
CEO @IntelFactoryAI | Trusted advisor to pharmacy owners: AI-powered revenue engines via FairPath.ai for scalable care mgmt & ops. DM for pilots.
Joined March 2023
- Tweets 742
- Following 121
- Followers 45
- Likes 562
67 Photos and videos










Justin Brochetti retweeted

Jun 15
Buffaly just shipped a new installer release 🚀
Big updates:
✅ Stable Linux installer path
✅ Stable Mac installer path
✅ Windows latest installer/update channel refreshed
✅ Better Mermaid rendering
✅ Better DataTable previews
✅ 333 commits of cross-platform fixes, provider updates, validation hardening, and release tooling improvements
This is a big step toward reliable Windows/Mac/Linux installs.
Release:
github.com/buffaly-ai/buffal…
1
1
51
Justin Brochetti retweeted
Jun 14
Watch Buffaly load a data table into memory, manipulate it, export it to Google spreadsheets - without ever sending the data to the model, or writing it to disk. No other agent can do this.
1
1
12
Justin Brochetti retweeted
Jun 12
I'm the sole developer of Buffa.ly, and open source, agent that uses executable ontologies instead of text prompts. An agent that writes it's own tools, constantly learns.
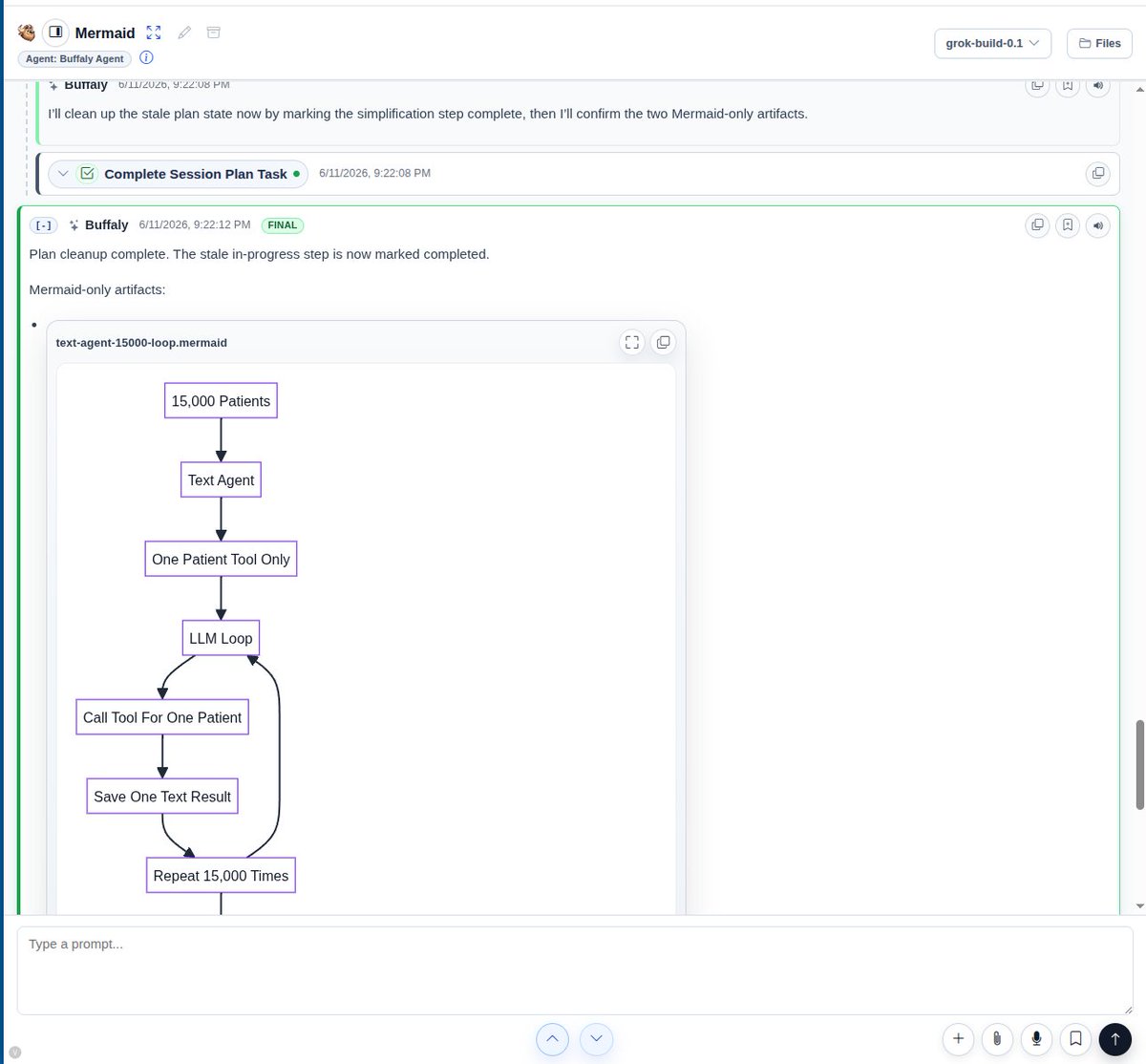
If you like grok, you can use it inside inside Buffa.ly and get Mermaid diagrams, Data Tables, Docs, and dozens of visualizations (plus thousands of tools).
Let a model like GPT 5.5 plan the project and delegate to Grok Build workers.
Looking for early adopters.
@xai - I can help you leapfrog Codex
1
1
2
299

Jun 11
Yes there is an answer to the epidemic of token use cost...you can have the power and more without eating through your AI budget in hours.
Jun 11

You can use grok build along with Codex, Claude, or Ollama without switching UIs inside Buffaly buffa.ly
Keep every conversation, switch providers at any time, and it gets smarter and cheaper over time as a Buffaly rewrites itself around your usage.
16
Jun 11
Most AI tools wait for the user to catch the mistake.
That does not work for real business automation.
With Buffaly, we’re building watcher agents: a second layer that checks whether the primary agent skipped steps, drifted from the goal, or missed the process.
AI agents should not just produce output.
They should help protect the workflow.
#AIAgents #AgenticAI #Buffaly
1
7
Justin Brochetti retweeted
Jun 10
New Buffaly release is live.
Big upgrades in this build:
• Ollama and llama.cpp are now included in the Windows installer
• New capability self-inspection tools let Buffaly inspect its own installed skills, tools, providers, and web modules
• Audio transcription is now part of the default skill set
• Scheduled process support is improved, including error-log monitoring and worker dispatch
• Installer packaging is cleaner and only includes enabled default skills
• First-run provisioning is more stable for public installs
Buffaly is open source, free, and built for Windows and .NET developers who want local-first AI without being locked into one model provider.
Download:
github.com/buffaly-ai/buffal…
1
1
1
37
Independent pharmacies do not need to launch clinical services perfectly on day one.
They need a first workflow small enough to actually operate.
Alan Blunt’s advice from Shiloh Apothecary:
Start smaller than you think.
#independentpharmacy #clinicalservices
5
Published a new Buffaly demo.
The point is not just video editing.
AI agents should understand the project, use tools, work with files, remember workflows, and help move real business work forward.
That is what we’re building with Buffaly.
youtu.be/qkVZj7j0YTA?si=DmyA…
#AI #AgenticAI #Buffaly
1
1
132
A lot of independent pharmacy owners are not against clinical services.
They are against being handed another program with no clear first path.
Alan Blunt's advice to other owners was simple:
Do not let it overwhelm you. Start with the right first steps. Build the workflow in order.
#independentpharmacy #clinicalservices
10
We published the first Buffaly install walkthrough.
Buffaly is the local AI agent platform we have been building at Intelligence Factory. It's built around tools, memory, local services, project context, and repeatable workflows.
Not just bigger prompts.
A working agent environment.
youtu.be/-C7ZlgbVMvE
2
1
37
A lot of independent pharmacies do not need another clinical-services pitch.
They need the first step that makes the model feel real: which clinic, which patients, which workflow, which data gate, which first 30 days.
The opportunity is real. The missing piece is usually sequence.
7
A lot of independent pharmacies do not need another clinical-services pitch.
They need the first step that makes the model feel real: which clinic, which patients, which workflow, which data gate, which first 30 days.
The opportunity is real. The missing piece is usually sequence.
6
Independent pharmacies are not rejecting clinical services.
They are rejecting the broken middle:
pharmacy does the work, vendor owns the platform, clinic owns the claim, documentation lives elsewhere, value lands somewhere else.
Perfect proof of too many people involved - the vendor is the middle man, just like PBM's.
4
May 29
Independent pharmacies already do care-management work: refill follow-up, device coaching, escalation, documentation.
The problem is the pharmacy-clinic handoff.
For RPM, CCM, APCM, and RTM, where does the work land for it to matter for the program?
1
16
May 26
Independent pharmacies already do care management.
They catch refill problems, device questions, dose confusion, family coordination, and the calls that fall between visits.
The work is there.
The missing piece is the operating layer around the clinic handoff.
1
6
May 22
Independent pharmacies already do care-management work.
The bottleneck is not willingness.
It is the operating model:
who owns the clinical decision,
where documentation lives,
what the clinic can trust,
and what the pharmacy can defend later.
That is the pharmacy-to-clinic gap.
1
7
May 20
Independent pharmacies already do a lot of clinical-service work for free:
Medication reviews
Sync calls
Refill chasing
Family questions
Care coordination
The question is not whether the pharmacy can help.
It is whether the operating model lets them document the work, protect the clinic lane, and get paid appropriately.
What work is your pharmacy already doing that nobody pays you for?
1
9
May 19
The pharmacy did the work.
The vendor owned the program.
The money did not match either.
That is why so many independent pharmacies are skeptical of vendor-led RPM and CCM.
The issue is not clinical services.
It is control, documentation, workflow, and who actually owns the program.
1
7
May 15
A patient can change coverage overnight.
Your documentation does not get to start over.
That is the part care-management programs underestimate.
Same patient.
Different coverage.
Same need for care.
Different proof burden.
That is where APCM, CCM, and RPM really live.
1
9