
Pulmonary and Critical Care Medicine Point Of Care Ultrasound (POCUS) education by @Edwin_J_Jr. RDCS & NBE CCE & ccTEE Diplomate
Joined May 2022
- Tweets 1,411
- Following 278
- Followers 4,395
- Likes 1,974
316 Photos and videos












Pinned Tweet

11 Jun 2025
What is the short clip challenge? Check out this clip from our 2024 @IUSMDeptMed Grand Rounds. Are you ready to take the challenge? sign up here-->pulmonarypocus.com/contact-u…
@NephroP @IUPCCM @OSUPCCM_Fellows @accpchest @POCUSJournal
3
11
5,038
Pulmonary-POCUS retweeted

Jun 13
Thanks for having me!
Jun 13

EMCrit 427 - Advancing Concepts in Shock Physiology. As an intro to a 3-part series, I go over two papers discussing new ways to assess and understand shock hemodynamics.
(@emnerd, @thinkingcc, @saracrager)
[#MembersOnly]
emcrit.org/427

1
11
45
8,283
Pulmonary-POCUS retweeted

Jun 11
@DanRozenbaum
Curious on what you think. I thought this was early cycle dyssynchrony. Tried to increase I time but did not help. Increased opioid infusions but did not help.
1
2
7
554
Pulmonary-POCUS retweeted
What an honor to receive the Golden Lung Teaching Award from our graduating Indiana University PCCM/CCM fellows!
Teaching mechanical ventilation and critical care to this incredible group has been an absolute privilege. Thank you for this recognition!

2
2
33
1,685
Jun 7
Congratulations to this week's short clip challenge winner Maya Haouili, from IU IM residency! Congratulations Maya, enjoy a cup of coffee on us!
Here's a quick recap of last week's metrics:
We received 97 responses.
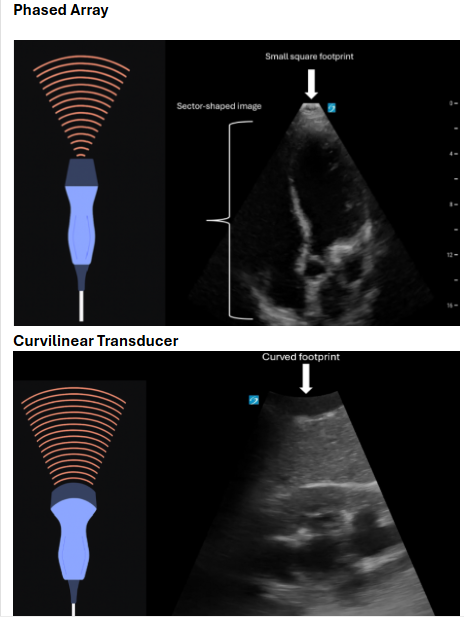
Question 1: You are visualizing a pleural effusion. Looking at the footprint of the probe, which transducer is being used?
Answer 2 The correct answer is the phased array transducer. 40% of respondents answered this question correctly.
Question 2: What structure is the white arrow pointing towards?
Answer 2: The correct answer is the diaphragm. 98 % of respondents answered this question correctly.
Key points:
See all Key points here—> pulmonarypocus.com/short-cli…
1
3
13
871
Pulmonary-POCUS retweeted

Jun 6
Interesting and scary #echofirst image (TEE)
A case of infective endocarditis caused by Tropheryma whipplei.
#POCUS #FOAMed
From 🔗 IDCases. 2023;32:e01800. doi: 10.1016/j.idcr.2023.e01800.
4
49
183
21,788
Pulmonary-POCUS retweeted
Jun 1
Hepatic vein Doppler waveform components explained.
#POCUS #VExUS #Nephpearls
🔗youtu.be/7KII6btTGJ8?si=YsnK…
38
110
14,562
Pulmonary-POCUS retweeted
May 31
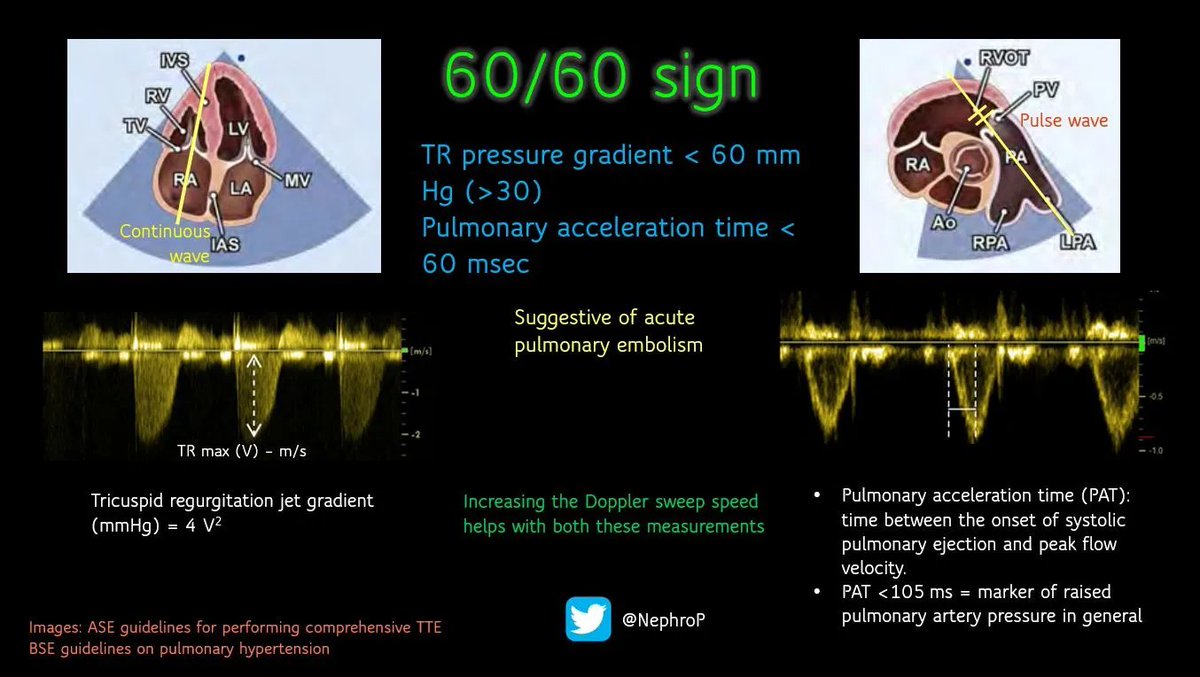
The 60/60 sign is a cardiac #POCUS finding used to support the bedside diagnosis of acute pulmonary embolism. It refers to the simultaneous presence of two measurements, both involving the number 60.
RV outflow tract (RVOT) acceleration time ≤60 ms - This is the time from the onset of blood flow through the pulmonary valve to its peak velocity. In acute PE, the sudden obstruction causes blood to accelerate and decelerate abnormally fast, producing a "truncated" or shortened flow profile.
Pulmonary artery systolic pressure (PASP) ≤60 mmHg (but >30 mmHg) - estimated via the tricuspid regurgitation jet.
In acute PE, the thin-walled right ventricle cannot generate very high pressures because it has not had time to adapt. A PASP above 60 mmHg suggests a chronic process (e.g., chronic pulmonary hypertension) where the RV has hypertrophied over time
2
29
131
5,323
Pulmonary-POCUS retweeted

In patients with a left-to-right shunt across a PFO undergoing OPCAB, intermittent apnea used to optimize surgical exposure may induce RV dysfunction and subsequent shunt reversal, resulting in worsening hypoxemia. #echofirst 👉 TEE is crucial
What about the last 2 🎞️ (ACT 300)?
5
17
79
7,120
Pulmonary-POCUS retweeted

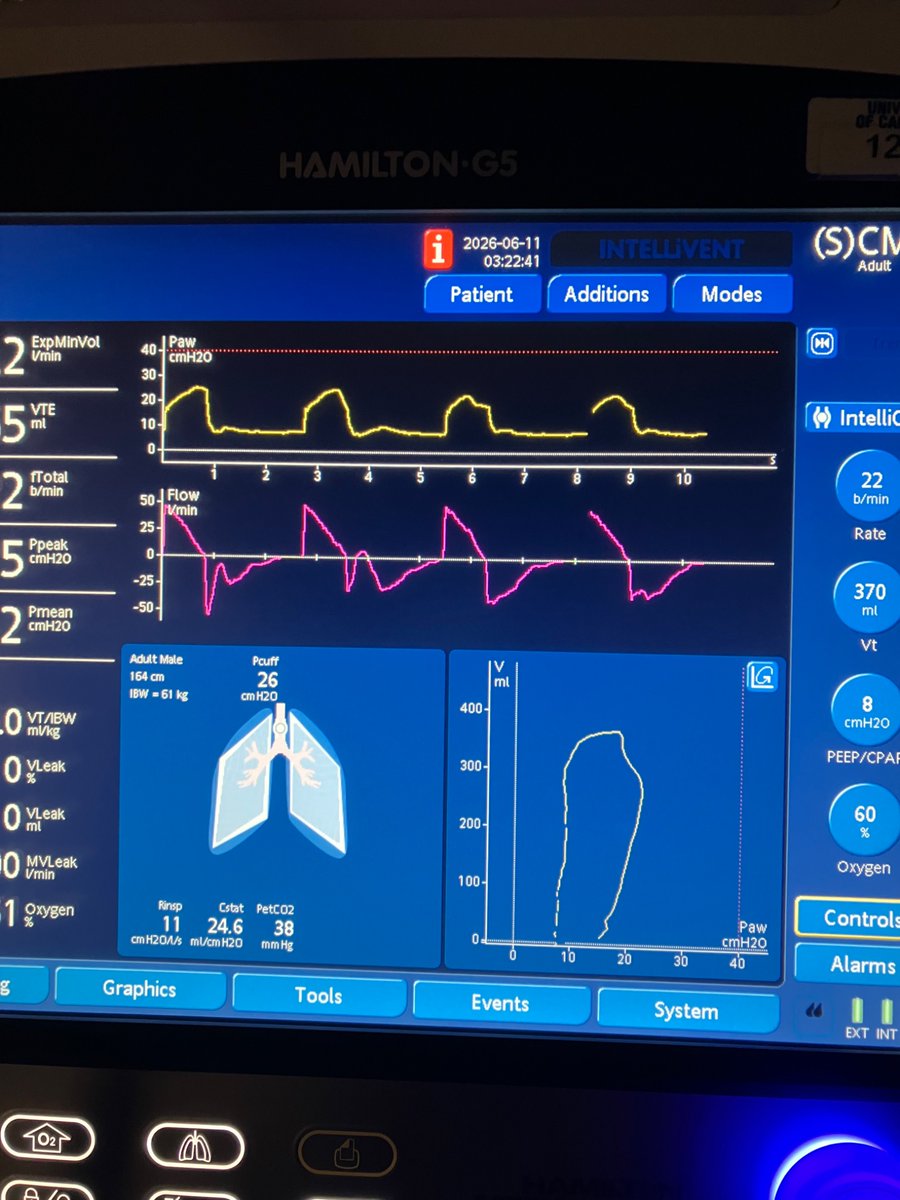
May 27
Teaching point:
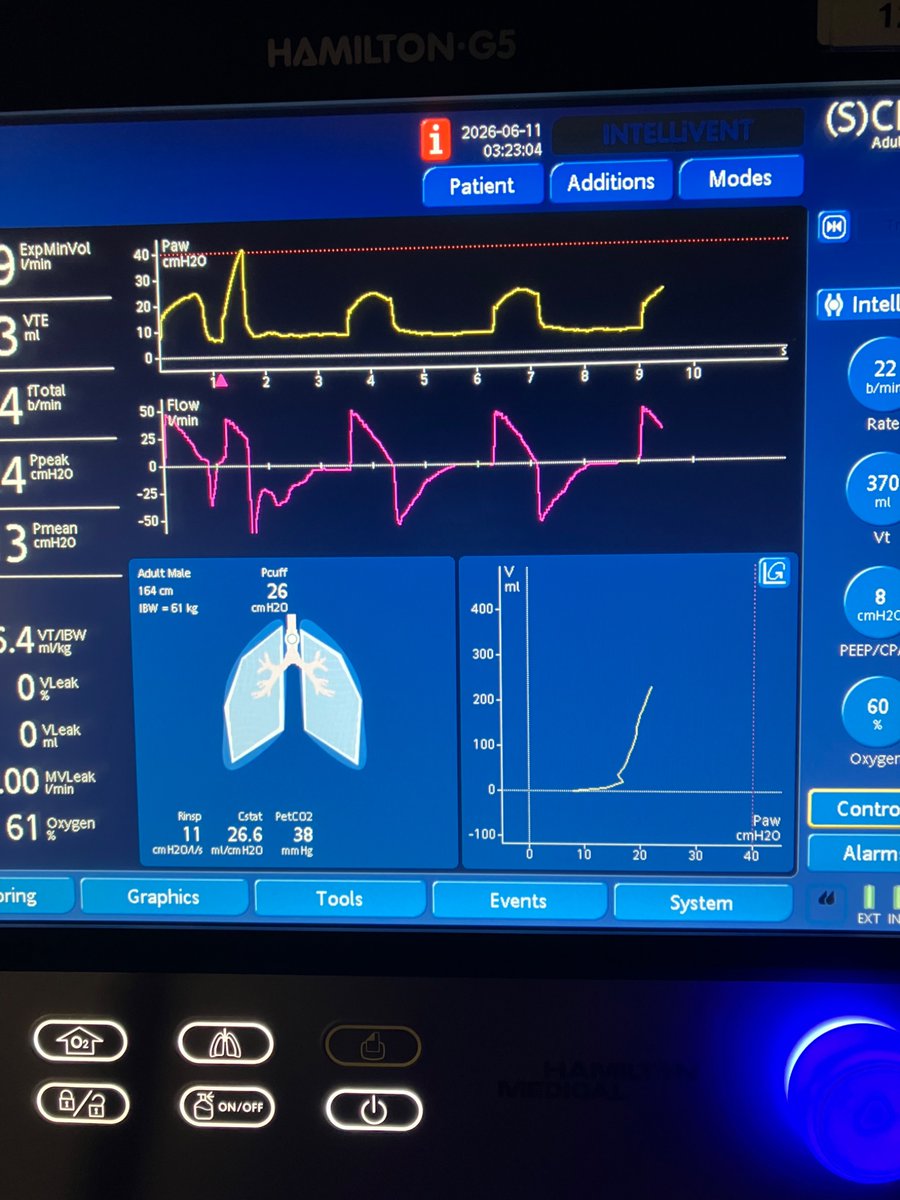
If tidal volumes are constant between the two measurements, the PEEP associated with the best static compliance is the one associated with the lowest driving pressure. Titrating to best static compliance vs to driving pressure becomes semantics.
However, if tidal volumes change between measurements, you can’t look at the driving pressure alone (the driving pressure is associated with BOTH static compliance AND tidal volume).
If your patient is on Pressure Control, like the one above, and the increase in PEEP worsens static compliance, tidal volumes will drop for the same applied inspiratory pressure. In a case like this, you MUST look at the static compliance!
We did insp and exp holds to calculate static compliance and got:
At a totPEEP of 12: 317/(32-12) = ~16ml/cmH2O
At a totPEEP of 15: 272/(34-15) = ~14ml/cmH2O
Since compliance was better at a PEEP of 12, we kept it as our ideal PEEP.
3
6
21
1,270
May 28
1/2 Congratulations to this week's short clip challenge winner Raul Gregg from IU Internal Medicine! Congratulations, Raul, enjoy a cup of coffee on us!
Here's a quick recap of last week's metrics: We received 102 responses.
Answer 1: The correct answer is the Inferior Vena Cava. 87% of respondents answered this question correctly.
Answer: 2 The correct answer is guidewire migration into the IVC, pull the wire back and continue the procedure. 85% of respondents answered this question correctly. @NephroP
1
11
2,011
May 28
2/2
Key points
1.The SVC sits directly above the IVC anatomically. During central line placement, the guidewire will often pass from the SVC into the right atrium and then straight down into the IVC. This can be seen in real time using a subxiphoid short-axis (“snail”) view.
2.This same pathway is used in several VV ECMO cannulation strategies. In the Avalon technique, a guidewire is advanced from the right internal jugular vein into the IVC, followed by sequential dilation and placement of the Avalon cannula with the distal port in the IVC and the middle port directed toward the tricuspid valve. ( see below)
Avalon cannulation technique.A: Guidewire is placed to the inferior vena cava from right internal jugular veinB: Sequential dilatation of the access site is doneC: The Avalon cannula is placed with distal port in the inferior vena cava and middle port facing to the tricuspid valve
Shaheen, Aisha & Tanaka, Daizo & Cavarocchi, Nicholas & Hirose, Hitoshi. (2016). Veno-Venous Extracorporeal Membrane Oxygenation (V V ECMO): Indications, Preprocedural Considerations, and Technique. Journal of cardiac surgery. 31. 10.1111/jocs.12690.
3. As you perform more POCUS-guided procedures, you will occasionally see PICC lines and guidewires end up in the IVC. One study showed that during standard central venous catheter insertion, about one-third of guidewires migrated into the IVC. Importantly, wires in the IVC often do not produce ectopy or arrhythmias. Because of this, the absence of arrhythmias should never be used to confirm appropriate wire position. The side or site of insertion also does not predict whether the wire will enter the IVC versus remain in the right heart.
pulmonarypocus.com/short-cli…
5
406
Pulmonary-POCUS retweeted
May 27
KEY CONCEPT and a tricky question:
Was the increment in PEEP from 12 to 15 beneficial from a respiratory mechanics standpoint? Answer below.


3
23
68
6,882
May 26
You have placed the guidewire for a CVC, you view the vessel below and see the wire in the lumen, How did this occur and what is your next step?
Take the full challenge here-->pulmonarypocus.com/short-cli…
@NephroP
3
4
20
10,734
Pulmonary-POCUS retweeted
May 19
I’m honored to have my video on end-inspiratory transalveolar pressures selected as a finalist for the ATS Teaching Competition. Congrats to Dr. Wang for winning the competition!
I’ll do my next post on end-inspiratory transalveolar pressures to bring some of the video to X!


2
2
20
1,221
May 17
🏆 Huge congratulations to Mitchell Holland from ISUM School of Medicine, our winner for Short Clip Challenge Week #103! Enjoy a $5 Starbucks coffee on us! ☕
We received 89 responses this week!
The correct answers were
1) Aorta
2) Aortic Dissection.
An aortic dissection occurs when there is bleeding within the medial layer of the aorta, most commonly due to intimal tearing and separation.
Click here for full explanations: pulmonarypocus.com/short-cli…
1
5
549
Pulmonary-POCUS retweeted
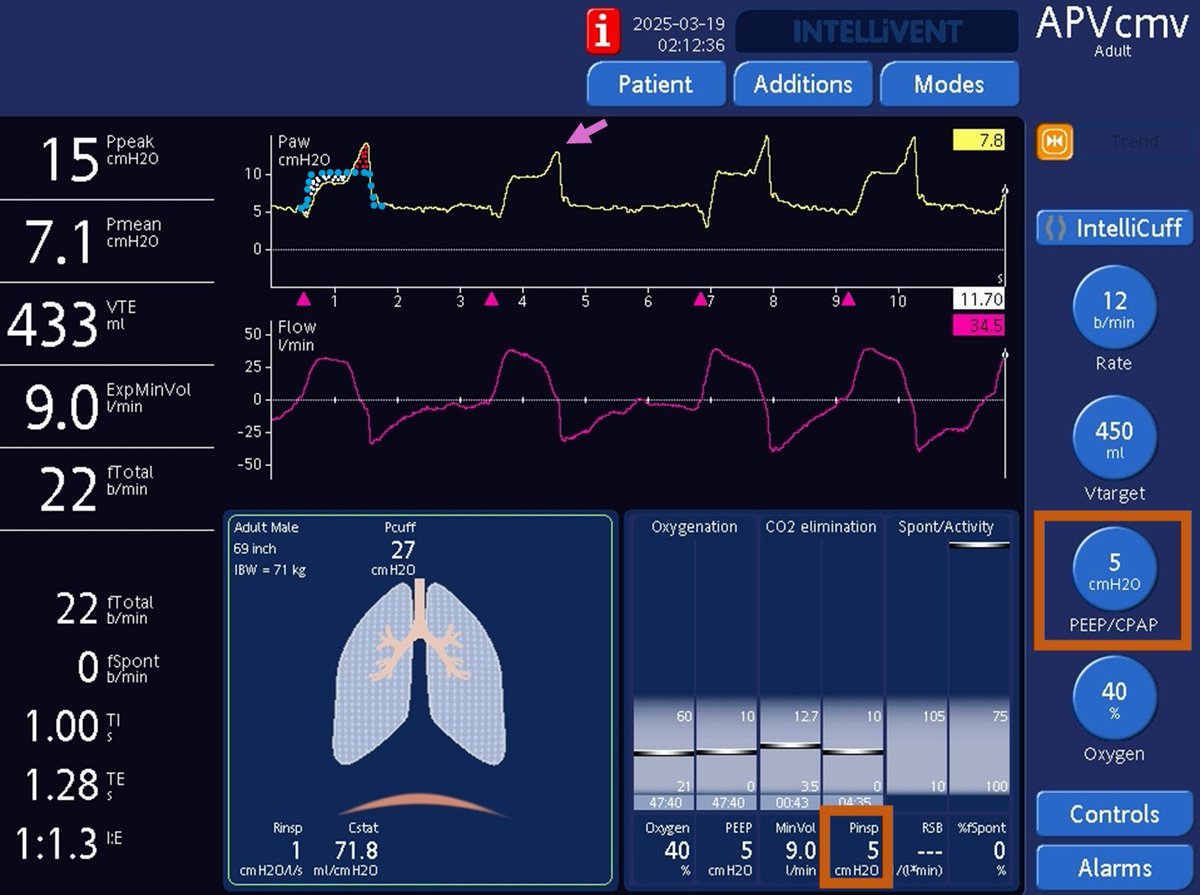
May 13
KEY CONCEPTS: Why does auto-PEEP lead to failed trigger events and why does raising set PEEP treats it?
In the pictures below, raising PEEP from 5 (left) to 10 (right) abolished the failed trigger events. Let's truly understand why!


2
25
104
7,000
May 12
Calling all POCUS enthusiasts! 🩺🎥 Join our weekly Short Clip Challenge released every Tuesday at 7:00 AM.
Watch a brief ultrasound clip, answer two questions, and the first to get both right wins a $5 Starbucks gift card! ☕
You also earn 0.25 AMA PRA Category 1 CME credits for each quiz!
Q# 1 what vessel is the arrow pointing towards?
Test your skills here 👇Select week # 103
pulmonarypocus.com/short-cli…
#POCUS #Ultrasound #MedEd #ShortClipChallenge #MedTwitter
1
1
9
546
Pulmonary-POCUS retweeted
Which DYSSYNCHRONY do you see here?
Please find a detailed waveform analysis below.
3
17
102
10,434
May 3
1/1: Congratulations to this week's SCC winner Tanner Course from IUSM IM-Peds
Congratulations Tanner, enjoy a cup of coffee on use
Here is a look at this weeks metrics
We have 122 responses
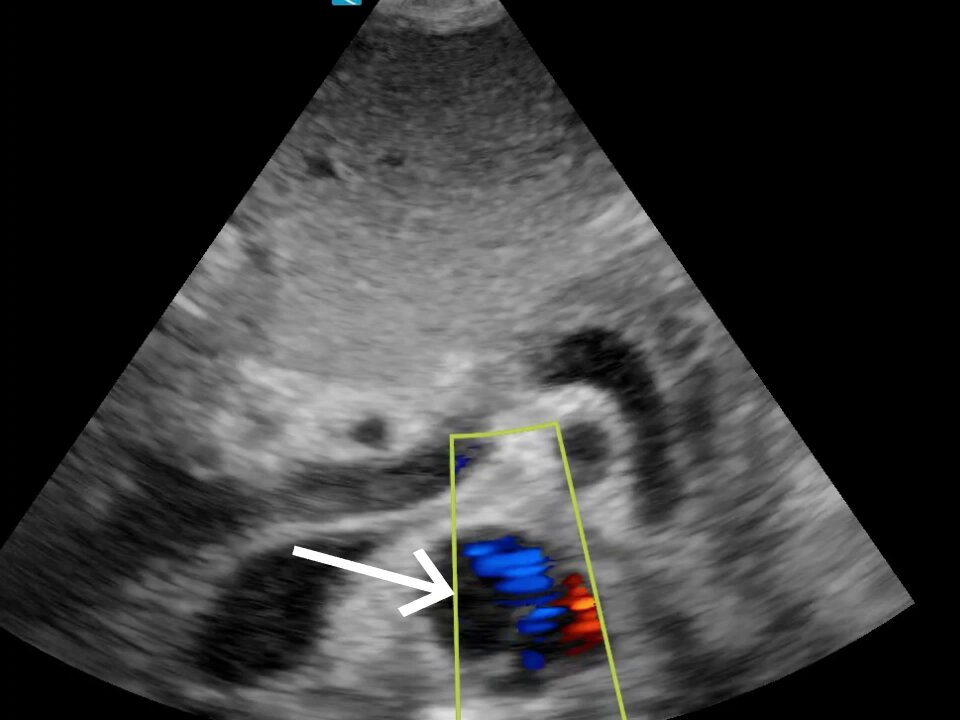
Q#1 You are performing a suprapubic ultrasound to evaluate decreased urine output in a cirrhotic patient with an indwelling Foley catheter. A nursing bladder scan estimates ~300 mL of urine. What is the white arrow pointing to?
A#1: Ascitic fluid
1
2
11
1,139
May 3
2/2
Q#2:Given the ultrasound findings and discrepancy with the bladder scan, what is the most likely explanation for the patient’s decreased urine output?
A#2 Ascites falsely elevating bladder scan volume
See the explanation here--->pulmonarypocus.com/short-cli…
208