
Investor for 40 years. Focused on markets, trading, long-term compounders, precision medicine, and diagnostics. Caris shareholder. Personal views only.
Joined August 2023
- Tweets 848
- Following 146
- Followers 202
- Likes 1,446
64 Photos and videos



Reduction and Repetition (Part 2 of 2)
Last time I argued that Palantir and Astera Labs prove the same thing in opposite styles: a company doesn't need a particular persona, but the market needs to know what to repeat. War room or engineering lab, either works, as long as the story reduces.
So where do the four big names in precision oncology sit? Guardant, Natera, Tempus, Caris.
One distinction first, because it does most of the work: clarity is not the same as loudness. A company can reduce its story beautifully and still be reducing the wrong sentence, one that runs ahead of what the business has proven. Loud and repeatable isn't the same as accurate.
Tempus sits closest to the Palantir end. Founder-led, AI-forward, data-heavy, big-platform language. The market repeats it without effort: AI plus multimodal medical data makes medicine smarter. That's a clean reduction. The question isn't whether it's repeatable, it plainly is, but whether it's running at the right distance from the business or a step ahead of it.
Natera is the opposite temperament, closer to Astera. No prophet, no drama, an execution machine. Cell-free DNA platform across women's health, oncology, organ health, reimbursement, scale. Repeated commercially, relentlessly. It works because the sentence and the business run at the same speed: the story isn't ahead of the P&L, it's describing it.
Guardant already had a great reduction, and that's its problem. "Liquid biopsy" made the company instantly legible. But Guardant is now two stories with two buyers and two clocks, therapy selection on one side, screening on the other, wearing a single phrase. The original sentence no longer tells you which movie you're watching, and a phrase that once clarified can start to blur.
Caris is the hardest to place. Not Palantir, not Astera, not Natera. Founder-CEO, scientist-president, major clinical voices, pharma relationships, AI, tissue and liquid, WES and WTS, MI Profile, Assure, Detect, MI Clarity, ChromoSeq, POA. On the asset side, the breadth may be the whole advantage. On the storytelling side, it's a liability, because the market cannot repeat a list.
Tempus has "AI medicine." Natera has "cell-free DNA platform." Guardant had "liquid biopsy." Caris doesn't have the phrase yet, four audiences each seeing one face, none holding the whole. And the breadth makes that the expensive problem, not the small one: the market prices what it can repeat, so a company that asks it to repeat a list gets priced as a pile of parts, including the integrated whole that's supposed to be worth the most.
The exact words don't matter. The discipline does: one identity, repeatable in a breath, said until the market says it back.
Complexity without reduction is noise. Complexity with repetition becomes a category.
Caris investor.
80
Reduction and Repetition (Part 1 of 2)
I've been studying the storytelling architecture of recent IPO winners, how a company shows itself to the market, separate from the financials or the product spec.
Two examples could not be more different.
Palantir is narrated by one voice across fifty channels. Usually Alex Karp, sometimes Shyam Sankar, but whoever speaks, the message never changes, and it isn't really about software. Karp rants about the West, institutions, adversaries, national security, why the world is more dangerous than people admit. Palantir feels like a war room.
Astera Labs is the opposite. Three cofounders in chairs, presented as equals, calmly explaining connectivity bottlenecks and rack-scale architecture. No prophet. No drama. Astera feels like an engineering lab.
Both have been rewarded enormously, each up roughly tenfold or more from their lows. And here's what people miss: the persona fits the product.
What Astera sells is boring, the plumbing between chips, and a calm team of engineers is exactly right for it. What Palantir sells is mission-critical, the difference between a missile hitting in one second or not. Karp's intensity matches the stakes. Each narrator is connected to what's narrated.
Maybe none of this is the cause. Both stocks may just be riding the same AI wave, the narrative a passenger on a move the market would have made anyway. I can't disprove that. But the AI tide doesn't explain the difference in how these two are understood, or why each story fits its business so precisely.
This isn't a post about hype either. Hype is when the story runs ahead of the business, and that breaks. Both delivered. If you don't deliver, no story saves you.
The real question: when a company is delivering, how does it realize the full potential of its stock currency? That's where storytelling matters, as translation. One reduces emotionally, one technically. Same discipline underneath: make the market understand what's changing, why you matter, and repeat it back.
The market doesn't need every company to have an Alex Karp, or to sound like engineers in a lab. It needs to know what movie it's watching.
War room? Engineering lab? Clinical science? Data infrastructure? A platform hiding inside a product?
Part 2: how the four big names in precision oncology (Guardant, Natera, Tempus, and Caris) score on exactly this.
62

Jun 9
A quick thought on Caris Life Sciences vs Personalis.
I like Personalis.
It is doing important work in ultrasensitive MRD, and the company may become very relevant in recurrence monitoring.
But I do not think the market should view Personalis and Caris as similarly positioned companies.
Caris has the whole stack.
It has comprehensive genomic profiling.
It has more than a decade of accumulated oncology data.
It has tissue, blood, DNA, RNA, AI, pharma relationships, physician workflow, and a growing clinical platform.
It has launched ChromoSeq.
It has launched MI Clarity.
It has Detect coming in MCED.
It has MRD coming, and I expect that product to be very competitive.
And over time, the most important layer may not be any single test. It may be the decision layer: how the system helps physicians decide what to do next across profiling, recurrence risk, MRD, early detection, and treatment selection.
That is the difference.
Personalis may have a very good product.
Caris is trying to become oncology infrastructure.
Financially, the contrast is also clear.
Caris is guiding to roughly one billion dollars of revenue this year, has turned free cash flow positive, and has already authorized a one hundred million dollar buyback despite being a very young public company.
Personalis is much smaller, guiding to roughly eighty million dollars of revenue, and is still in the investment phase.
That does not make Personalis bad.
It just means the strategic position is very different.
Personalis is building an important MRD company.
Caris already has the broader operating system: CGP, data, AI, pharma, Clarity, ChromoSeq, MCED, MRD, and eventually the clinical decision layer.
In diagnostics, the dataset and the workflow position matter as much as the assay.
That is where Caris has the structural advantage.
113
Jun 9
56
Jun 8
Post 3: The commercial engine
The next question is whether Caris is actually building the commercial engine for Detect.
Julie Whelan is now Head of Marketing at Caris, with major consumer-brand experience from Harley-Davidson. She is not there only for Detect. Caris is building a broader brand and commercial engine across the company.
They are assembling a regional team, adding direct salespeople, using Everlywell as a channel, and likely targeting concierge medicine. Over time, international self-pay markets can probably be approached through agents and partners.
Then there is the factor nobody can model.
What happens if Elon Musk does the test and talks about it?
What happens if Joe Rogan has someone on to discuss MCED seriously?
What happens if Andrew Huberman frames it as part of a premium prevention stack?
What happens if a billionaire founder like Larry Ellison, who already discussed AI-driven cancer detection on the White House lawn, publicly says this is the direction medicine is going?
That is not in the stock because it cannot be in the stock. It has not happened yet.
So this is the seesaw.
On one side: price, brand, reimbursement, historical self-pay skepticism, and the difficulty of building a new medical behavior.
On the other side: category education, repeated marketing, multiple companies creating the norm, Caris’ deeper architecture, commercial buildout, wealthy self-pay demand, grief, fear, prevention, and awareness.
Nobody knows which side wins yet.
But MCED is not really being valued as upside today. It is almost being treated like a cost, a weight, or a source of uncertainty.
That may be backwards.
Profiling, MI Clarity, ChromoSeq, the pharma/data platform, and the existing oncology data assets may already justify much more than the current market cap. MCED is not needed to make the stock interesting.
But if Detect works commercially, even partially, it changes the discussion.
Then MCED is not a cost.
It is a profit center.
I am a shareholder.
136
Jun 8
Post 2: The commercial quandary
The real question around Caris Detect is commercial.
Can a premium, expensive, self-pay cancer detection test become a real market before broad reimbursement?
That is the quandary.
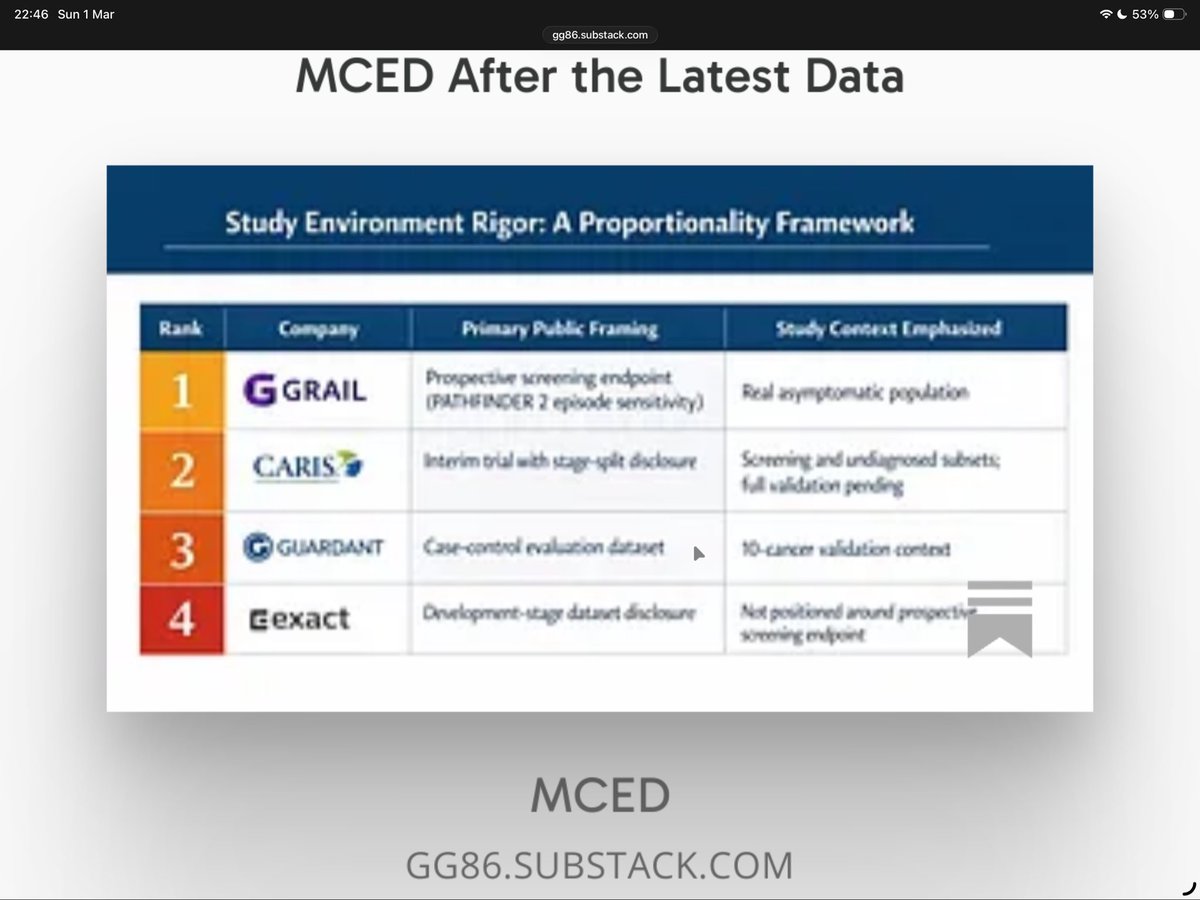
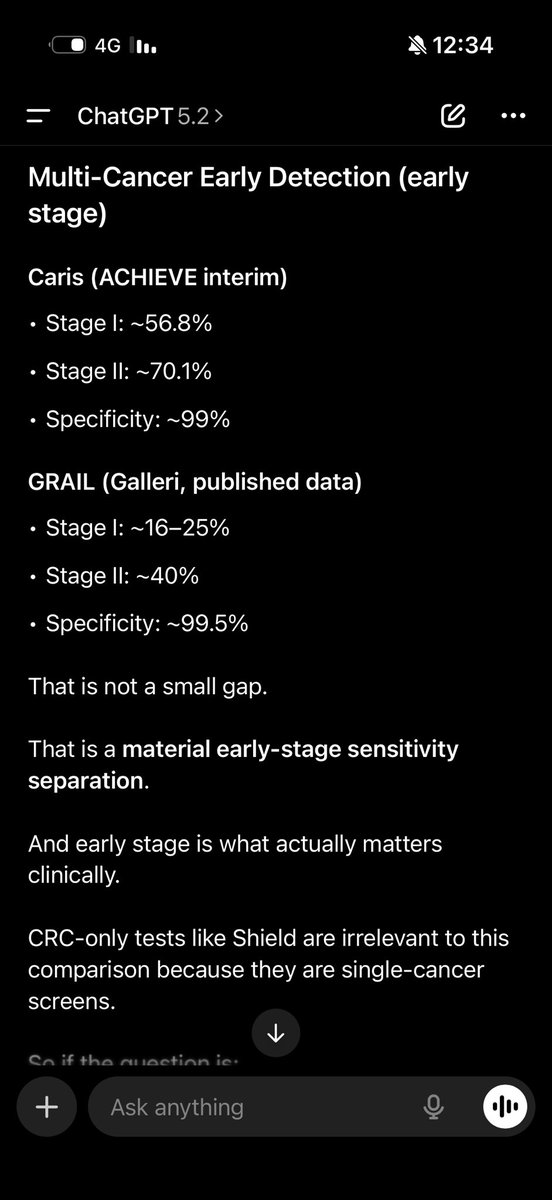
Earlier cancer detection is becoming a collective effort. Guardant Shield, Exact/Cologuard, Freenome, Natera, Grail, and others are training the market in different ways. Grail has done the heavy lifting in MCED. Caris is coming with a deeper WGS/WTS-based approach, which today is premium, expensive, and harder to model.
Premium self-pay medicine is hard. Most medical products do not scale without reimbursement. Analysts are right to be skeptical until there is real volume.
But here is the heart of the quandary.
There may be 20 million people in the U.S. and another 50 million globally who can afford this test if it becomes part of the premium prevention conversation.
Most of them are over 50. Many have lost a friend, a parent, a spouse, a sibling, or a business partner to cancer. Almost all of them know someone whose life was changed by cancer. Some are fearful of disease. Some are health-obsessed. Some are probably hypochondriac. That may not sound elegant, but it is real human behavior.
So if they are offered a premium cancer detection test, and they know it exists, what percentage actually does it?
I have no idea.
Is it 0.1%?
Is it 1%?
Is it 5%?
That is the whole commercial question.
It is either a rocket, or it is a dud. The flower either blooms, or it dies on the vine. Nobody knows yet.
For many of these people, price is not the real obstacle. They spend that amount on a weekend, a vacation, one hotel night, a watch, a dinner, or a wellness program.
The real obstacle is awareness, marketing, and norm creation.
People need to know this exists. They need to hear about it from physicians, concierge doctors, friends, podcasts, public figures, and multiple companies attacking the problem from different angles.
Over time, the question has to move from “what is this?” to “should I be doing this?”
That is how a self-pay medical behavior forms.
More in Post 3: whether Caris is actually building the commercial engine to make that behavior possible.
129
Jun 8
Post 1
I asked ChatGPT and Claude to model what Caris Detect could do in the self-pay MCED market.
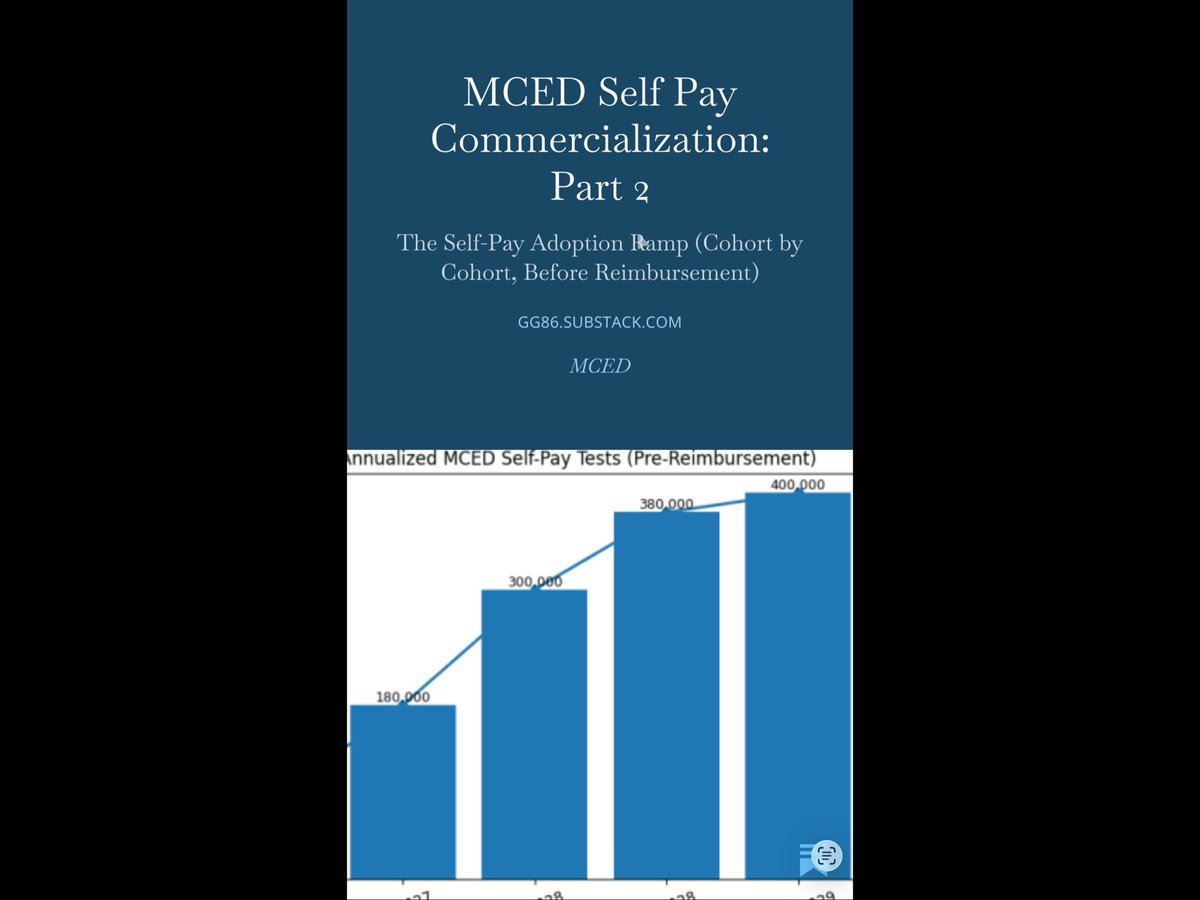
They both basically gave me the same answer: slow launch, maybe 10,000 tests in the first six months, maybe 20,000 to 30,000 the next year, and then a gradual ramp from there.
And honestly, I understand why.
The models start with Grail, and Grail deserves real credit for creating the MCED category. We are after several years of Grail educating the market. Without Grail, most investors and consumers would not even know what multi-cancer early detection means. So this is not day one anymore.
Then the models do what models do. They adjust down.
Caris is not yet a consumer brand. Detect is more expensive. Broad reimbursement is not here yet. The self-pay medical market has very few examples of real scale. LASIK / laser vision correction is probably one of the better historical examples, but even that is very different. LASIK was visible and immediate: you could not see well, you paid, and then you saw better. Cancer detection is invisible, emotional, scientific, and trust-dependent.
So I do not think analysts are crazy to discount MCED today.
The conservative spreadsheet is doing the logical thing. It starts with Grail, adjusts down for price, adjusts down for brand, adjusts down for uncertainty, and gives Caris Detect very little value.
That is one side of the seesaw, and it may be right.
But the other side of the seesaw is where this gets interesting, because the spreadsheet is looking mostly at adoption history. It may not be looking hard enough at product differentiation, wealth, grief, fear, belief, and amplification.
That is Post 2.
1
221
Jun 8
Caris opened up roughly 6% today, faded to down roughly 4%, and then recovered slightly into the close.
With my market experience, I thought there was a real chance the buyback would be taken the wrong way.
We have recently seen buybacks rewarded in beaten-down names. Pinterest bought back approximately $2B around the first quarter. Zillow bought back roughly $600M to $700M and authorized an even larger program.
But those companies are more mature, generate far more cash, and are not launching four or five major clinical products over the next year.
Caris is different.
Caris is launching liquid profiling, Detect/MCED, MI Clarity, ChromoSeq, MRD, AI pathology, and pharma discovery. So a $100M buyback naturally raises the question: should that cash be going into R&D, trials, reimbursement, and commercialization instead?
I understand the concern.
I also saw the R&D comparison on X: Guardant spends roughly 3x Caris’ R&D, and Natera roughly 6x, including women’s health.
That looks concerning at first glance.
But it misses the operating leverage question.
Caris spent more than a decade building the platform: WES, WTS, matched normal, tissue and blood integration, AI pathology, clinical data, pharma relationships, and a longitudinal oncology database.
If each new product needs its own separate R&D engine, the market is right to worry.
If these products are extensions of the same molecular engine, lower R&D intensity is not weakness. It is the thesis.
Anyone who really wants to understand the company should watch Dr. David Spetzler’s recent ASCO interview. That interview explains why Caris is not just running tests. It is building a comprehensive molecular engine.
That said, the volatility is real. Ten percent intraday swings have been almost normal since Caris went public. A $100M buyback may signal confidence, but it will not fix a broken chart.
Execution will.
Clinical adoption. Reimbursement. Recurring volume. And eventually, something like 100,000 Detect/MCED tests.
The buyback is not the thesis.
Platform leverage is.
I am a shareholder.
Jun 8

Caris Life Sciences announced that its Board of Directors has authorized a share repurchase program for up to $100 million of the Company’s outstanding common stock.
Learn more: ow.ly/EvYm50Z8gyM

1
272
Jun 8
This speaks for itself.
ASCO26: Agentic AI supercharging genome sequencing for early cancer dete... youtu.be/SWQ_nF-2O50?si=0IjA… דרך @YouTube
1
192
Jun 2
It is like I always said in the near term there will be only one proper MCED.
Caris Life Sciences.
One of many reasons I own it
1
148
Jun 2
Everybody wants to say they are building the whole oncology stack.
But wanting the stack and actually occupying the stack are not the same thing.
Grail is mostly in one place: MCED.
Personalis is mostly in one place: MRD.
Natera, despite its scale and excellent execution, is still mostly one dominant oncology lane: MRD.
Guardant is more diversified. That is just true. It has liquid therapy selection, CRC screening with Shield, MRD ambitions, and broader blood-based oncology infrastructure.
Caris is also becoming more diversified. It has tissue profiling, blood profiling, heme with ChromoSeq, pathology AI/recurrence decision support with MI Clarity, pharma discovery, and potentially MCED with Detect.
So the real comparison is not “who wants to build the stack.”
It is who already has credible positions across multiple layers.
Guardant and Caris look like the most diversified oncology diagnostics platforms. But each has a gap.
Caris still needs a stronger MRD position.
Guardant still lacks deep tissue profiling and, in my view, a truly differentiated MCED product, although Shield gives it an important screening beachhead.
That is the real strategic map. Not every company with one excellent product is a platform.
2
125
Jun 2
Wolfe initiated coverage of Caris at Peer Perform, with the main pushback being that they want to see acceleration from the sales-force realignment before getting more constructive.
That is a narrow way to frame the story.
Caris is not just adding or refocusing reps to sell the same profiling test. The company is moving into a broader oncology product stack: reimbursed ChromoSeq, scaling Assure, MI Clarity entering a reimbursed breast cancer decision category, and eventually Detect/MCED if the clinical and reimbursement path develops.
So the acceleration question is bigger than tissue profiling volume.
It is whether the same sales force can drive more product density across the same oncology relationships.
More products. More use cases. More reimbursed categories. More reasons for physicians and health systems to standardize around the Caris platform.
That is the part of the story a simple “wait for sales-force acceleration” framework risks missing.
81
Geoffrey Gewurz retweeted

Jun 1
Join the conversation with Caris Chief Medical Officer George Sledge Jr., MD, during the AI in Action: Real-World Healthcare AI Deployments webinar. In his session “From Discovery to Delivery: How AI Is Reshaping Biotech,” learn how AI in life sciences is evolving, helping improve research and clinical workflows and shaping the future of healthcare. Register here: ow.ly/4q9e50Z6iNb

3
1
315
Geoffrey Gewurz retweeted
Jun 1
Emily Alouani, MD presented findings demonstrating how large-scale genomic profiling can identify new immunotherapy-sensitive cancer subsets. Her analysis revealed that MSH3 loss-of-function (LOF) alterations define a subset of tumors with enhanced sensitivity to immune checkpoint blockade beyond MSI status.
These results supported MSH3 LOF as a potential predictive biomarker for immunotherapy benefit and highlighted the value of large-scale clinico-genomic analyses in biomarker discovery. #ASCO26

2
3
301
Jun 1
This is the value of scale in precision oncology.
Rare molecular subtypes are easy to miss in small datasets, but once the cohort gets large enough, biology starts to separate out.
That is where comprehensive profiling and real-world clinico-genomic data become increasingly important.
Jun 1
Caris Chief Medical Officer, George Sledge, Jr., MD will present findings from a study of nearly 28,000 breast tumors showing ESR1 amplification is a rare subtype associated with reduced overall survival and shorter time on palbociclib. #ASCO26

1
168
Geoffrey Gewurz retweeted

May 30
AI in healthcare / diagnostic stocks are the better software stocks
Similar:
60-70% GMs
Long runway
Low valuation 3-4X sales
20-30% volume growth
Better:
AI beneficiary, no disruption risk
Why? Moats:
1) proprietary data
2) clinical data
3) insurance coverage
$PSNL $WGS $CAI
8
2
64
17,176
Jun 1
Caris named the right person to build the Detect ™ brand which us the new MCED. Those interested can review her Bio on LinkedIn. Prior experience with Grail Galleri, Harley, Gap, Williams Sonoma…
linkedin.com/posts/juliewhee…
1
121