
Joined February 2018
- Tweets 5,258
- Following 316
- Followers 1,262
- Likes 13,328
151 Photos and videos









Pinned Tweet

14 Mar 2025
If you've done MBBS :You are in top 0.1% of the population
If you've done MD after MBBS: You are in the top 0.01% of the population
If you've done DM after MD,MBBS: You need to get a life
31
106
1,490
95,201
Jun 2
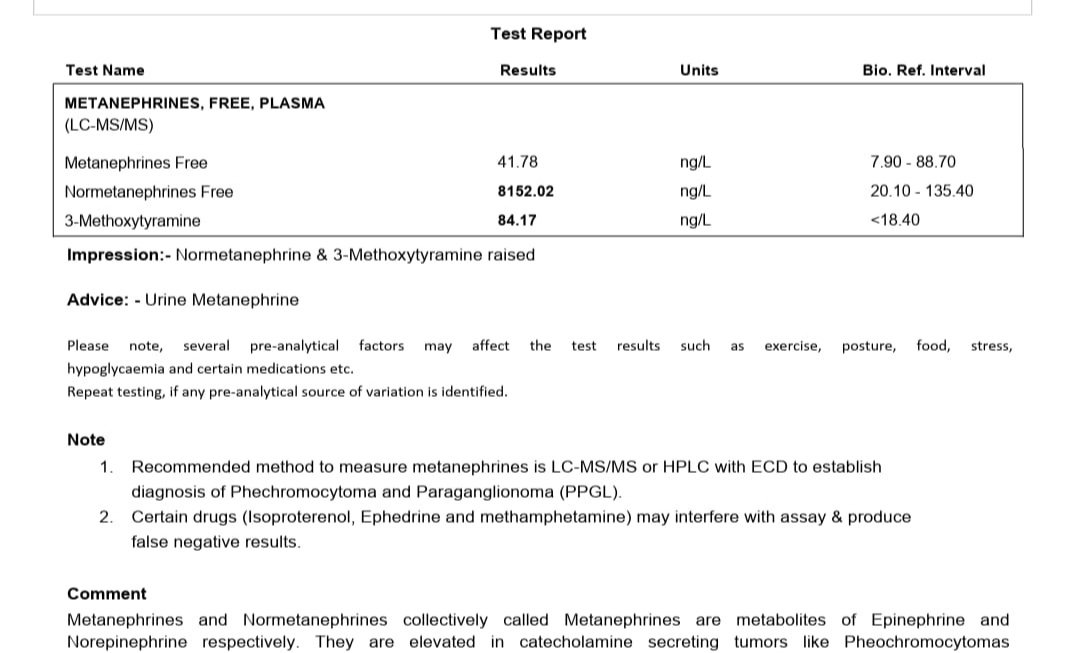
Daraxonrasib- The new weapon in the armamentarium against pancreatic cancer is creating ripples across the med onc community
I would like to take this opportunity to remind you how incredible Oncology residency is:
In the 1 st year ,you hear about the names of all these fascinating drugs
In the 2nd year , you learn how to pronounce the names of all these drugs
In the 3rd year , you understand how to prescribe all these fantastic molecules
And after you pass out, you get to know that all these "fascinating" drugs have become redundant..and you go back to learning how to pronounce these new drugs again
18
1,294
Jun 1
There is no test in the world to differentiate between SIADH and CSW
The only way you can come to a conclusion is by giving a trial of fluids and see the response
If the patient improves its spot on Cerebral Salt Wasting and if the patient deteriorates it is multiple Consumer court visits
2
1
9
932
May 18
In the face of global unrest , India is facing a severe shortage of platinum agents
It is a sad time for most oncology centres EXCEPT for that one institute we all know that will come out with the SUBPLAT trial-" Substitution of platinum drugs with other chemotherapy agents in war affected areas- A real world study of 1000 patients" ☠️
5
278
Naman retweeted

1. High CRP /procalcitonin = infection
2. Low CRP/procalcitonin = no infection
3. ESR is useful
4. Granuloma = TB
5. Flucloxacillin is superior to cefazolin
6. Antibiotics prevent infection (infection prevention prevents infection: mainly hand hygiene)!
7. Perhaps contrast-induced nephropathy (not my area of expertise)
8. You need three drugs to treat HIV (not a major issue, but two will mostly do just fine)
9. Pyuria = UTI
10. Bacteriuria = UTI
11. Positive BAL/sputum/tracheal tube cultures = pneumonia
12. You need cephalexin (use cefadroxil)!
***
And as always
-Longer is better
-IV > oral
2
13
25
2,271
Naman retweeted

May 2
One of the BIGGEST sources of confusion of diuretic therapy with ascites is getting the dosing wrong.
For CHF spironolactone is 25 mg. In Ascites we START at 100 mg and go to maximum of 400 a day.
Furosemide is added with 40 mg and maximum 160 mg
5
56
403
25,238
Apr 28
If you are single you often feel left out ,unhappy , sometimes even miserable
You are unable to thrive, blossom and reach your full potential !
That is why Myeloma decided to not be single . It chose to be multiple- Multiple myeloma, multiple lesions ,multiple tumors
It decided to be savage af and wreak havoc 😈
2
1
9
773
Naman retweeted

Apr 26
You are about to give parenteral B12. Which electrolyte must be checked first and what complication are you trying to prevent?
46
97
1,028
354,726
Naman retweeted

Apr 22
Medical guidelines have destroyed critically thinking in medicine.
139
227
1,709
322,227
Apr 12
Heard many south indian songs but Monica Belluci always hits different!
I think idolizing Western stars in Indian songs is the secret ingredient to a hit song recipe
2
4
532
Naman retweeted

People who diss clinical examination as part of the diagnostic algorithm probably were never taught it properly, consequently are shit at it, and have also probably never diagnosed anything based on clinical exam in their entire lives...
9
11
104
7,230
Apr 7
This is where I write most of my tweets -over a cup of caffeine
The calm ambience and aroma of coffee gives me the motivation to provide insights into medicine residency, write medical humour and trigger uptight medtwitter specialists
2
1
7
384
Apr 6
I would be impressed if you knew how to read an MRI Brain film
But I would be bamboozled if you knew how to read an MRI spine
Try identifying the pathology here
10
9
85
35,306
Apr 5
Diuretics come much much later in the treatment of fluid overload
The first and foremost thing is to correctly estimate the Input- Output balance
The reason why Govt hospitals fail in this in contrast to corporate is because the balance is calculated by Nurses:-
The Nurse to patient ratio in corporate is 1 : 3
In govt it is 1 :20! - This is where mistakes occur
Folks,
We dont need a higher Doctor:Patient ratio
We need a higher Nurse:Patient ratio
4
5
65
9,297
Apr 3
For the Specialist not trained in the Gen Med here is an important but overlooked tip for your patient's Creatinine problems:
If the BUN/Creatinine ratio is >20- Give Fluids. The Creatinine will normalize after 24 hours
If the BUN/Creatinine ratio is <20- Call the nephrologist. This is not your patinet to treat !
10
24
236
22,106

Apr 1
What agent do you use for luminal treatment of an amebic liver abscess ..that is available in India ?
Curious to know
@Gastronaut___
@anujtiwari11
@Gaurz3
1
6
1,134
Mar 28
Knya med is going All out on marketing their new line of stethoscopes- claiming theirs have sharper acoustics,better clarity and more comfort
What they dont realise is that medicos don't buy Littman for its superior acoustics
They buy it for Brand Value and the Glory that comes from having a Littman wrapped around your neck 🌟
13
3
146
15,466
Mar 25
All corporate hospitals, DNB institutes have a Code Blue system-
Wherein an alarm is announced across the hospital whenever a patient collapses,and all available doctors are supposed to rush immediately to the incident site
But no such system exists in government hospitals-
Not because of lack of infrastructure , but because if a Code Blue system was implemented in govt institutes the whole hospital would be ringing with sirens...24/7 !
6
35
419
68,420
Mar 15
Dear Juniors ,
The most common cause of T inversion in leads 2,3,aVF is not Inferior Wall MI ..it is Incorrect Limb Lead placement
Which is why you should know how to do ECG and not leave it to the nursing staff ..😀
6
13
239
18,552