
Joined February 2021
- Tweets 9,476
- Following 2,896
- Followers 30,605
- Likes 21,201
4,769 Photos and videos
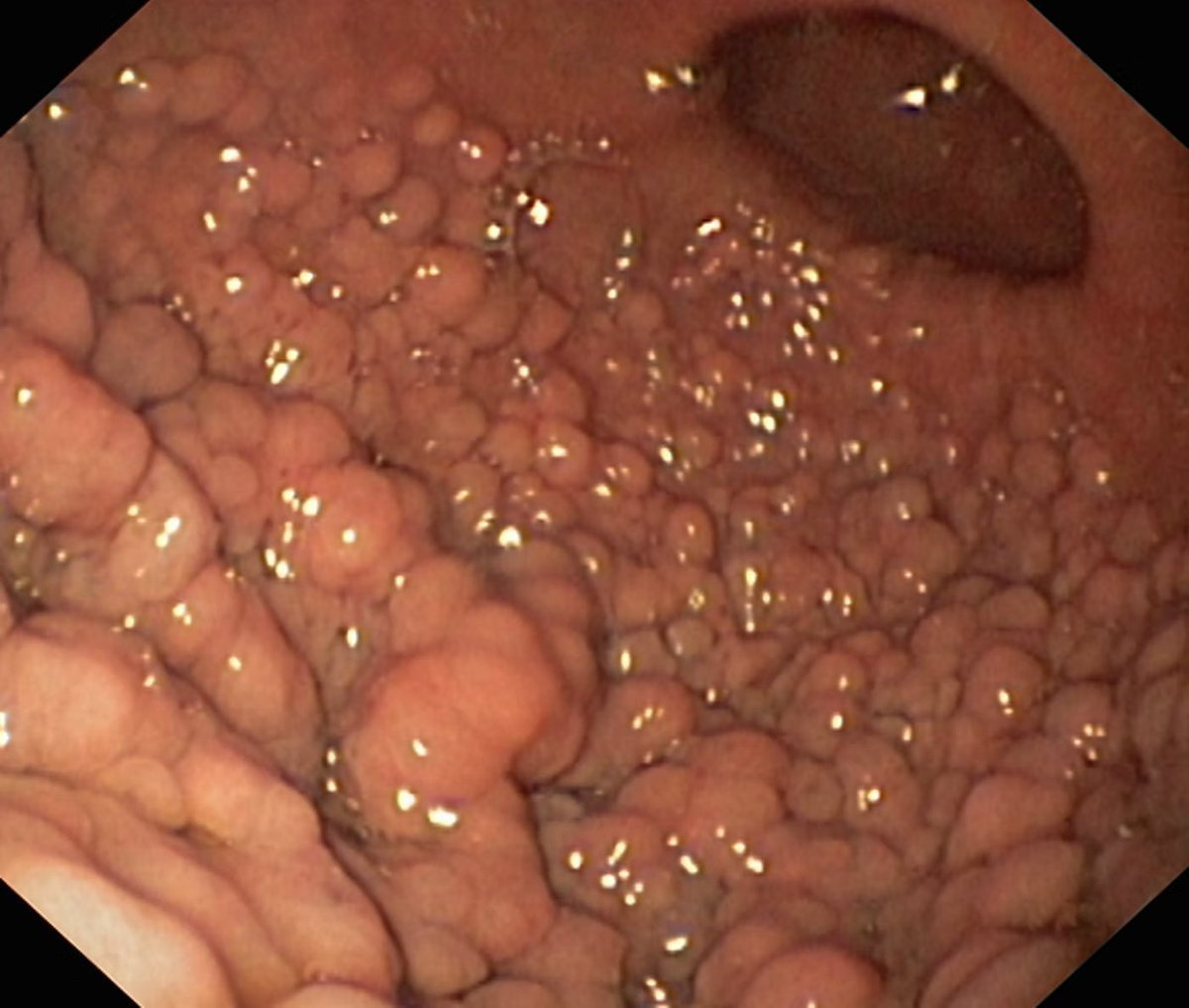




Stomach Photo Quiz
What is your diagnosis? Would you also perform a colonoscopy on this patient?
If so, why?
1
409
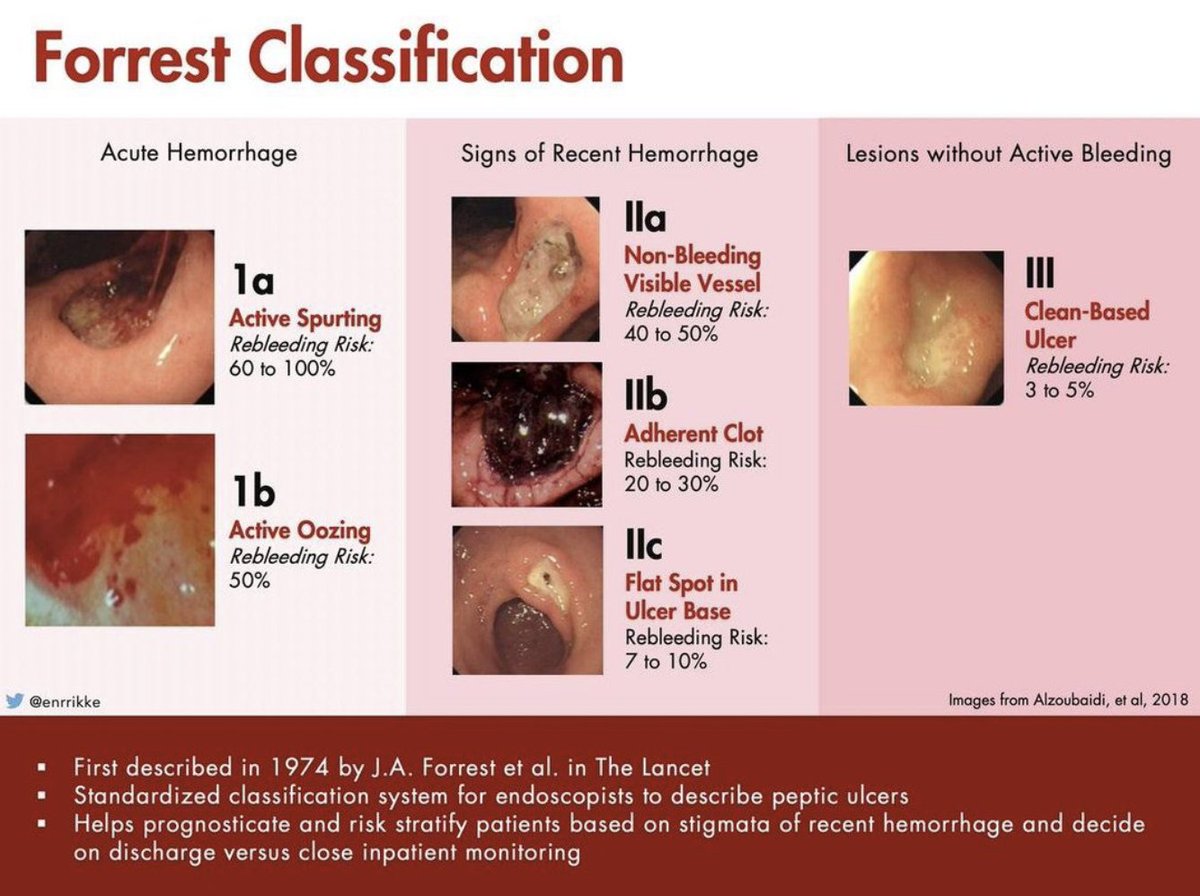
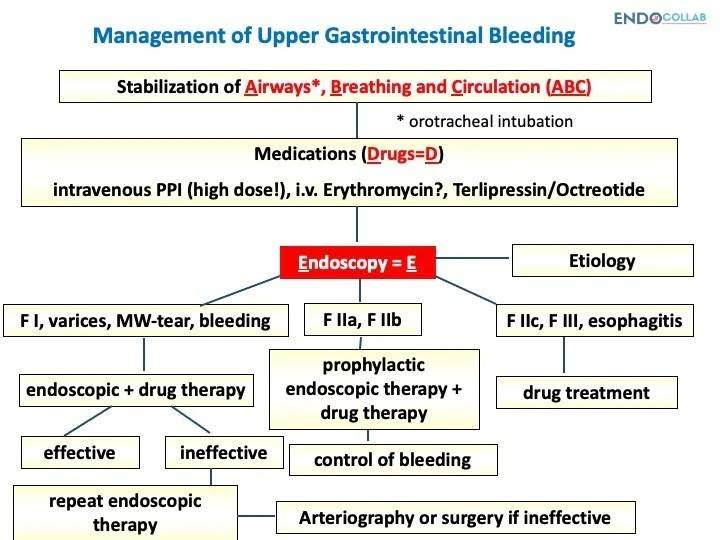
Applying the Forrest classification for peptic ulcer bleeding helps guide endoscopic therapy and predict rebleeding risk.
Peptic ulcer bleeding classifications:
- Type Ia: Active spurting bleeding.
- Type Ib: Active oozing bleeding.
- Type IIa: Visible non-bleeding vessel.
- Type IIb: Adherent clot.
- Type IIc: Flat pigmented spot.
- Type III: Clean-based ulcer.
Which ulcer stages do you routinely treat?
2
2
206
3 endoscopic findings in dabigatran-induced exfoliative esophagitis:
1. Sloughing of the esophageal mucosa, often described as a cast-like appearance.
2. Circular or longitudinal peeling of the mucosal layer.
3. Sparing of the gastric mucosa, which distinguishes drug-induced damage from caustic injury.
Review the case reports and endoscopic images below ⬇
1
5
4
1,277
Read the full article and see the endoscopic spectrum:
endocollab.com/blogs/gi-endo…
2
743
New: Endoscopic Balloon Dilation of a Benign Duodenal Stenosis
thepracticingendoscopist.com…
2
612
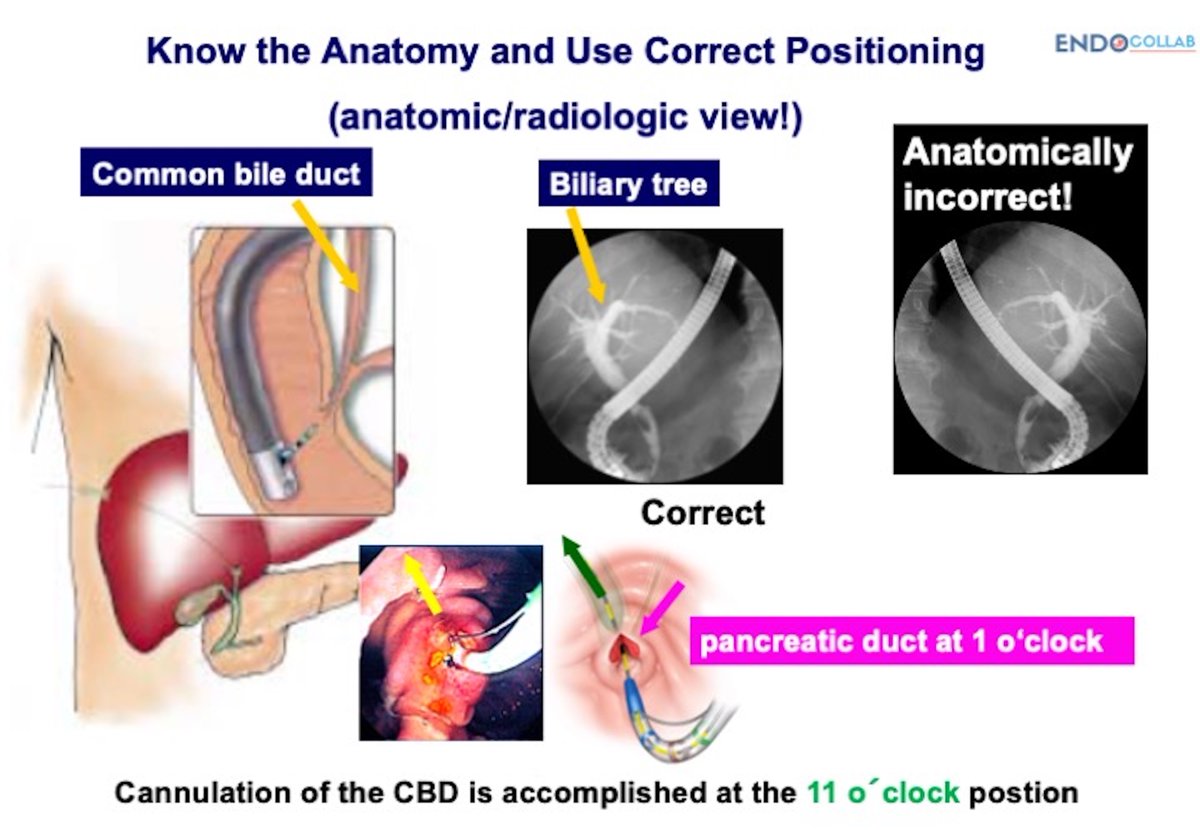
Cannulation during ERCP reveals two separate openings at the papilla.
Two possibilities to distinguish:
1. A natural anatomic variation with separate biliary and pancreatic orifices.
2. Biliary-enteric fistula caused by prior stone passage or instrumentation.
How do you confirm the anatomy before passing your guidewire?
1
3
16
2,649
3 points on using hemostatic powders in gastrointestinal bleeding:
1. Keep the catheter tip 1 to 2 cm away from the bleeding source to prevent occlusion.
2. Clear the endoscope channel with a puff of air before inserting the catheter.
3. Use hemostatic powder as salvage therapy or when the bleeding site is too large for mechanical clips.
Review the complete clinical review below ⬇
1
2
7
866
Read the full guide on hemostatic powder application:
endocollab.com/blogs/course-…
3
468
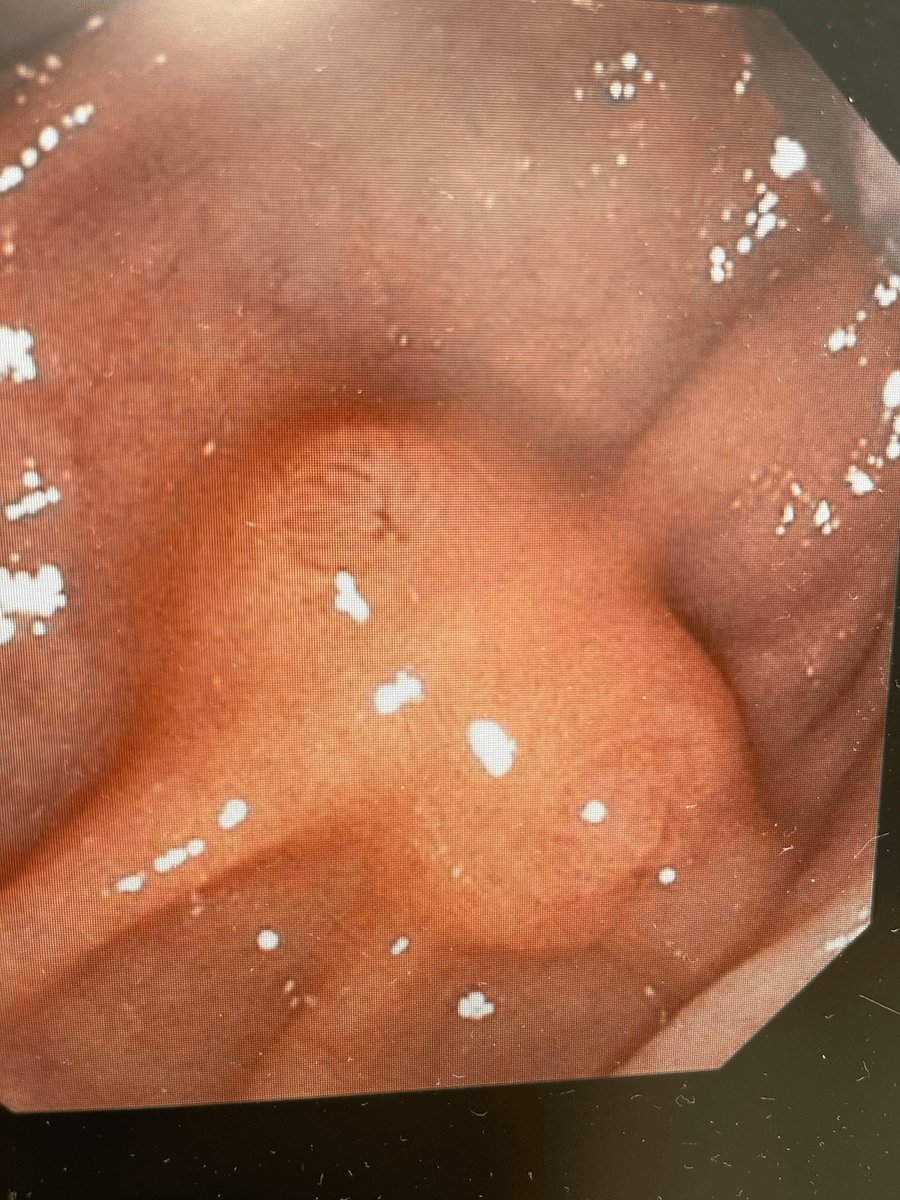
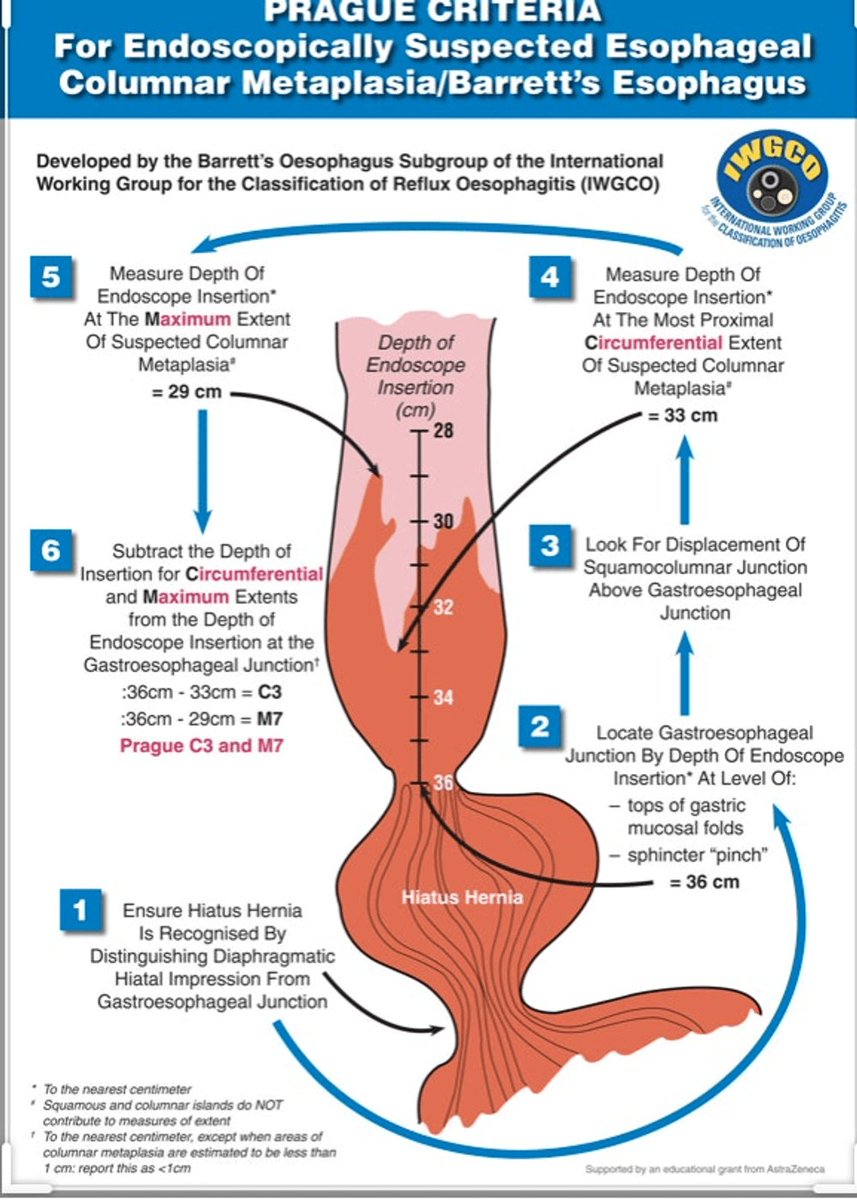
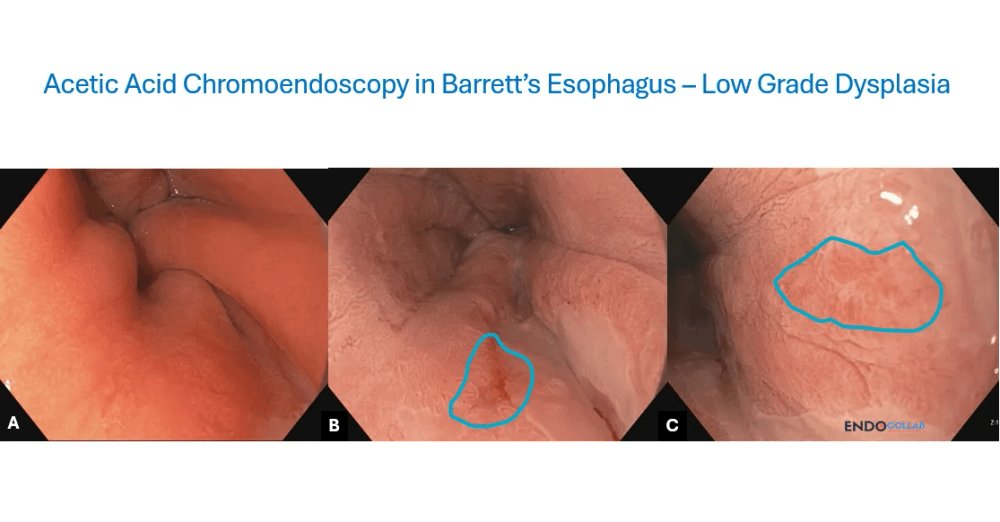
Applying the Prague classification for Barrett's esophagus requires finding the exact gastroesophageal junction (GEJ).
How to locate the GEJ:
- Find the proximal margin of the gastric folds.
- Deflate the esophagus partially to see where the folds settle.
- Do not use the palisade vessels as the primary landmark when active esophagitis is present.
Note: Measuring the C (circumferential) and M (maximal) extent starts from this GEJ level.
6
11
668
EndoCollab™ | GI Endoscopy Community retweeted

After 2.5% acetic acid, target Barrett red zones with loss of aceto-whitening.
thepracticingendoscopist.com…
1
2
568
3 tips for clipping Mallory-Weiss tears:
1. Deploy the first clip at the distal margin of the tear to secure anchor position.
2. Use a distal attachment cap on the endoscope to maintain clear visualization of the bleeding point.
3. Apply suction to draw the tissue into the cap before releasing the clip if bleeding is active.
More technical details on clipping techniques below ⬇
1
4
12
2,350
Read the full technical review and watch the procedure steps:
endocollab.com/blogs/gi-endo…
2
4
817
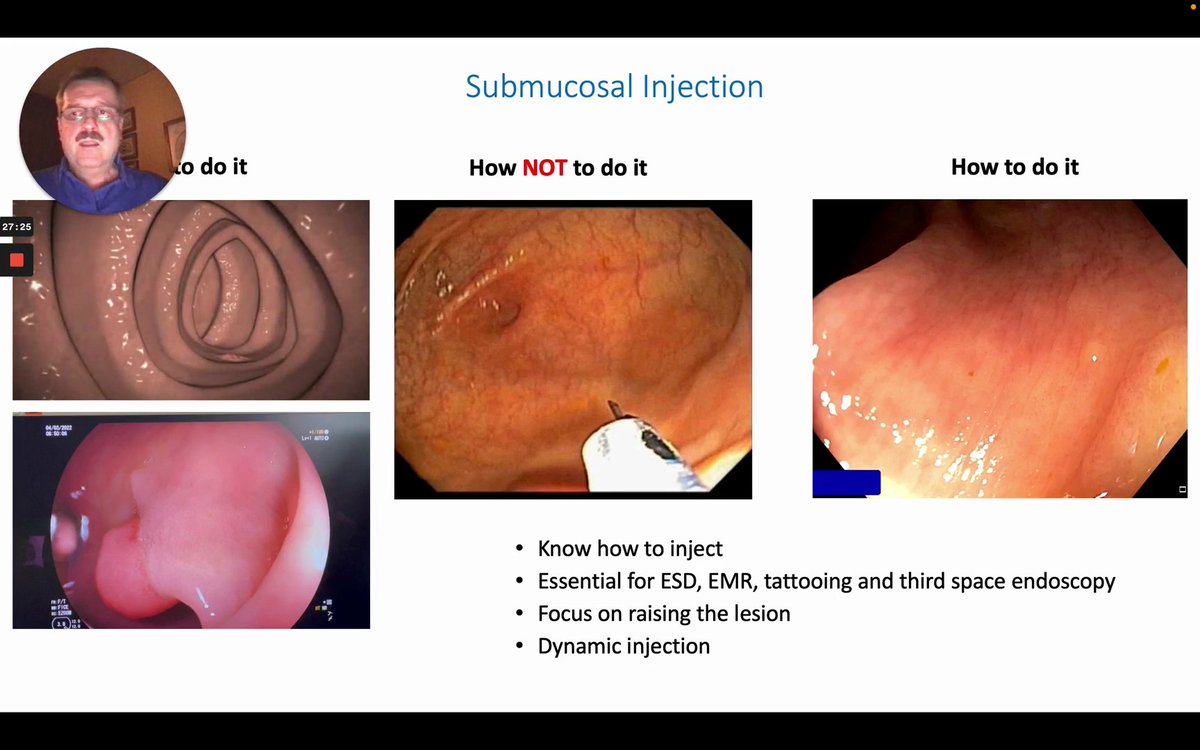
How to Create the “Blue Dye” for the Submucosal Cushion
endocollab.com/blogs/lecture…
1
1
523
When should you switch to cap-assisted technique for difficult scope navigation?
Employing a high-flow water jet and stent combination facilitates safe debris removal and hemostasis, significantly reducing procedural complications.
3
7
1,059
Know the Anatomy and Use Correct Positioning
ALT Know the Anatomy and Use Correct Positioning
7
19
1,602
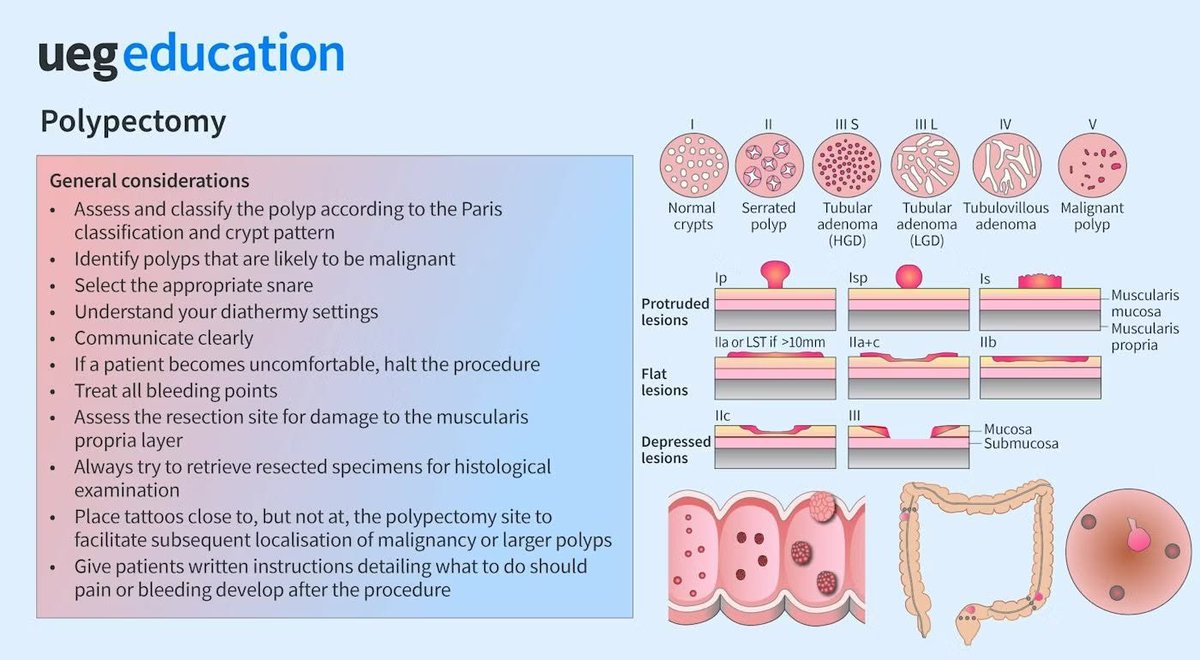
Tips for Colon Polypectomy
I would also add: have clips and injector needles available, know how to perform a submucosal cushion, do not perform polypectomy in dirty colon
28
71
3,159
EndoCollab™ | GI Endoscopy Community retweeted
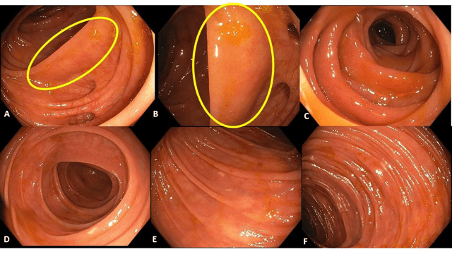
80-year-old patient with ongoing watery diarrhea for several weeks.
Read the full case: thepracticingendoscopist.com…
1
4
17
3,059
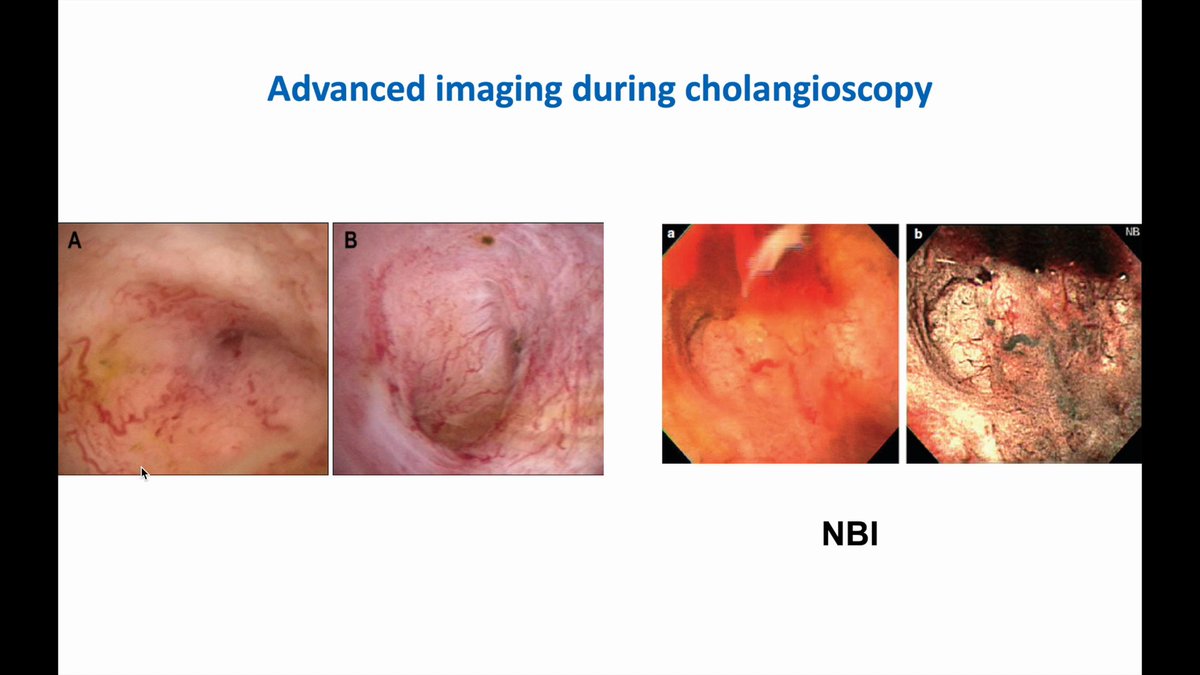
Advanced imaging during cholangioscopy
4
10
947
EndoCollab™ | GI Endoscopy Community retweeted
Persistent or worsening symptoms in celiac disease should raise concern for complicated disease, including EATL (lymphoma), adenocarcinoma, or ulcerative enteritis.
Read the full case: thepracticingendoscopist.com…

6
8
993
Submucosal Injection
• How to do it
• How NOT to do it
2
12
1,886