
Driving research on fluoroquinolone's mechanism of damage to develop diagnostic and therapeutic solutions to create change for the affected global community.
Joined February 2018
- Tweets 788
- Following 79
- Followers 772
- Likes 369
356 Photos and videos








Pinned Tweet

16 Aug 2025
Serious systemic adverse effects (beyond package side effects) from #fluoroquinolone (#Cipro/#ciprofloxacin, Levaquin (off market)/#levofloxacin, Avelox/#moxifloxacin etc) antibiotics may persist for extended periods, potentially lasting for years or indefinitely for some.
In 2016 and 2018, the FDA advised that fluoroquinolones should only be used in cases where no other options are available for sinusitis, bronchitis, or uncomplicated UTIs. They contain multiple Black Box warnings,* the most serious warnings a medication can have.
If you are experiencing any or all of these symptoms below and are stunned by the ongoing emergence of new and troublesome issues following the antibiotic treatment you underwent, you have been what is deemed 'floxed':
✅ Extreme weakness, inability to stand or walk as before prescription
✅ Nerve problems — weakness, numbness, pain, muscle jerking and twitching, crawling bug feeling
✅ Tendon tears and muscle weakness
✅ Collagen destruction, hanging skin, wounds slow to heal
✅ Acute sensitivity to sunlight, sudden hormone & thyroid issues
✅ Ringing in the ears, vision disturbances
✅ Anxiety, panic attacks, disorientation, impaired concentration or memory, confusion, depersonalization, hallucinations, psychoses
Due to the potential of mitochondria** dysfunction, the actual list of adverse effects can be quite lengthy. Every prescription drug has side effects, some worse than others. Please do your research before you take that next pill, ear drop or eye drop, ask for a substitute if needed - don't let yourself become a statistic.
🟠 🟡 🟢 🔵 🟣 ⚫ 🟤
*Black Box warnings: fq100.org/fda-warnings
**Mitochondria are the powerhouse of your cells
➥Listen to our 3 part series with Dr. Stefan Pieper: YouTube channel: youtube.com/@FqAntibioticDam…
💊Medications in the fluoroquinolone class (incl: Cipro/ciprofloxacin, Levaquin (off market)/levofloxacin, Avelox/moxifloxacin etc) in all forms for humans and pets: fq100.org/drug-list
Find support and resources on our sites:
🌐 Medical resources: fq100.org/find-medical
🧭 Help & Misc resources: fq100.org/find-help
▶️ YouTube: youtube.com/@FqAntibioticDam…
🐦 X/Twitter: twitter.com/FQ_100
#FQAwareness #Fluoroquinolones #MitochondrialHealth #AntibioticSideEffects #Floxed #Cipro #Levaquin #FQAD
⚠️Disclaimer: Fluoroquinolone Toxicity Study does not provide medical advice, and all articles and written content are intended for informational purposes only. We do our best to provide accurate information. Such information is not a substitute for professional medical advice, diagnosis or treatment. For multiple reasons, supplements, treatments, and pharmaceutical effects and outcomes can possibly vary significantly among those affected by fluoroquinolone drugs.

4
11
34
3,191
We have some resources for you ✏️
Dealing with fluoroquinolone antibiotic adverse effects and an upcoming doctor appointment? Feeling isolated and lost? We want you to feel a little more prepared and a little less alone.
Last year when the code came out, we put some supportive tools in one place on our website so you do not have to reinvent the wheel on a day when your body and brain may already be doing a lot.
🟣A printable ICD-10 code sheet you can bring with you
ICD-10 simply means the standardized diagnosis and billing codes used in medical records and by insurance. As of October 1, 2025, fluoroquinolone adverse effects/toxicity have their own ICD-10 code category. That can make it easier for a clinician to document your reaction accurately and consistently.
➦Check out the code list, included FDA warnings and Black Box timeline to print and take with you in the downloads section.
🟣Asking for the Code
Some possible helpful guidance on how to ask your doctor to enter the code into your medical record
➦Check out this document in the downloads section.
🟣The Adverse Effects Evaluation Form
Many people tell us the hardest part of an appointment is remembering everything their body is experiencing, especially adverse effects that are ever-changing and piling up. This downloadable form helps you check-off what you have experienced, when it started, and what changed over time, so you can walk in with a clear snapshot of top complaints.
➦Check out this form in the downloads section.
🟣Medical care
If you are looking for a clinician who may be more open to documenting complex reactions, our Find Medical page gives some options.
➦Check out our Dear Doctor letters in the downloads section on the Find Help page in addition; another document that may help support your visit
🟣Support in the community
Seek comfort in a like-minded community via our Find Support page reflecting groups in multiple countries. Even one kind conversation with someone who gets it can make a tough day feel a bit lighter, despite the huge challenges we are all facing.
➦See the support group page link below
➤ ➤ ➤ ➤ ➤ ➤ Start here❗ (best first step & for downloads): fq100.org/find-help
🌈🌈🌈If you already took the code information to an appointment, please share how it went in the comment section below. Feedback can help others, determine if we need to add more to references, and get an idea of what hurdles floxies are still facing at appointments.
🟣🟣🟣🟣🟣🟣🟣🟣🟣🟣🟣🟣🟣
Find Medical: fq100.org/find-medical
Find Support: fq100.org/find-support
💊Medications in the fluoroquinolone class (incl: Cipro/ciprofloxacin, Levaquin (off market)/levofloxacin, Avelox/moxifloxacin etc) in all forms for humans and pets: fq100.org/drug-list
Looking for more info? Check out our past Facebook posts and our YouTube channel: ▶️: youtube.com/@FqAntibioticDam…
#Fluoroquinolones #FQAD #FQToxicity #Mitochondria #Neuropathy #AntibioticSideEffects #Cipro #Levofloxacin
22
For decades, fluoroquinolone antibiotic injured patients have reported tendon pain, weakness, tearing, ruptures, instability, and a frightening sense that their connective tissue no longer has the same strength or support. This new unedited* study: "Effects of fluoroquinolone antibiotics on extracellular matrix-related phenotypes in tendon cells", adds another important piece to that puzzle.
Rather than looking only at tendon pain or rupture risk, the researchers examined what fluoroquinolone antibiotics may be doing inside tendon cells and to the extracellular matrix, or ECM. The ECM is the body’s structural support system around cells. In tendons, this matters enormously because tendon strength depends on a highly organized collagen matrix. When that matrix is disrupted, the issue may not simply be “less collagen,” but weaker, poorly assembled connective tissue.
The authors focused mainly on ciprofloxacin and levofloxacin using adult mouse Achilles tendon cells. Their central finding was that fluoroquinolones did more than reduce collagen production. They also disrupted several key parts of tendon matrix health, including collagen assembly and quality, collagen fibril stiffness, fibronectin, lysyl oxidase activity, and active β1-integrin, an important receptor that helps cells attach to and communicate with the surrounding matrix.
This suggests that fluoroquinolones may weaken tendon structure by disturbing both:
➥ ➥ the “building materials” and the “assembly system.”
What they found --
🟡 Ciprofloxacin enters tendon cells through a carrier-mediated process. That means it is not just passively floating around outside the cells; tendon cells appear able to take it up through transport systems. The authors say this was shown in tendon cells for the first time, although they also admit the transporter they identified does not explain all uptake.
🟡 Reduced type I collagen (the major tendon collagen) ➨Levofloxacin and ciprofloxacin reduced type I collagen mRNA and protein, with ciprofloxacin appearing stronger in this model.
🟡 Reduced fibronectin (fibronectin helps organize collagen matrix and supports cell adhesion).
🟡 Increased type V collagen ➨type V collagen helps regulate collagen fibril diameter. The authors suggest that a shift in the type V/type I collagen balance could contribute to thinner or altered collagen fibrils.
🟡 Collagen assembly was strongly inhibited. The collagen network was much more affected than total hydroxyproline content, suggesting the issue is not only “less collagen,” but poorly organized collagen matrix.
🟡 Reduced hydroxyproline content (a marker of collagen content and collagen-related ECM).
🟡 Reduced lysyl oxidase activity. (Lysyl oxidase (LOX) helps cross-link collagen and elastin and what gives connective tissue strength).
🟡 Ciprofloxacin reduced collagen fibril elastic modulus by about 67% and fibril diameter by about 45% in vitro (cell culture), a concrete “structure/strength” finding.
🟡 Reduced active β1-integrin. This matters because β1-integrin helps cells attach to and sense the ECM. The authors speculate that impaired fibronectin and β1-integrin signaling could contribute to anoikis (form of cell death/dysfunction related to poor cell-matrix attachment).
What is new?
The most useful newer contribution is not that fluoroquinolones damage collagen - that was already known but:
1. Tendon-cell uptake of ciprofloxacin
They specifically show carrier-mediated ciprofloxacin uptake in mouse tendon cells. That gives a plausible reason tendon cells themselves may be directly affected, not only indirectly harmed by inflammation or systemic oxidative stress.
2. Collagen assembly versus collagen amount
Importantly, they show the collagen network/assembly can be severely impaired even when total collagen marker reduction is more modest. That helps explain why tissue could be functionally weak even if a simple collagen quantity marker does not look catastrophic.
3. LOX and fibril stiffness
The LOX/collagen fibril stiffness finding is meaningful because it connects FQ exposure to mechanical properties, not just molecular markers, and a 67% reduction in elastic modulus (the collagen structure became less firm and less mechanically strong).
❓The key question…..
How do we help the body rebuild and remodel matrix over time, while avoiding further injury and supporting the cellular systems that create usable collagen?
Evidence from tendon biology and tendinopathy research supports the importance of adequate protein, vitamin C, collagen-building nutrients, mineral cofactors, and progressive tendon loading for connective-tissue remodeling. However, this information comes largely from the general tendon-repair literature, not from studies specifically designed around fluoroquinolone-injured patients. Individuals with FQAD (fluoroquinolone associated disability) may not respond in the same way as the general population, and some may be unable to tolerate standard rehabilitation, treatments or supplement approaches, especially during periods of acute or systemic dysfunction. This is why this new tendon-cell paper is important as its findings point to a broader problem than just collagen.
This unedited study suggests fluoroquinolones may impair collagen production, collagen assembly, LOX activity, fibril strength, collagen balance, fibronectin, and β1-integrin/cell-matrix signaling. Therefore, a rational recovery framework may need to look beyond simply taking collagen and instead consider the larger matrix-repair environment. According to studies, potential support areas may include adequate protein, collagen peptides or collagen-rich foods to provide collagen-building amino acids, vitamin C sufficiency, copper/zinc balance for LOX-related cross-linking, correction of nutritional deficiencies, oxidative-stress and mitochondrial support, careful progressive mechanical loading, and avoidance of overload while the matrix is structurally vulnerable. Dedicated human studies in fluoroquinolone-injured patients are urgently needed to better understand these mechanisms and identify meaningful paths toward recovery.
Currently, much of the feedback regarding what helps or can worsen adverse effects such as tendon issues, still comes from patient experiences within the fluoroquinolone-injured community, with varying outcomes remaining very individual. Several additional clinician-supervised or experimental areas sometimes discussed in tendon repair include shockwave therapy, PRP, hyaluronic-acid/proteoglycan support, and regenerative peptides such as BPC-157 or thymosin β4/TB-500 (not currently FDA approved). Please always do your research and consult with a physician in functional medicine or similar before embarking on any treatments, keeping in perspective that many of those living with fluoroquinolone adverse effects can be living with fragile systems which many doctors are completely unaware of.
Should there be any changes to the early-access journal article once published, this post will be updated.
⚠️⚠️Disclaimer: This article is for educational and informational purposes only. It is not medical advice, does not provide a diagnosis or treatment plan, and should not be used as a substitute for care from a qualified healthcare professional. Fluoroquinolone-associated injury can involve complex, individualized risks. Some interventions, including supplements, exercise, physical therapy, medications, treatments and dietary changes, may be inappropriate or harmful for certain individuals based on many factors. Patients should consult their own healthcare professionals before making changes or starting new protocols.
⚠️Note: products such as collagen, bone broth and gelatin are animal derived and source quality can vary.
*✏️Article link:
Anand A, Sakai K, Dickens D, et al. Effects of fluoroquinolone antibiotics on extracellular matrix-related phenotypes in tendon cells. Scientific Reports. 2026. doi.org/10.1038/s41598-026-5… [Important Note: This is an unedited early-access version that may undergo further editing before final publication – see the download button for full article]
References
1. Anand A, Sakai K, Dickens D, Tsuzuki S, Minamiguchi S, Asai N, Kazaili A, Akhtar R, Pirmohamed M, Sakai T. Effects of fluoroquinolone antibiotics on extracellular matrix-related phenotypes in tendon cells. Scientific Reports. 2026.
nature.com/articles/s41598-0…
2. Buchalski A, et al. Collagen Supplementation on Tendon-Related Structural, Functional, and Clinical Outcomes: A Systematic Review. Journal of Functional Morphology and Kinesiology. 2026;11(1):130.
mdpi.com/2411-5142/11/1/130
3. Hijlkema A, Roozenboom C, Mensink M, Zwerver J. The impact of nutrition on tendon health and tendinopathy: a systematic review. Journal of the International Society of Sports Nutrition. 2022;19(1):474-504.
pmc.ncbi.nlm.nih.gov/article…
4. Kjaer M, Langberg H, Heinemeier K, et al. From mechanical loading to collagen synthesis, structural changes and function in human tendon. Scandinavian Journal of Medicine & Science in Sports. 2009;19(4):500-510.
paulogentil.com/pdf/From m…
5. Mousavizadeh R, Hojabrpour P, Eltit F, et al. β1 integrin, ILK and mTOR regulate collagen synthesis in mechanically loaded tendon cells. Scientific Reports. 2020;10:12644.
nature.com/articles/s41598-0…
6. Ellingson AJ, Pancheri NM, Eberman LE, Kines KJ, Recker AJ, Bates NA. Regulators of collagen crosslinking in developing and adult tendon. Journal of Orthopaedic Research. 2022;40(8):1821-1834.
pmc.ncbi.nlm.nih.gov/article…
7. Nguyen PK, Briquez PS, Kyoung J, et al. Tendon mechanical properties are enhanced via recombinant lysyl oxidase treatment. Scientific Reports. 2022;12:13624.
pmc.ncbi.nlm.nih.gov/article…
1
4
8
449
Even though this journal study in the link is not in its possible final version, it could be a good paper to print and take with you to tendon related appointments.
24
IMPORTANT:
🌀More comments needed! Please take 2 minutes.....
☑️The FDA is accepting public comments on the Fluoroquinolone* Citizen Petition
Johanna Ihli (affected patient & advocate) has filed a Citizen Petition on behalf of the vast global community affected by these antibiotics. Please support this effort and take a few minutes and sign using the link below. If you don't partake, then your voice is not counting.....
This petition asks the FDA to implement patient informed consent and improve public awareness concerning mitochondrial dysfunction from fluoroquinolone antibiotics, including medications such as Cipro (ciprofloxacin), levofloxacin, Avelox (moxifloxacin), and others (see drug list link below)
Fluoroquinolones already carry FDA boxed warnings for serious adverse effects, including tendon rupture, peripheral neuropathy, central nervous system effects, and disabling, potentially long-lasting multisystem reactions. Many patients report delayed or progressive symptoms that are difficult to diagnose, document, and connect back to the medication exposure.
Public comments matter❗
Patients, caregivers, family members, from any country can all submit comments and show the real-world impact of these medications.
✔ Directions!
➥Click link below
➥ Make your comment
Comments may include:
What medication was taken and why
When symptoms began, including any delayed onset
Tendon, nerve, neurological, psychiatric, autonomic, cardiac, connective tissue, or multisystem effects
Difficulty getting diagnosis, recognition, documentation, or treatment
Impact on work, mobility, family life, daily function, or quality of life
Why stronger informed consent and clearer warnings are needed
➥Comment Category - 'Individual Consumer" is what has been suggested
Important:
Every comment becomes part of the official FDA record and can help warn patients, encourage more appropriate limits on the use of fluoroquinolone medications, and remind doctors that these antibiotics can have serious medical implications beyond what many recognize from package inserts or the often-overlooked black box warnings.
✏️SIGN HERE: regulations.gov/commenton/FD…
Please share in FQ community support groups
*💊List of these antibiotics in all forms for humans and pets: fq100.org/drug-list
2
1
4
133
We are stronger together when we all use our voice.
1
42
Mitochondria 101 for Fluoroquinolone Associated Disability
✏️Fluoroquinolone Associated Disability (FQAD)
This is an FDA term whose definition is: A constellation of disabling symptoms in two or more body systems lasting 30 days or longer after the prescription* is finished.
To see the complete definition and indicated body systems, please visit: fq100.org/fda-warnings
Watch this video here: youtube.com/watch?v=v7mYIiPH…
*💊Medications in the fluoroquinolone class (incl: Cipro/ciprofloxacin, Levaquin (off market)/levofloxacin, Avelox/moxifloxacin etc) in all forms for humans and pets: fq100.org/drug-list
Find support and resources on our sites:
🌐 Website & Resources: fq100.org/
▶️ YouTube: youtube.com/@FqAntibioticDam…
🔵 Facebook: facebook.com/fqtoxicitystudy…
🐦 X/Twitter: twitter.com/FQ_100
#Fluoroquinolones #FQAD #FQToxicity #Mitochondria #Neuropathy #AntibioticSideEffects #Cipro #Levofloxacin
4
7
430
Have you ever felt like your body’s thermostat stopped working after fluoroquinolone antibiotics?
After fluoroquinolone injury, temperature regulation can feel unstable. Heat, cold, sun, saunas, air conditioning, or cold water can affect the body much more intensely than they used to. Instead of adjusting normally, the body may struggle to find its way back to a comfortable baseline after becoming too hot or too cold.
Fluoroquinolone* antibiotics have been linked in scientific literature to mitochondrial stress, oxidative stress, and nervous system adverse effects. These effects may help explain why temperature regulation can feel so disrupted for some people. Hot weather, direct sun, saunas, strong air conditioning, cold weather, cold water, or being chilled for too long can trigger or worsen symptoms in different ways.
So why might this happen – some plausible thoughts…..
The body regulates temperature through a complex network involving mitochondria, metabolism, the autonomic nervous system, blood sugar, hormones, inflammation, circulation, and the brain’s temperature-control centers.
🌀 Mitochondria play an important role because they help produce cellular energy. When mitochondria are under stress, cells may not produce energy as efficiently. That matters because energy production is closely tied to heat production, metabolism, and the body’s ability to keep temperature stable. Brown fat, which helps the body generate heat, is especially dependent on healthy mitochondrial function. Research shows that brown adipose tissue contains mitochondria that are highly involved in heat production and thermogenesis.
The autonomic nervous system is another piece of the puzzle. This is the part of the nervous system that helps control sweating, blood vessel constriction and dilation, heart rate, and other automatic functions. When it is not regulating well, temperature changes can bring on chills, flushing, overheating, shakiness, weakness, or trouble adjusting normally.
🔥 Heat exposure can place extra demand on this system. Hot weather, direct sun, exercise in heat, saunas, or hot tubs make the body work harder to cool itself and maintain circulation. That may help explain why people with fluoroquinolone-associated injury can experience poor heat tolerance, worsening symptoms after sun or sauna exposure, trouble cooling down once overheated, or an increased heart rate in heat or direct sun. The heart rate piece can be especially unsettling. In heat, the heart may beat faster as the body tries to move blood toward the skin to release heat. For people with autonomic instability, this normal cooling response can become exaggerated, uncomfortable, or difficult to calm down.
❄️Cold can be difficult too. When the body gets too cold, it has to work harder to maintain core temperature through shivering, blood vessel tightening, stress-hormone signaling, and increased metabolic demand. For someone already dealing with mitochondrial stress, nervous system sensitivity, circulation issues, or dysautonomia**-like symptoms, cold weather, strong air conditioning, cold water, or being chilled too long can feel especially draining and may worsen fatigue, muscle tightness, tremors, weakness, pain, or temperature instability.
Inflammation and oxidative stress may add another layer. Mitochondrial dysfunction can increase reactive oxygen species, which may further disrupt cellular signaling and nervous system stability. Several studies and reviews discuss fluoroquinolone-related mitochondrial dysfunction, oxidative stress, and possible vulnerability in people with reduced antioxidant defenses or mitochondrial susceptibility.
✅ For those living with fluoroquinolone-associated injury, the focus is often on reducing extra stress on the body rather than pushing through symptoms. This can include pacing activity, resting after exertion, staying hydrated, considering electrolytes when appropriate, and being cautious with temperature extremes such as direct sun, saunas, hot tubs, strong air conditioning, cold water, or prolonged cold exposure.
It may also be helpful to speak with a doctor in functional medicine about thyroid function, anemia, blood sugar regulation, dehydration, electrolyte imbalance, blood pressure changes, heart rhythm concerns, symptoms related to dysautonomia, and other issues that can affect temperature control, heart rate, weakness, and fatigue.
*Medications in the fluoroquinolone class (incl: Cipro/ciprofloxacin, Levaquin (off market)/levofloxacin, Avelox/moxifloxacin etc) in all forms for humans and pets: fq100.org/drug-list
**Dysautonomia: is a dysfunction of the autonomic nervous system, which controls automatic body functions such as heart rate, blood pressure, temperature regulation, digestion, and sweating.
Find support and resources on our sites:
🌐 Website & Resources: fq100.org/
▶️ YouTube: youtube.com/@FqAntibioticDam…
🔵 Facebook: facebook.com/fqtoxicitystudy…
🐦 X/Twitter: twitter.com/FQ_100
References:
1. U.S. Food and Drug Administration. Ciprofloxacin Prescribing Information. Revised September 2024.
accessdata.fda.gov/drugsatfd…
2. Michalak K, Sobolewska-Włodarczyk A, Włodarczyk M, Sobolewska J, Woźniak P, Sobolewski B. Treatment of the Fluoroquinolone-Associated Disability: The Pathobiochemical Implications. Oxidative Medicine and Cellular Longevity. 2017.
pmc.ncbi.nlm.nih.gov/article…
3. Kalghatgi S, Spina CS, Costello JC, Liesa M, Morones-Ramirez JR, Slomovic S, Molina A, Shirihai OS, Collins JJ. Bactericidal Antibiotics Induce Mitochondrial Dysfunction and Oxidative Damage in Mammalian Cells. Science Translational Medicine. 2013;5(192):192ra85.
pmc.ncbi.nlm.nih.gov/article…
4. Bertholet AM, Kirichok Y. Mitochondrial H Leak and Thermogenesis. Annual Review of Physiology. 2022;84:381-407.
pmc.ncbi.nlm.nih.gov/article…
5. Crandall CG, González-Alonso J. Cardiovascular Function in the Heat-Stressed Human. Acta Physiologica. 2010;199(4):407-423.
pmc.ncbi.nlm.nih.gov/article…
6. Low DA, Keller DM, Wingo JE, Brothers RM, Crandall CG. Sympathetic Nerve Activity and Whole Body Heat Stress in Humans. Journal of Applied Physiology. 2011;111(5):1329-1334.
pmc.ncbi.nlm.nih.gov/article…
7. Ouzzahra Y, et al. Effect of Acute Cold Exposure on Energy Metabolism and Activity of Brown Adipose Tissue in Humans: A Systematic Review and Meta-Analysis. Frontiers in Physiology. 2022;13:917084.
frontiersin.org/journals/phy…
8. Cleveland Clinic. Dysautonomia. Last reviewed September 11, 2023.
my.clevelandclinic.org/healt…
#Fluoroquinolones #FQAD #FQToxicity #FluoroquinoloneToxicity #Mitochondria #MitochondrialDysfunction #OxidativeStress #Dysautonomia #AutonomicNervousSystem #TemperatureRegulation #HeatIntolerance #ColdIntolerance #Neuropathy #AntibioticSideEffects #AdverseDrugReaction #DrugSafety #Cipro #Ciprofloxacin #Levofloxacin #Moxifloxacin
3
7
239
The Informed Consent Charade: Are Patients Truly Protected? peoplespharmacy.com/articles… via @peoplespharmacy
2
1
4
86
‼️There is a place to leave a comment directly on the online article for their community to see. If you were not warned about the possible adverse effects and/or the black box warnings when you were prescribed these medications, please consider sharing that there so others may learn and create awareness! See the comment guidelines first.
2
54
We have some resources for you ✏️
Dealing with fluoroquinolone antibiotic adverse effects and an upcoming doctor appointment? Feeling isolated and lost? We want you to feel a little more prepared and a little less alone.
We put some supportive tools in one place so you do not have to reinvent the wheel on a day when your body and brain may already be doing a lot.
🟣A printable ICD-10 code sheet you can bring with you
ICD-10 simply means the standardized diagnosis and billing codes used in medical records and by insurance. As of October 1, 2025, fluoroquinolone adverse effects have their own ICD-10 code category. That can make it easier for a clinician to document your reaction accurately and consistently.
➦Check out the code list, included FDA warnings and Black Box timeline to print and take with you in the downloads section.
🟣The Adverse Effects Evaluation Form
Many people tell us the hardest part of an appointment is remembering everything their body is experiencing, especially adverse effects that are ever-changing and piling up. This downloadable form helps you check-off what you have experienced, when it started, and what changed over time, so you can walk in with a clear snapshot.
➦Check out this form in the downloads section.
🟣Medical care
If you are looking for a clinician who may be more open to documenting complex reactions, our Find Medical page shares starting points and resources to help with your search.
➦Check out our Dear Doctor letters in the downloads section
🟣Support in the community
Seek comfort in a like-minded community via our Find Support page reflecting groups in multiple countries. Even one kind conversation with someone who gets it can make a tough day feel a bit lighter.
➨➨➨➨❗Start here (best first step & for downloads): fq100.org/find-help
Find Medical: fq100.org/find-medical
Find Support: fq100.org/find-support
💊Medications in the fluoroquinolone class (incl: Cipro/ciprofloxacin, Levaquin (off market)/levofloxacin, Avelox/moxifloxacin etc) in all forms for humans and pets: fq100.org/drug-list
Looking for more info? Check out our past Facebook posts and our YouTube channel: ▶️: youtube.com/@FqAntibioticDam…
1
2
7
129
A Letter Every Doctor Should Read – From a Physician Who Was "Floxed" by a Fluoroquinolone Antibiotic:
Over 10 years ago, anesthesiologist Dr. Todd R. Plumb, wrote a pertinent letter to colleagues after experiencing severe adverse effects from a common medication in the fluoroquinolone* family of antibiotics. His perspective as both doctor and patient, and his call for better awareness and more careful, compassionate care is sadly still very relevant today as we continue to fight and research for answers, awareness and treatments. The new ICD10 medical diagnosis code** was a start, but we still have much work to do.
🌀You can download this below letter, along with the publication references, from our Help page under “Downloadable Materials”, where you will also find multiple resources that may help an upcoming doctor visit go more smoothly, especially if you are seeking the medical diagnosis code for fluoroquinolones: fq100.org/find-help
➥ We also want to say this: if you are a healthcare professional who has been affected and feel hesitant to speak out, you are not alone. We welcome you to reach out to the Foundation through the Contact Us page on our website below.
Dr. Plumb’s letter✏️
Dear Doctor,
As you are probably aware, the fluoroquinolone class of antibiotics is useful for certain serious infections. Unfortunately, fluoroquinolones also have a long history of serious adverse drug reactions, many of them long term. [1] As a consequence of these reactions, several of these drugs have been removed from clinical practice or their use severely restricted. Besides the severe life-threatening immediate reactions, those of a more chronic nature may occur.
The spectrum of these adverse reactions is extremely broad. Patients suffering from these reactions are often misdiagnosed, referred for a psychiatric consult or even unfairly labeled as "difficult patients."
Many physicians have not been properly educated about the severe nature of these chronic adverse reactions, some of which result in life-long disabilities. Post-marketing studies of several flouroquinolones have shown an incidence of adverse reactions much higher than were originally reported in pre-clinical studies. [1,2,3]
You are probably aware that the fluoroquinolones are eukaryotic DNA gyrase and topoisomerase inhibitors very similar to many antineoplastic agents. Because of their similar mechanisms of action, it's no surprise that fluoroquinolones and many antineoplastic agents share similar toxicity profiles. Studies have even been conducted using fluoroquinolones to inhibit neoplastic chondrocyte growth in chondrosarcoma. [4]
There are many patients who have a syndrome of associated symptoms that include, but are not limited to:
CNS agitation, depression, insomnia, new-onset anxiety and panic attacks, and even elevated intracranial pressure and visual abnormalities. They may also present with peripheral neuropathy usually of the small fiber type with temperature and pain sensory aberrations, but also often involving larger sensory and motor nerves. Spontaneous muscle activity with fasciculations, myokymia and myoclonic jerks may also occur. Many have musculoskeletal damage with degeneration of cartilage and tendons often leading to tendon rupture and severe ongoing musculoskeletal pain long after therapy has been discontinued. [1,2,3,4,5,6,7,8]
This complex symptomatology does not usually resolve after discontinuation of the inducing fluoroquinolone and may in fact worsen. Many patients go on to have disability that may persist for years. [1] Unfortunately, such patients are often seen by many physicians from multiple specialties who, given the complex symptomatology, fail to recognize a unifying diagnosis.
The mechanism of injury is not fully apparent, but several studies have been conducted and researchers have implicated the following possible mechanisms:
1. Inhibition or disruption of the CNS GABA receptor. [9]
2. Depletion of magnesium and disruption of cellular enzymatic function. [10]
3. Disruption of mitochondrial function and energy production. [11,12]
4. Oxidative injury and cellular death. [14]
This seems to be a functional disorder and structural abnormalities are not usually seen on radiological studies. [13] Patients may have abnormal EMG/NCV studies, abnormal skin punch neurologic density and morphology, abnormal vasomotor and sudomotor function on autonomic testing, and abnormal degeneration of tendons and cartilage on MRI. [13]
There may be a large number of these patients with coexisting endocrine abnormalities including: antithyroid antibodies and abnormal thyroid function, abnormal adrenal function with either hyper or hypocortisolism, hypogonadism, hypo or hyperglycemia and possibly impaired pituitary function. [13]
Most patients suffering from these side effects have a very clear onset of symptoms temporally related to a course of fluoroquinolone antibiotic. [13] They were often given the fluoroquinolone in conjunction with a corticosteroid or NSAID. Both of these classes of medications are associated with an increased incidence of adverse drug reaction from fluoroquinolones. [10,13]
As of yet no scientifically proven effective treatment is known, however patients will definitely benefit from your caring support and appropriate informed care. Of course, other diseases with similar symptoms need to be carefully ruled out.
There exists a large community of these patients who share information on the World Wide Web. Their numbers grow as the prescription of fluoroquinolones increases. Many of these patients are professionals like myself who have been affected by these drugs. Thank you for your time and consideration.
Todd R. Plumb MD
✏️✏️✏️✏️✏️✏️✏️✏️✏️✏️✏️
References: See this letter along with it's full references in the download section of this page: fq100.org/find-help
*💊Medications in the fluoroquinolone class (incl: Cipro/ciprofloxacin, Levaquin (off market)/levofloxacin, Avelox/moxifloxacin etc) in all forms for humans and pets: fq100.org/drug-list
** See more about the medical diagnostic code for fluoroquinolones: fq100.org/find-help
✏️✏️✏️✏️✏️✏️✏️✏️✏️✏️✏️✏️
Find support and resources on our sites:
🌐 Website resources: fq100.org
▶️ YouTube: youtube.com/@FqAntibioticDam…
🐦 X/Twitter: twitter.com/FQ_100
#FQAwareness #Fluoroquinolones #MitochondrialHealth #AntibioticSideEffects #Floxed #Cipro #Levaquin #FQAD
1
6
141
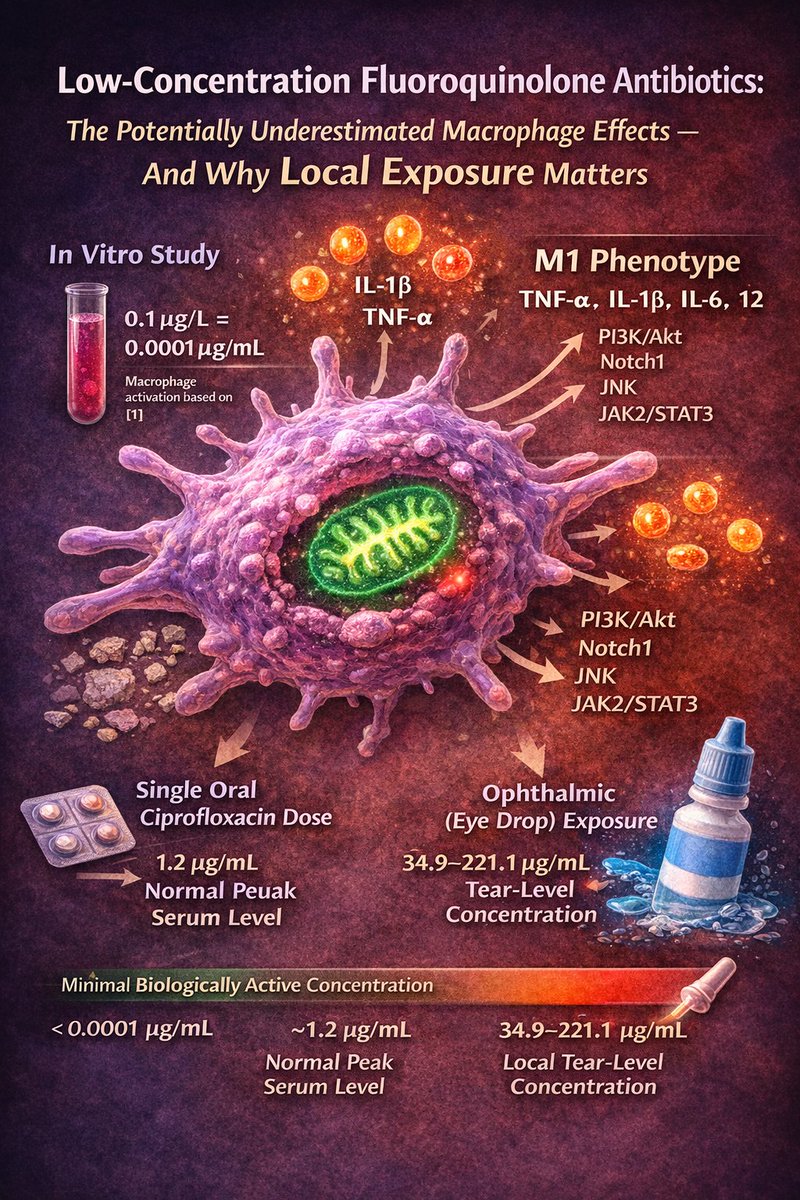
Part II Low-Concentration Macrophage Effects and Why Even Local Fluoroquinolone Exposure May Matter
One of the more striking findings in the macrophage literature is that quinolone-induced inflammatory signaling was reported at an extremely low external culture-medium concentration of 0.1 μg/L in RAW264.7 macrophages [1]. That detail matters.
The study was not measuring serum concentrations, and it was not measuring directly quantified intracellular concentrations inside macrophages. It was asking a more basic mechanistic question:
how little quinolone exposure in the surrounding medium is needed before macrophage inflammatory behavior begins to shift
At that level, the authors reported increased pro-inflammatory cytokine signaling, including TNF-α, IL-1β, IL-6, and IL-12, together with activation of pathways such as PI3K/Akt, Notch1, JNK, and JAK2/STAT3, consistent with a more M1-like inflammatory phenotype.
Put differently, this work suggests that macrophage inflammatory signaling may respond at a very low exposure threshold. The comparison to human dosing must be made carefully, because 0.1 μg/L in cell culture medium is not the same thing as serum concentration in a patient, nor is it the same as a directly measured intracellular concentration inside a macrophage. Even so, the scale is notable. That concentration equals 0.0001 μg/mL, which is far below levels reached in humans even after low standard oral fluoroquinolone dosing. After a single 250 mg oral dose of ciprofloxacin, mean peak serum concentrations are about 1.2 μg/mL, and mean concentrations at 12 hours are still about 0.1 μg/mL.
The same labeling reports that urine concentrations after a single 250 mg dose usually exceed 200 μg/mL during the first two hours and remain around 30 μg/mL at 8–12 hours. Although those are serum and urine values rather than macrophage intracellular concentrations, they show that routine human exposures can be vastly higher than the very low external concentration that was sufficient to alter macrophage signaling in vitro [1–3].
This is also why local exposure from fluoroquinolone eye drops cannot be dismissed automatically. Ophthalmic administration produces a very different pharmacokinetic profile from oral dosing, but it demonstrates the same basic principle: a drug can create very high local tissue-surface exposure even when systemic absorption is much lower. For levofloxacin ophthalmic solution 0.5%, mean tear concentrations after a single drop ranged from 34.9 to 221.1 μg/mL during the first 60 minutes and were still about 17.0 μg/mL at 4 hours and 6.6 μg/mL at 6 hours. In the same product information, plasma concentrations after ophthalmic dosing were low but measurable, ranging from about 0.86 to 2.05 ng/mL one hour after dosing, with a highest maximum mean concentration of about 2.25–2.5 ng/mL during intensive dosing. More concentrated ophthalmic levofloxacin formulations have shown even higher tear concentrations, including values around 757 μg/mL at 15 minutes, together with low-ng/mL plasma exposure [4,5].
The practical implication is not that eye drops should be assumed to produce the same risk profile as tablets or intravenous therapy. That would overstate the evidence. The more careful conclusion is that very low concentrations have already been shown to alter macrophage inflammatory behavior in vitro, while local ophthalmic exposure can generate concentrations at the ocular surface that are orders of magnitude higher than that in vitro threshold, even though blood levels remain much lower than after oral dosing. If macrophages or related immune-responsive cells are involved in tissue-level responses to fluoroquinolones, then local routes of exposure may still be biologically relevant, at least in principle [1,4,5].
This point becomes even more important when viewed together with the broader macrophage and mitochondrial literature.
Fluoroquinolones have been reported to drive mitochondrial hyperpolarization and modulate iNOS expression in monocyte-derived macrophage populations [6]. Other work has shown ciprofloxacin-driven increases in IL-1β and TNF-α together with pro-inflammatory macrophage polarization in mammalian models [7]. More broadly, macrophages are now recognized as central regulators of inflammation resolution, tissue repair, fibrosis, and regeneration, while mitochondrial dysfunction in macrophages has been linked to impaired repair and persistent inflammatory signaling [8–12].
Taken together, these studies do not prove that every low or local exposure causes clinically meaningful toxicity in humans. They do, however, support a biologically plausible concern:
that even relatively small exposures may be capable of influencing macrophage inflammatory programming under certain conditions, and that high local surface concentrations — such as those achieved with ophthalmic dosing — deserve more attention than they have usually received.
If these findings translate, even partially, to humans, the theoretical consequences could be important. Macrophages help determine whether tissues move from acute defense into true recovery. If fluoroquinolones shift macrophages toward a more persistent M1-like, cytokine-driven state, or disturb their mitochondrial function enough to impair their repair role, then one possible downstream effect would be poor resolution of inflammation. In practical terms, that could theoretically contribute to more:
persistent tissue irritation,
delayed recovery after injury or infection,
prolonged inflammatory flares,
slower wound healing, and
greater difficulty returning to baseline after physical, infectious, or chemical stress.
In tissues where macrophages play especially strong regulatory roles, such as the lungs, ocular surface, connective tissue, and mucosal barriers, an abnormal inflammatory or immunometabolic response could in principle amplify local injury or prolong symptoms beyond what would be expected from a short-lived drug exposure alone. This remains a mechanistic projection, not a proven one-to-one clinical outcome [6–12].
The most responsible conclusion, therefore, is neither dismissal nor overstatement. These macrophage studies do not prove that low-dose, local, or ophthalmic fluoroquinolone exposure necessarily causes lasting human disease. What they do show is that macrophage biology can respond to quinolone exposure at very low levels in vitro, and that local tissue exposure from common formulations can greatly exceed those levels. That combination is sufficient to justify a more serious mechanistic discussion and, more importantly, direct human research.
Future studies should examine whether comparable macrophage signaling changes occur in human primary macrophages, in patient-derived immune cells, and in clinically relevant exposure models, including low-dose and local routes of administration. Without that work, the human significance of these findings will remain uncertain. With it, the field may better understand whether macrophage dysregulation is one of the missing links between fluoroquinolone exposure and prolonged multi-system symptoms reported by patients [1,4,6].
✏️Author note: This article was authored by Jerzy Tyszkowski, with AI used only for drafting and language refinement.
🌀 🌀 Disclaimer: This article is an educational, science-based interpretive summary intended for hypothesis generation. It does not establish clinical causation in any individual patient and should not be taken as medical advice, diagnosis, or treatment guidance. The mechanistic implications discussed here are based on experimental and preclinical findings and should be understood as biologically plausible interpretations that still require confirmation in human studies.
💊Medications in the fluoroquinolone class (incl: Cipro/ciprofloxacin, Levaquin (off market)/levofloxacin, Avelox/moxifloxacin etc) in all forms for humans and pets: fq100.org/drug-list
Find support and resources on our sites:
🌐 Website & Resources: fq100.org/
▶️ YouTube: youtube.com/@FqAntibioticDam…
🔵 Facebook: facebook.com/fqtoxicitystudy…
🐦 X/Twitter: twitter.com/FQ_100
References
[1] Lang L, Zhang Y, Yang A, Dong J, Li W, Zhang G. Macrophage polarization induced by quinolone antibiotics at environmental residue level. International Immunopharmacology. 2022;106:108596. doi:10.1016/j.intimp.2022.108596.
[2] Ciprofloxacin Tablets USP prescribing information. Pharmacokinetics after oral dosing: peak serum concentration after a 250 mg oral dose approximately 1.2 μg/mL; mean 12-hour concentration approximately 0.1 μg/mL.
[3] CIPRO prescribing information. After a 250 mg oral dose, urine concentrations usually exceed 200 μg/mL during the first 2 hours and are approximately 30 μg/mL at 8 to 12 hours after dosing.
[4] QUIXIN™ (levofloxacin ophthalmic solution 0.5%) prescribing information. Mean tear concentrations 34.9–221.1 μg/mL during the first 60 minutes after a single drop; approximately 17.0 μg/mL at 4 hours and 6.6 μg/mL at 6 hours; plasma concentrations about 0.86–2.05 ng/mL, with highest maximum mean approximately 2.25–2.5 ng/mL during intensive dosing.
[5] IQUIX® (levofloxacin ophthalmic solution 1.5%) prescribing information. Mean tear concentration approximately 757 μg/mL at 15 minutes after instillation; plasma concentrations in the low ng/mL range.
[6] Hardgrave AW, Dooley M, Maminimini I, Faniyi A, Christodoulidou A, Alshammari Y, March HJ, D’Elia RV, Worthington JJ. Fluoroquinolones directly drive mitochondrial hyperpolarization and modulate iNOS expression in monocyte-derived macrophage populations. Discovery Immunology. 2025;4(1):kyaf018. doi:10.1093/discim/kyaf018.
[7] Fan M, Chen S, Weng Y, Li X, Jiang Y, Wang X, Bie M, An L, Zhang M, Chen B, Huang G, Wu J, Zhu M, Shi Q. Ciprofloxacin promotes polarization of CD86 CD206− macrophages to suppress liver cancer. Oncology Reports. 2020;44(1):91–102. doi:10.3892/or.2020.7602.
[8] Wang L, Yang K, Xie X, Wang S, Gan H, Wang X, Wei H. Macrophages as Multifaceted Orchestrators of Tissue Repair: Bridging Inflammation, Regeneration, and Therapeutic Innovation. Journal of Inflammation Research. 2025;18:8945–8959. doi:10.2147/JIR.S527764.
[9] Cai S, Zhao M, Zhou B, Yoshii A, Bugg D, Villet O, Sahu A, Olson GS, Davis J, Tian R. Mitochondrial dysfunction in macrophages promotes inflammation and suppresses repair after myocardial infarction. Journal of Clinical Investigation. 2023;133(4):e159498. doi:10.1172/JCI159498.
[10] Zheng H, Cheng X, Jin L, Shan S, Yang J, Zhou J. Recent advances in strategies to target the behavior of macrophages in wound healing. Biomedicine & Pharmacotherapy. 2023;165:115199. doi:10.1016/j.biopha.2023.115199.
[11] Jiang Y, Cai R, Huang Y, et al. Macrophages in organ fibrosis: from pathogenesis to therapeutic targets. Cell Death Discovery. 2024;10(1):487. doi:10.1038/s41420-024-02247-1.
[12] Zhao C, Yang Z, Li Y, Wen Z. Macrophages in tissue repair and regeneration: insights from zebrafish. Cell Regeneration. 2024;13(1):12. doi:10.1186/s13619-024-00195-w.
#FQAwareness #Fluoroquinolones #MitochondrialHealth #AntibioticSideEffects #Floxed #Cipro #Levaquin #FQAD
4
181
The Newest Study 2025/26
Macrophages, Mitochondria, and Fluoroquinolones: A New Clue in the FQAD Story
[This review article was written by Jerzy Tyszkowski with the assistance of AI]
Macrophages are among the most important cells of the innate immune system, yet they are rarely discussed in the broader public conversation about fluoroquinolone toxicity. These cells are found throughout the body and act as local guardians of tissue health. They clear debris, engulf microbes, present antigens, regulate inflammation, and help determine whether injured tissue moves toward recovery or toward chronic dysfunction. Because they sit at the crossroads of immunity, metabolism, and repair, any drug that alters macrophage behavior may have consequences well beyond a simple antimicrobial effect.
That is why the newer macrophage literature on fluoroquinolones deserves attention. A recent paper by Hardgrave and colleagues reported that fluoroquinolones directly induced mitochondrial hyperpolarization and altered iNOS expression in monocyte-derived macrophage populations. Importantly, the authors concluded that these effects were independent of obvious cytotoxicity and independent of pH changes in the culture conditions, which strengthens the argument that the antibiotics were directly altering macrophage biology rather than simply poisoning the cells nonspecifically. In the same study, the investigators proposed that mitochondrial hyperpolarization could prime macrophages toward a more inflammatory phenotype.
A second study, by Lang and colleagues, examined quinolone antibiotics in RAW264.7 macrophages and found that even very low concentrations could promote M1-type polarization and increase pro-inflammatory mediators such as TNF-α, IL-1β, IL-6, and IL-12. The authors described activation of signaling pathways including PI3K/Akt, Notch1, JNK, and JAK2/STAT3, suggesting that quinolones were not merely passive exposures but active modulators of macrophage programming. Although this was an environmental-residue model rather than a standard therapeutic exposure model, it still showed that quinolones can influence macrophage inflammatory direction.
A third paper, by Fan and colleagues, focused specifically on ciprofloxacin and found that it promoted a CD86 CD206− macrophage phenotype together with increased IL-1β and TNF-α production. That work was conducted in a tumor-related context, so it should not be overstated as a direct mirror of ordinary clinical exposure. Even so, it remains highly relevant because it demonstrates that ciprofloxacin can shift macrophage phenotype and cytokine output in mammalian systems.
These findings become more significant when placed next to the older mitochondrial literature on fluoroquinolones. Earlier cell studies showed delayed cytotoxicity, mitochondrial DNA injury, reduced mitochondrial DNA content, impaired respiration, and disturbances in mitochondrial replication biology after ciprofloxacin exposure. More broadly, the literature on macrophage biology shows that mitochondrial function is not a side issue in these cells. It is central to whether macrophages resolve inflammation efficiently, clear damaged cells, and support normal tissue repair. When macrophage mitochondrial function is disrupted, inflammation may persist and repair may weaken.
This is why macrophages matter so much in the context of fluoroquinolone toxicity. In the healthy setting, macrophages are highly plastic. They move along a spectrum, often simplified as M1 and M2 states. A more inflammatory M1-like response helps fight danger early, while a more reparative M2-like response helps resolve inflammation and support healing later. The problem comes when that balance is chronically disturbed. Reviews on wound healing, tissue repair, and fibrosis consistently show that persistent inflammatory macrophage activation can impair healing, sustain tissue damage, and contribute to fibrotic remodeling.
If these macrophage findings were to translate more directly to humans than has yet been proven, the consequences would likely not appear as one single “macrophage syndrome.” Instead, they would probably emerge as a pattern of poor resolution of inflammation and impaired tissue recovery.
The most plausible consequences would include slower healing after injury, more persistent tissue irritation, greater inflammatory reactivity after physical or chemical stress, and difficulty shifting from an “injury response” into a true repair phase. In organs where macrophages are especially important, such as the lungs, gut, liver, nerves, and connective tissue, that kind of distorted immunometabolic signaling could theoretically make symptoms linger longer than expected. This remains a mechanistic possibility, not a proven clinical fact.
If one makes that theoretical extrapolation, the symptom profile that might follow would be biologically consistent with what is already known about macrophage-driven inflammation and mitochondrial dysfunction. One could expect persistent fatigue, exercise intolerance, post-exertional worsening, slower recovery after illness or physical strain, ongoing muscle or soft-tissue pain, heightened inflammatory flares, delayed wound healing, and in some individuals potentially a stronger tendency toward chronic tissue irritation or fibrosis. In tissues such as the lungs or gut, this might theoretically contribute to prolonged sensitivity, inflammatory reactivity, or incomplete return to baseline after exposure. Again, this is not a statement that these macrophage studies have already proven these exact symptoms in patients. It is a carefully framed projection of what such biology could mean if the laboratory findings track more closely with human disease than is currently established.
The larger point is that the fluoroquinolone story may be wider than direct mitochondrial injury in isolated target cells. If these drugs also disturb the cells responsible for surveillance, cleanup, inflammatory control, and tissue repair, then they may help explain why some people do not simply experience a short-lived adverse reaction, but instead struggle with a more prolonged, multi-system pattern of impaired recovery. That possibility does not replace the existing work on tendons, nerves, or mitochondrial DNA. It adds another layer to it. Macrophages may represent one of the missing links between cellular injury and the body’s failure to return to equilibrium.
That is why future FQ/FQAD research should not focus only on whether fluoroquinolones damage cells directly, but also on whether they alter the immune cells that decide how damage is processed, contained, repaired, or prolonged. If those questions are confirmed in stronger human models, the clinical understanding of fluoroquinolone toxicity may need to expand from a narrow adverse-drug-reaction framework into a broader picture of host-cell immunometabolic injury.
✅Disclaimer: This article is a science-based interpretive summary intended for education and hypothesis generation. It does not establish direct clinical causation in any individual patient and should not be understood as medical advice, diagnosis, or treatment guidance. Some of the mechanistic implications discussed here are theoretical extrapolations from experimental and preclinical findings and require further validation in human studies.
Find support and resources on our sites:
🌐Website & Resources: fq100.org/
▶️YouTube: youtube.com/@FqAntibioticDam…
🔵 Facebook: facebook.com/fqtoxicitystudy…
🐦 X/Twitter: twitter.com/FQ_100
#FQAwareness #Fluoroquinolones #MitochondrialHealth #AntibioticSideEffects #Floxed #Cipro #Levaquin #FQAD
1
3
13
929
✏️✏️✏️Update:
Addendum: Which Symptoms in Our Adverse Effects Evaluation Form Best Fit the Macrophage–Mitochondria Model?
➥see our form in the download section: fq100.org/find-help
After reviewing our Adverse Effects Evaluation Form in detail, it is clear that many of the symptom groups listed there are biologically consistent with the newer macrophage findings. The macrophage–mitochondria model does not explain every feature of fluoroquinolone toxicity by itself, but it may help explain why some patients develop a prolonged multisystem pattern of poor recovery, inflammatory reactivity, nerve hypersensitivity, autonomic instability, gut dysfunction, psychiatric symptoms, and unusual sensitivity to ordinary triggers.
➥Peripheral Neuropathy, Neuralgia, Burning Pain, Allodynia, and Hyperalgesia
This is one of the strongest fits. Our form includes tingling, numbness, electric shocks, burning pain, neuralgia, altered skin sensitivity, allodynia, hyperalgesia, fasciculations, tremors, and limb weakness. These symptoms are already consistent with recognized fluoroquinolone-associated peripheral nerve toxicity. The macrophage model may add an important second layer by helping explain why nerve irritation, pain amplification, and sensory overreactivity can remain prolonged instead of resolving normally.
pmc.ncbi.nlm.nih.gov/article…
pmc.ncbi.nlm.nih.gov/article…
pmc.ncbi.nlm.nih.gov/article…
➥Psychiatric and Neuropsychiatric Symptoms, Including Psychosis
Our form also includes anxiety, panic, insomnia, confusion, memory loss, brain fog, depersonalization, depression, suicidal thoughts, agitation, personality changes, nightmares, disorientation, bipolar symptoms, seizures, and psychosis. These are important to include. The most careful interpretation is that they fit the known spectrum of fluoroquinolone neuropsychiatric toxicity and CNS hyperexcitability, likely involving disturbed inhibitory signaling, GABA-related mechanisms, and broader neuroimmune dysfunction. The macrophage–mitochondria model may not fully explain psychosis by itself, but it strengthens the argument that persistent neuroinflammatory and immunometabolic dysregulation could contribute to these severe CNS and psychiatric reactions.
pubmed.ncbi.nlm.nih.gov/3290…
pubmed.ncbi.nlm.nih.gov/2158…
pubmed.ncbi.nlm.nih.gov/1658…
➥Extreme Fatigue, Exercise Intolerance, Post-Exertional Worsening, and Fibromyalgia-Like Pain
This is another very strong fit. Our form includes extreme fatigue, exercise intolerance, muscle pain, weakness, soft-tissue pain, and impaired endurance. If macrophages remain locked in a more inflammatory mitochondrial state, the body may stay in an injury-response mode longer and shift less effectively into true tissue repair. That provides a biologically coherent explanation for post-exertional worsening, persistent pain, slower recovery, and a fibromyalgia-like pattern.
pubmed.ncbi.nlm.nih.gov/4150…
pmc.ncbi.nlm.nih.gov/article…
➥Dysautonomia, POTS-Like Symptoms, and Cardiovascular Instability
Our form lists lightheadedness, dizziness on standing, dysautonomia, tachycardia, bradycardia, arrhythmia, low blood pressure, sweating abnormalities, poor circulation, temperature dysregulation, and shortness of breath. These symptoms fit well as indirect downstream effects of persistent inflammatory and immunometabolic dysregulation. This does not prove that macrophage dysfunction alone causes POTS, but it supports a plausible model in which autonomic instability develops in the setting of chronic inflammatory signaling and impaired recovery biology.
pubmed.ncbi.nlm.nih.gov/4150…
pmc.ncbi.nlm.nih.gov/article…
➥MCAS-Like Reactivity, Hives, Pruritus, Anaphylactic-Type Reactions, and Bronchospasm
Our form includes urticaria, itching, rash, mucocutaneous reactions, bronchospasms, anaphylactic reaction, and broader exaggerated reactivity. These symptoms fit the model as indirect immune consequences. The careful wording is that macrophage dysfunction may contribute to a body environment that favors mast-cell-like overreactivity, histamine-related symptoms, and inflammatory flares, rather than proving formal MCAS in every patient. This is especially relevant when these reactions coexist with POTS-like or gut-reactive patterns.
pmc.ncbi.nlm.nih.gov/article…
pmc.ncbi.nlm.nih.gov/article…
pmc.ncbi.nlm.nih.gov/article…
➥Food Intolerance, Medication/Supplement Intolerance, Gut Dysfunction, and Post-Infectious Reactivity
This is also a strong fit. Our form includes food sensitivities, medication intolerance, supplement intolerance, bloating, abdominal pain, altered bowel patterns, gastroparesis, maldigestion, malnutrition, reflux, gut inflammation, and broader GI instability. Macrophages are essential for gut barrier integrity, mucosal immune balance, post-inflammatory repair, and the transition from inflammation to recovery. If their mitochondrial function is disturbed, food reactivity, gut barrier problems, and supplement intolerance become much more biologically plausible.
pmc.ncbi.nlm.nih.gov/article…
➥Chemical Sensitivity, Fume Intolerance, Material Sensitivity, Smell Hypersensitivity, and Multiple Chemical Sensitivity
Our form directly includes chemical intolerance, fume intolerance, materials sensitivity, smell hypersensitivity to odors, phantosmia, skin sensitivity to chemicals, and multiple chemical sensitivity. These are among the more complex symptoms, but they still fit the broader model as indirect neuroimmune effects. The safest way to state it is that persistent inflammatory signaling, mast-cell-related reactivity, sensory amplification, and impaired barrier function may help explain why ordinary environmental exposures become disproportionately provocative in some patients.
pmc.ncbi.nlm.nih.gov/article…
pmc.ncbi.nlm.nih.gov/article…
➥Headaches, Migraines, Pressure Sensations, Hyperacusis, Visual Snow, and Sensory Overload
Our form includes headaches, migraines, head pressure, hyperacusis, visual snow, photophobia, smell hypersensitivity, and other sensory-processing problems. These are not necessarily caused directly by macrophages alone, but they are consistent with a broader neuroimmune sensitization state in which inflammatory cells and sensory pathways remain abnormally reactive. The macrophage model may therefore help connect mitochondrial injury with persistent sensory amplification rather than isolated organ damage alone.
pmc.ncbi.nlm.nih.gov/article…
pubmed.ncbi.nlm.nih.gov/2158…
➥Poor Wound Healing, Skin/Mucosal Reactivity, and Incomplete Tissue Repair
Our form includes poor wound healing, reopening of scars or cuts, mucocutaneous reactions, inflammatory skin lesions, and chronic tissue irritation. This fits very well with the idea that altered macrophage programming may impair the normal resolution of inflammation and transition to repair. In that setting, the body does not simply react too strongly; it also fails to finish healing properly.
pubmed.ncbi.nlm.nih.gov/4150…
pmc.ncbi.nlm.nih.gov/article…
❗Important Limitation
Not every symptom in the form is equally explained by this macrophage article. Some findings in the form, such as tendon rupture, major collagen breakdown, retinal detachment, aortic aneurysm, and certain structural tissue injuries, likely involve additional or separate mechanisms, including direct connective-tissue toxicity, oxidative stress, matrix disruption, or other fluoroquinolone effects beyond macrophage dysfunction. So this addendum should be presented as an expansion of the model, not as a claim that macrophages explain all fluoroquinolone damage.
pubmed.ncbi.nlm.nih.gov/4150…
✅Bottom Line✅
After comparing the article to our full symptom evaluation form, the symptom groups that fit best are peripheral neuropathy and nerve hypersensitivity, psychiatric and neuropsychiatric symptoms, fatigue, exercise intolerance, fibromyalgia-like pain, dysautonomia/POTS-like symptoms, MCAS-like reactivity, food and supplement intolerance, gut dysfunction, chemical and fume sensitivity, sensory overload, and poor wound healing. In other words, this macrophage–mitochondria model may help explain not only direct tissue injury, but the body’s failure to return to equilibrium after fluoroquinolone exposure.
✨✨✨Disclaimer: This addendum is a science-based interpretive summary intended for education and hypothesis generation. It does not establish direct clinical causation in any individual patient and should not be understood as medical advice, diagnosis, or treatment guidance.
1
4
89