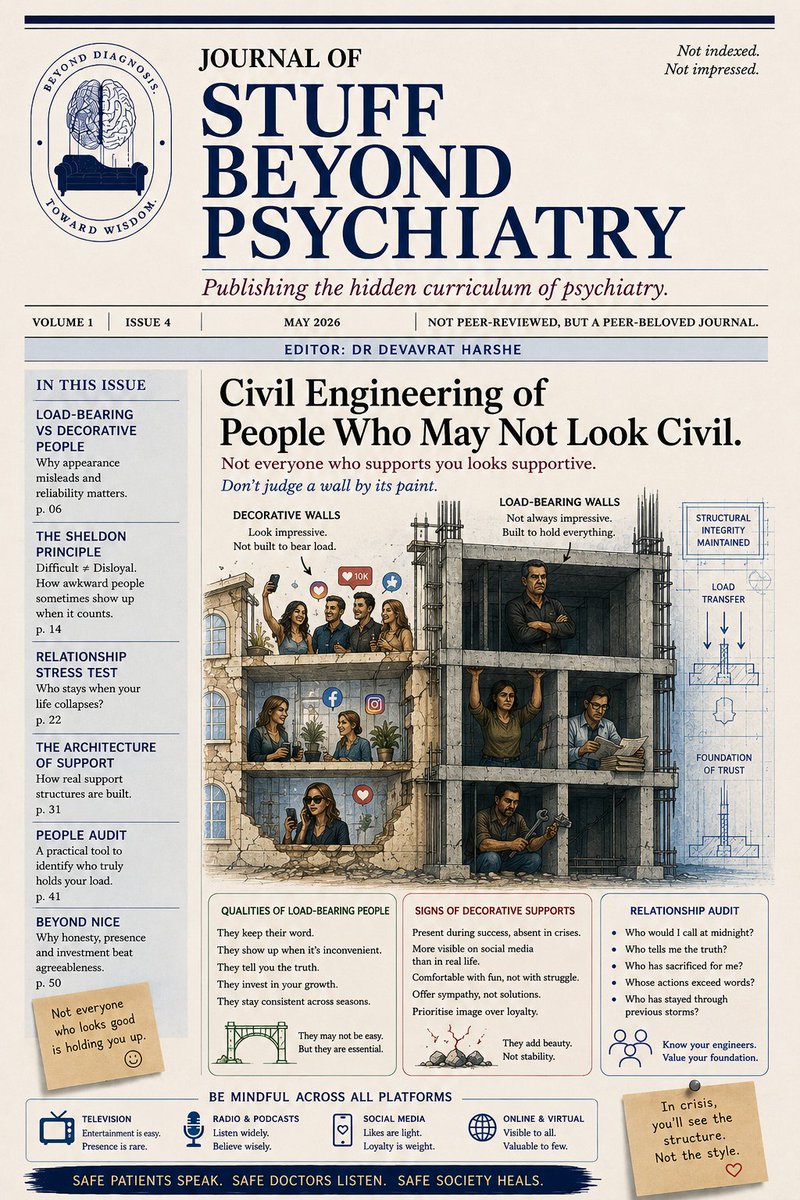
The #Journal of Stuff Beyond Psychiatry.
Vol. 1, No. 4. Skill: Civil Engineering
Every building has two kinds of walls, and from the inside they look exactly the same.
Which Supports Are Structural and Which Are Decorative
One holds the roof up. The other divides the room. Both get painted the same colour, hung with the same pictures, finished with the same skirting. Stand in the room and you cannot tell which is which.
The two walls
A load-bearing wall carries weight. Remove it and that load has nowhere to go. The structure sags, cracks, and eventually fails.
A partition wall carries nothing but itself. It exists to divide space and to look like a wall. It is genuinely useful. It gives you privacy and somewhere to hang a painting. But it holds up nothing. You can remove it on a whim and the house does not notice.
Here is the part that matters. You cannot tell them apart by appearance. The smoothness of the finish tells you nothing about the structure. The decorative wall is often the better looking one, precisely because it has no load to carry and can afford to be smooth.
The people version
People are the same. Some of the people around you are load-bearing. When the weight of your life goes up, illness, money, grief, a 2 a.m. crisis, they take some of it. Others are decorative. They are pleasant company, they make the room nicer, and when the load goes up they carry none of it. Not because they are bad. Because that was never their function.
And as with walls, you cannot sort them by how pleasant they are to stand next to. This is the error. People assume the agreeable ones are the supports and the difficult ones are dead weight. It is frequently the other way round.
Exhibit A:
Consider Sheldon Cooper.
By any reasonable social measure, Sheldon is a problem. He is rigid, condescending, and tone deaf. He keeps a schedule for the bathroom. He explains things nobody asked to have explained. To Penny, his neighbour, he is openly rude. He informs her that she is a failed waitress. He notes that the acting career is not happening. He keeps an itemised mental ledger of what she owes him. Spend an evening with him and you would call him a pain, and you would be correct.
However..
When Penny slips in her bathroom and dislocates her shoulder, alone and unable to move, it is Sheldon who comes. He hates germs. He hates disruption to his routine. He is visibly horrified by the entire situation. And he gets her dressed, drives her to the hospital, and stays. When she later needs to learn the material for a job she is not qualified for, he does the unglamorous, accurate work of actually teaching it to her. He shows up. He tells her true things she does not want to hear. He carries weight.
Sheldon is a load-bearing wall. Rough finish. Scrapes your knuckles when you pass. Does not move when you want it to move. And it is holding up the roof.
Blunt is not toxic
This brings us to the distinction that the word "toxic" has nearly destroyed.
Blunt is not toxic. A pain is not toxic. Honest is not toxic.
Toxic has a specific meaning, and the meaning is structural. A toxic person does not merely fail to carry your weight. They transfer their weight onto you. They extract. They distort your information so that you make worse decisions. They are warm when it costs them nothing and absent the moment a load appears. Toxic is a partition wall that has somehow also started rotting the foundation.
Sheldon is none of that. When he calls Penny a failed waitress, the information is accurate, it is offered in the open, and the cruelty buys him nothing. It is tactlessness, not extraction. So the test is not "did it sting." Structural walls scrape you constantly. The test is the direction of the weight. Is this person taking load off you, or loading you up?
How to find the load-bearing walls
Three questions, then, to find the supports and to stop mistaking them for the decoration.
First, what happens under load. Not on a good day. On the worst day. Decorative walls are wonderful on good days, which is exactly why they fool you. You learn a wall's job only when you put your whole weight on it.
Second, which way the weight is moving. A blunt friend hands you accurate, uncomfortable information and leaves you stronger than they found you. A toxic one hands you their moods, their problems, and their version of reality, and leaves you carrying more than you arrived with.
Third, what it costs them to show up. The decorative person gives you what is free: agreement, flattery, easy company. The load-bearing person gives you what is expensive: time, honesty, the hospital run at an hour that wrecks their week.
Two warnings
Do not knock out load-bearing walls because they are unpleasant. The fashionable advice is to remove anyone who causes discomfort and keep the company that soothes.
And the opposite warning, which matters just as much. Bluntness is not a permit. Not every unpleasant person is a secret pillar. Some difficult people are simply difficult and also carry nothing, abrasive and decorative at the same time. And some genuinely toxic people will tell you they are "just being honest" right up to the moment they extract. You still have to check the load path. Honesty, plus reliability, plus a cost paid to show up. All three.
Cruelty on its own is just cruelty.
Why this is our business
For us in psychiatry the application runs two ways.
Patients arrive mid-renovation. They are worn out by the blunt parent, the demanding mentor, the friend who keeps saying the hard thing, and they are being told from every direction to cut these people loose.
Part of our job is to help them check the structure before they swing the hammer.
The other part, equally, is to help them name the genuinely toxic relationships. The skill is the distinction. It is never a blanket rule in either direction.
Find the people who hold weight. Forgive them their finish.
@psychidiaries
This is the recent version. Will share the last week's one now.
#MedTwitter
#PsychTwitter
1
3
8
1,127
May 28
खारी है ईमान मेरा खार मेरी जिंदगी.


2
50
May 27
A cricket helmet passes British safety standards by being dropped 2 metres onto an anvil. Impact velocity at contact: ~23 km/h.
#Bumrah bowls at 145.
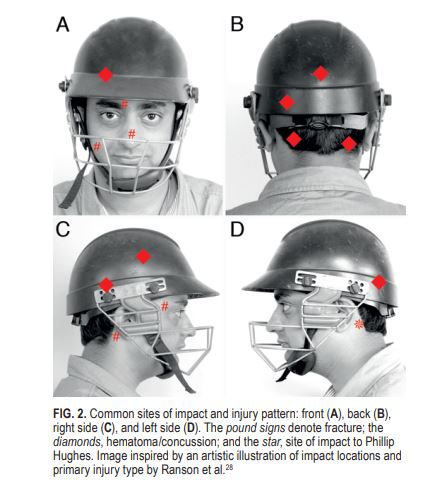
A 2016 NIMHANS neurosurgery paper went through 145 years of professional cricket — from George Summers in 1870 to Phillip Hughes in 2014 and catalogued every head injury they could find.
36 incidents. 5 dead. 9 careers ended.
86% of the damage lands on batters. More than half were a ball straight to the head. In nearly 1 in 5, the ball squeezed through the peak-faceguard gap.
British Standards mandates that gap be ≤55mm. The ball is 73mm. The 18mm "safety margin" keeps failing — the ball deforms on impact, the grill bends inward,what worked in the lab fails on the pitch.
The quieter story is wicketkeeping. Three career-ending eye injuries — Mark Boucher, Saba Karim, Paul Downton. None of them from the ball. All from the bail. You cannot watch both at once, especially against a spinner.
Despite the gap between the peak and the grill being smaller than the ball, we often see, the ball getting lodged between them by breeching the grill.
After Phillip Huges and Steve Smith got hit by bouncers helmets were redesigned and the temple grill was extended to the back of the neck.
When the authors finally swapped the drop test for an air cannon firing real balls at real speeds, cricket helmets attenuated 80% of the impact at slow velocity and only 40% at fast-bowler velocity.
Helmets are getting built for safety. Key question: What speed are they being tested at?
#Cricket
#HeadInjury
#Helmets
@AMP86793444 @bestcricstories
Image courtsey:
1. Tripathi M, Shukla DP, Bhat DI, Bhagavatula ID, Mishra T. Craniofacial injuries in professional cricket: no more a red herring. Neurosurg Focus. 2016 Apr;40(4):E11. doi: 10.3171/2016.2.FOCUS15341. PMID: 27032914.
2. Cricinfo.
1
4
18
4,401
May 27
Full paper.
Tripathi M, Shukla DP, Bhat DI, Bhagavatula ID, Mishra T. Craniofacial injuries in professional cricket: no more a red herring. Neurosurg Focus. 2016 Apr;40(4):E11. doi: 10.3171/2016.2.FOCUS15341. PMID: 27032914.
217