
internist - primary care - assistant professor | - (Salary 233k RVU bonus) - no other COI
- Tweets 1,174
- Following 377
- Followers 306
- Likes 848












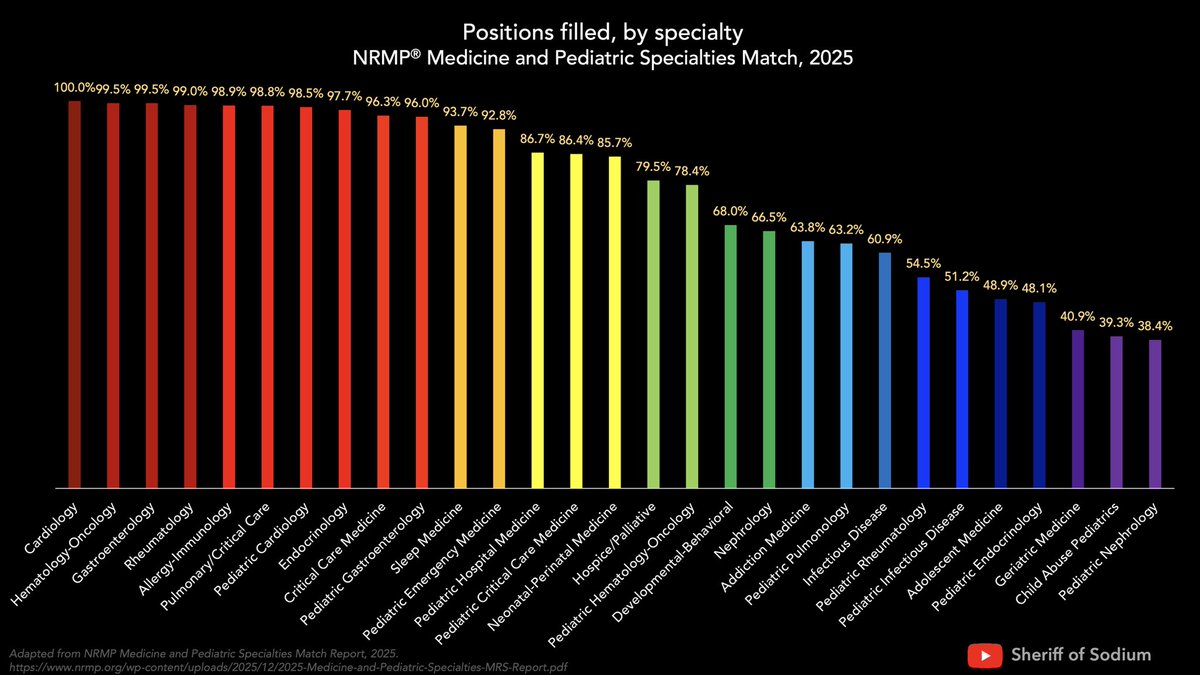
ALT Positions filled, by fellowship specialty, in the 2025 NRMP Medicine and Pediatric Specialties Match. Cardiology, Hematology-Oncology, Gastroenterology, and Rheumatology filled >99% of available positions, while Geriatrics, Child Abuse Pediatrics, and Pediatric Nephrology filled 41% or less.
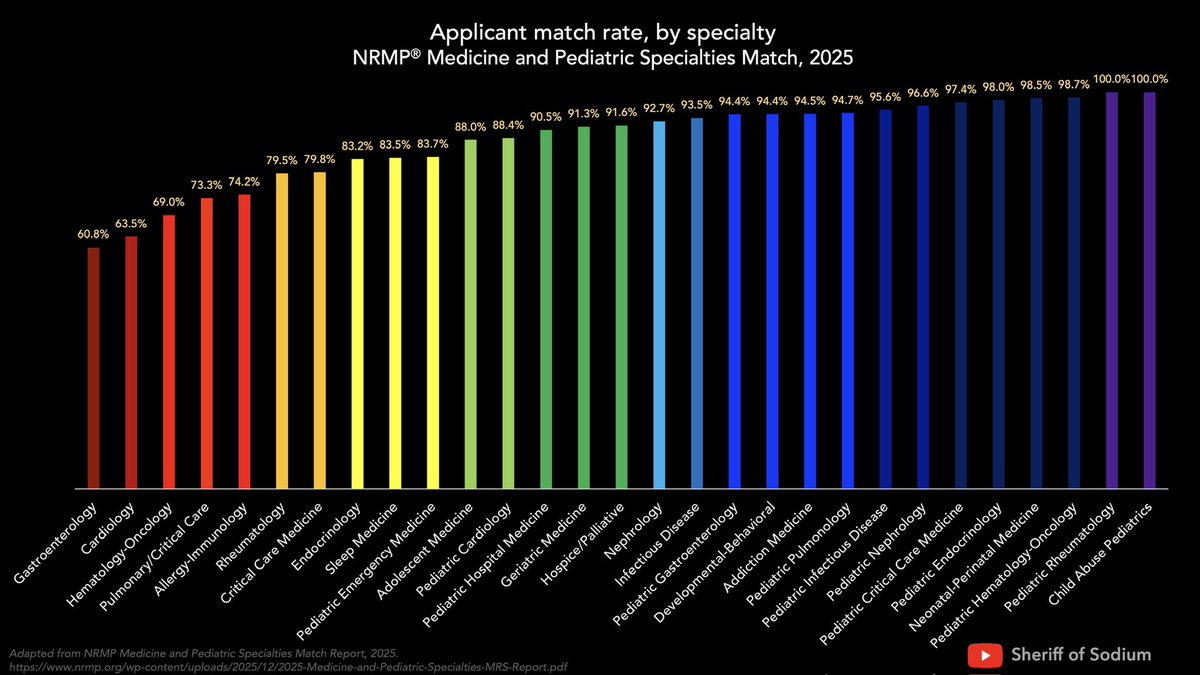
ALT Applicant match rate, by specialty, for the 2025 NRMP Medicine and Pediatric Specialties Match. Match rates for Gastroenterology, Cardiology, and Hematology Oncology were 61%, 64%, and 69%, respectively, while applicants in Pediatric Endocrinology, Neonatal-Perinatal Medicine, Pediatric Hematology-Oncology, Pediatric Rheumatology, and Child Abuse Pediatrics had 98 % match rates.
