
The Internal Medicine Residency Program at Medstar Georgetown/ Washington Hospital Center
Joined October 2020
- Tweets 451
- Following 263
- Followers 1,532
- Likes 185
216 Photos and videos












Pinned Tweet

Mar 20
Overjoyed to welcome these incredible people to our Internal Medicine family! We can’t wait to start this journey together—see you in July!

1
10
58
7,702
May 20
Your quick guide to reading PFTs made by one of our PCCM enthusiasts
1
205
May 19
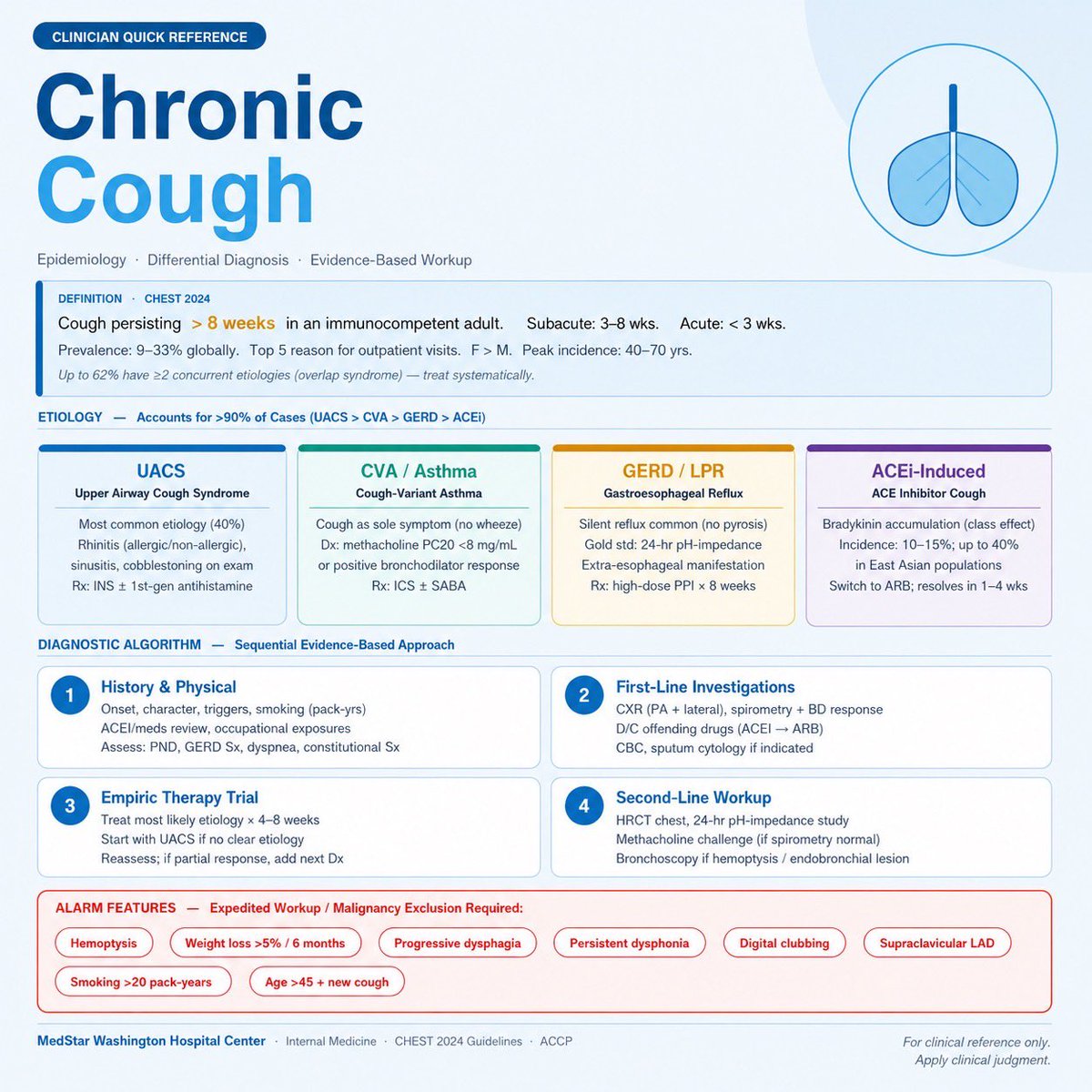
When cough becomes chronic, structure beats speculation- here’s a quick reference sheet made by one of our residents
1
1
139
May 18
This evidence-based guide breaks down the Surviving Sepsis 2026 bundle: from fluids and vasopressors in the first hours to antibiotics, source control, and adjunctive thresholds every clinician needs to know.
3
105
MWHC IM Residency retweeted

May 12
We’ve all spent hours debating volume status at the bedside and it’s still one of the hardest things to assess in medicine. A quick visual summary of how physical exam findings, POCUS, and BNP perform for identifying (and ruling out) volume overload #MedTwitter

1
2
131
May 12
The Renove Trial was completed to assist in understanding what clinicians should consider for patients with high VTE recurrence risk. It showed low dose DOACs were noninferior to full dose DOACs in preventing future VTEs. 1/2
1
238
May 12
ATLS has come out with some new key takeaways to help with management of massive hemorrhage. A key difference is the x-ABCDE focus on stabilization that emphasizes stopping the “eX-sanguinating bleed” first before ensuring an airway.

77
MWHC IM Residency retweeted

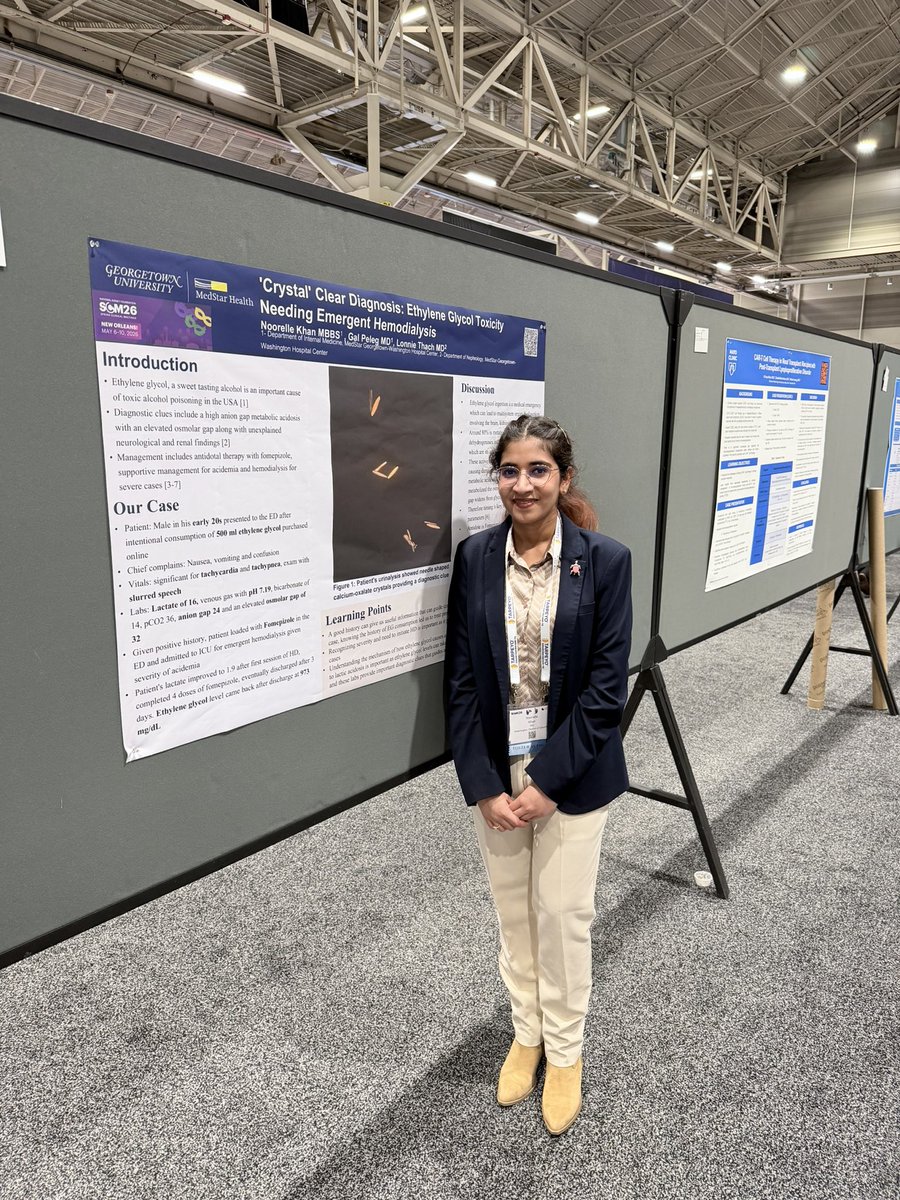
Delighted to present our clinical case report at the National Kidney Foundation Spring Clinical Meeting 2026! Inspired by the ground breaking research transforming kidney care!
#NKFSCM2026 @nkf
1
5
308
MWHC IM Residency retweeted

A quick infographic to review the new PE guidelines 🫀

1
5
143
May 4
Cardiogenic vasodilatory shock, a complex, high-stakes phenotype requiring careful hemodynamic assessment and tailored management.
Key concepts and clinical approach informed by JACC's State-of-the-Art Review.
A quick, high-yield review #MedTwitter #CardioTwitter
176
MWHC IM Residency retweeted


2
7
326
MWHC IM Residency retweeted

Autoimmune hepatitis can masquerade as many things! Recognizing the clues early matters. A tweetorial on diagnosis, pitfalls, and management pearls. 🧵 #MedTwitter #LiverTwitter #Hepatology

2
4
203
MWHC IM Residency retweeted

Apr 27
Initiation of NB therapy during index HM3 LVAD implant associated with improved survival, a finding that needs to be prospectively studied @FlaviaTejadaF @fsheikh22 @RichaGuptaMD @MedStarHealth @GTCardFellows @IMMWHC onlinelibrary.wiley.com/doi/…
3
6
447
Apr 22
Excellent grand rounds by one of our General Internists Dr. Mueller!
4
267
Apr 9
Such a fun morning report!!

Today, I presented a case of pyogenic liver abscess with transdiaphragmatic extension and concurrent lung abscess due to Streptococcus intermedius. Was nervous but excited to talk through such a cool case!
2
435
Apr 7
🫁 Your patient has dyspnea on exertion. The echo report says "PASP 52 mmHg - consider pulmonary hypertension."
But does that mean they have PH?
Not necessarily. Here's what echo can (and cannot) tell you. 🧵 #MedEd #Cardiology #Pulmonary
1
4
996
Apr 7
PH is classified into 5 WHO Groups:
1️⃣ PAH (idiopathic, CTD, drugs)
2️⃣ Left heart disease ← common
3️⃣ Chronic lung disease/hypoxia
4️⃣ CTEPH
5️⃣ Multifactorial
Why does this matter? Because Group 2 & 3 do NOT get PAH therapy. Getting the group right changes everything
7
187
Apr 7
🏠 Take-home:
1. Echo gives a PASP estimate, not a diagnosis
2. Use ESC probability (Low/Intermediate/High)
3. Normal echo does NOT rule out PH if suspicion is high
4. RHC is required to confirm dx, measure PVR, and classify hemodynamic profile
70
Apr 7
So, what do you do with an abnormal echo?
Clinical suspicion → 🔬 TTE → Low prob: look for alternatives → Intermediate/High: V/Q scan → ➡️ Right Heart Catheterization
Echo probability guides who goes to cath - not whether PH exists.
52
Apr 7
The overdiagnosis problem is real.
When borderline elevation on echo is compared to invasive mPAP?
~50% correlation.
High PASP on echo alone ≠ PH diagnosis. It's an indication to look further - not a diagnosis to hang your hat on.
Fisher MR doi.org/10.1164/rccm.200811-… PMID 19164700
1
87
Apr 7
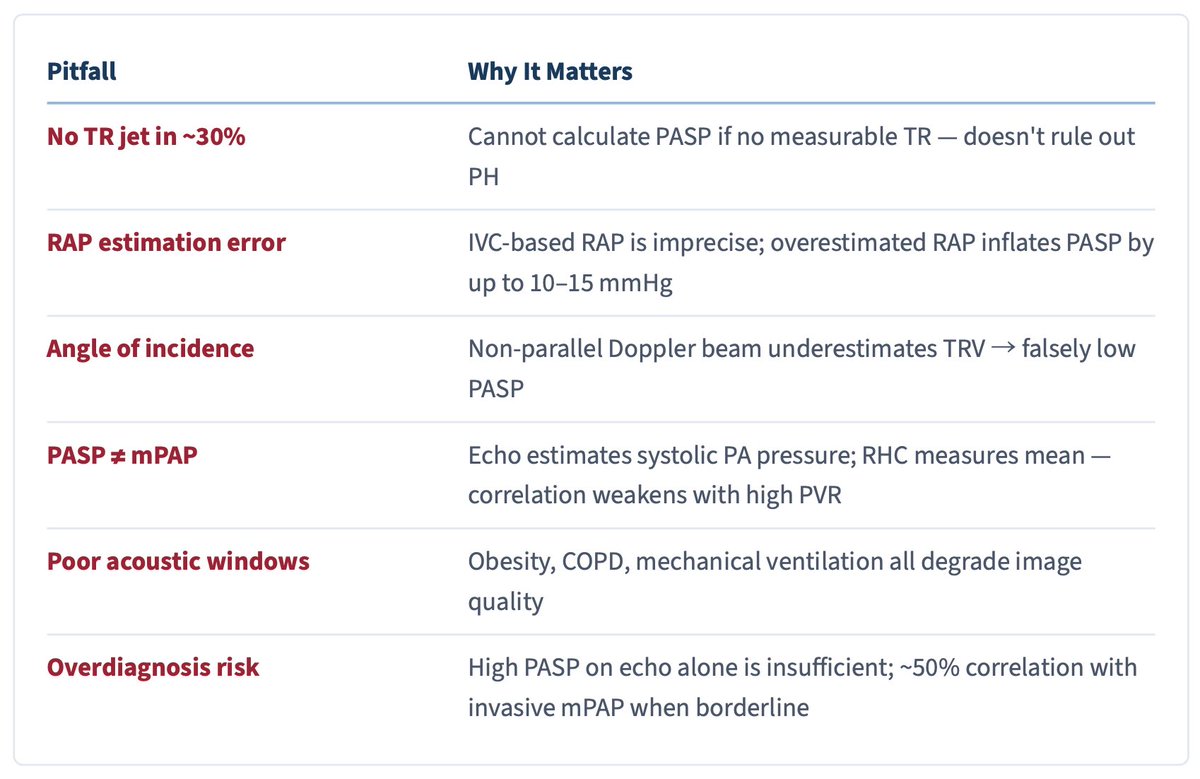
However, Echo lies. Here are some of the ways how:
❌ No TR jet in ~30% of patients → can't calculate PASP (absence ≠ no PH)
❌ IVC-based RAP overestimates by up to 10–15 mmHg
❌ Non-parallel Doppler beam → underestimates TRV
❌ PASP ≠ mPAP - they diverge as PVR rises
43
Apr 7
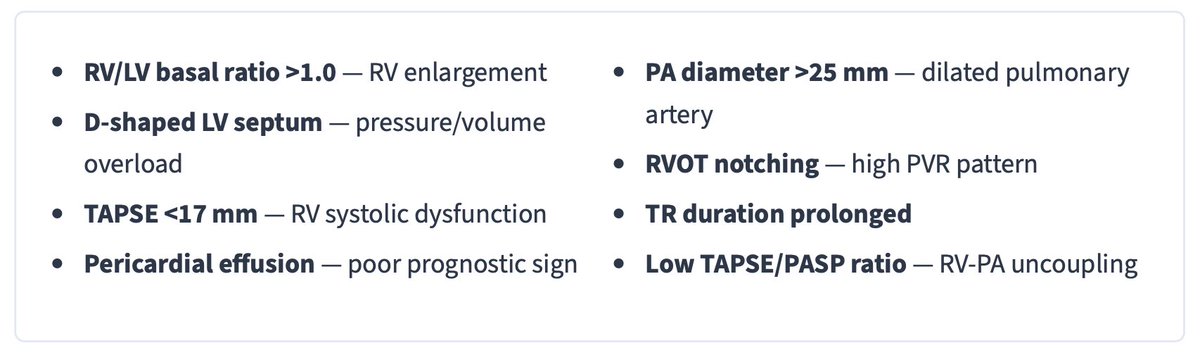
Beyond TRV, look for these RV stress signals:
📏 RV/LV basal ratio >1.0 → RV enlargement
🫀 D-shaped septum → pressure/volume overload
📉 TAPSE <17mm → RV systolic dysfunction
💧 Pericardial effusion → poor prognostic sign
📊 Low TAPSE/PASP ratio → RV-PA uncoupling
1
88
Apr 7
The 2022 ESC/ERS Guidelines moved away from a single TRV cutoff.
Now we use echo probability categories (TRV signs):
✅ TRV ≤2.8 no signs → Low
🟡 TRV ≤2.8 signs OR 2.9–3.4 → Intermediate
🔴 TRV ≥3.4 → High
"Signs" = RV dilation, D-septum, TAPSE <17mm, PA dilation
58