
Clinical Scientist 🧑🏻🔬. Also bit of a space nerd 🌌 Like/repost/follow ≠ always agree.
Joined November 2018
- Tweets 1,378
- Following 298
- Followers 426
- Likes 2,878
27 Photos and videos





Pinned Tweet

13 Feb 2023
261
2,475
8,580
1,381,996
Apr 1
I cannot eay this enough. A 'negative' tumour marker result NEVER excludes malignancy and a 'positive' never diagnoses malignancy in its self. And yes, this includes CA 125 and PSA. Tumour marker fishing is also a bad idea. Pre-test probability is extremely important.
56
Kade 🧑🏻🔬🌌 retweeted

For doctors, most diagnoses come from the history and examination. In many non-medical pathways, it can feel like the reverse: very little diagnosis from history/exam, and a heavy reliance on tests or onward referral, sometimes with no working diagnosis at all. If someone doesn’t understand what history and examination are for, it’s easy to skip them and default to “do tests” or “admit/refer so a specialist can diagnose”.
The problem is that tests are then interpreted without a Bayesian “a priori” anchor. Without a pre-test probability built from a good story, a focused exam, and an understanding of how common conditions are so you’re left with results that can mislead, over-diagnose, or generate incidental findings. And if you don’t have a detailed grasp of disease patterns, you don’t know which questions to ask or what to look for to diagnose dementia or depression or diabetes or diphtheria. You can’t form a meaningful differential if you don’t know what’s common, what’s dangerous, and what’s discriminating.
So the whole process drifts into secondary referrals and scanning as the default route to certainty. In parallel, some non-medical exams don’t require a deep knowledge base, so people are expected to “look it up” in real time under pressure. That isn’t the same as understanding, and it’s hard to expect consistently good outcomes from it.
The final issue is that often one doesn't know what one doesn't know. This can lead to overconfidence or a very defensive position.
Finally if you want to be seeing patients and making good diagnoses there is course for this called Medicine. Exams do expect knowledge.
26
139
506
39,547
14 Oct 2025
Wait... this is controversial?? 🤦♂️
14 Oct 2025

The opinion of people who received a medical degree is vastly superior to the opinion of those who did not, when it comes to medically related topics.
223
Kade 🧑🏻🔬🌌 retweeted

14 Sep 2025
If you think extremism only comes from one side, you are part of the problem
151
92
1,022
22,612
Kade 🧑🏻🔬🌌 retweeted

26 Aug 2025
This dog already saw this week's news and decided her dad didn't need to know all that. 14/10 (Sasha via ViralHog)
86
1,084
19,235
337,823
Kade 🧑🏻🔬🌌 retweeted
28 Aug 2025
This is Parker. He will not eat until he receives a forehead kiss. 13/10 would give him so many smooches
146
1,939
39,080
1,252,209
28 Aug 2025
SPACE FACT #6: Magnetars - a type of neutron star - have a magnetic field a TRILLION times stronger than the field surrounding Earth. This is so powerful that if you found yourself 1,000 km away from one, you would die as the electrons in your body's atoms would be distorted 🤯.
1
100
Kade 🧑🏻🔬🌌 retweeted

27 Aug 2025
By far the most beautiful launch I’ve seen to date.
This is one of thousands of photos I captured across 7 cameras. I can’t wait to share more with you!

1,017
1,929
21,545
1,406,721
27 Jul 2025
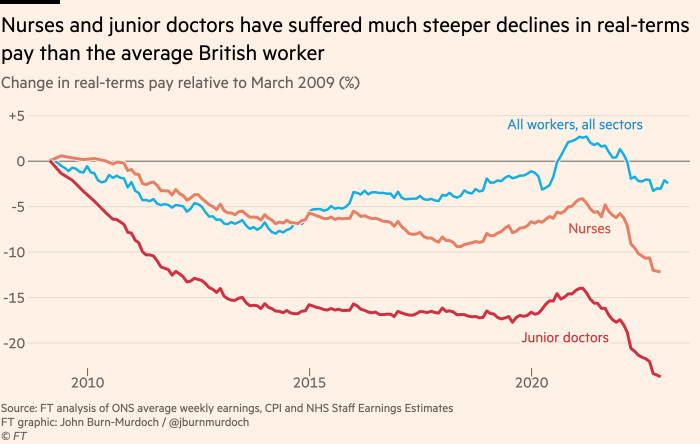
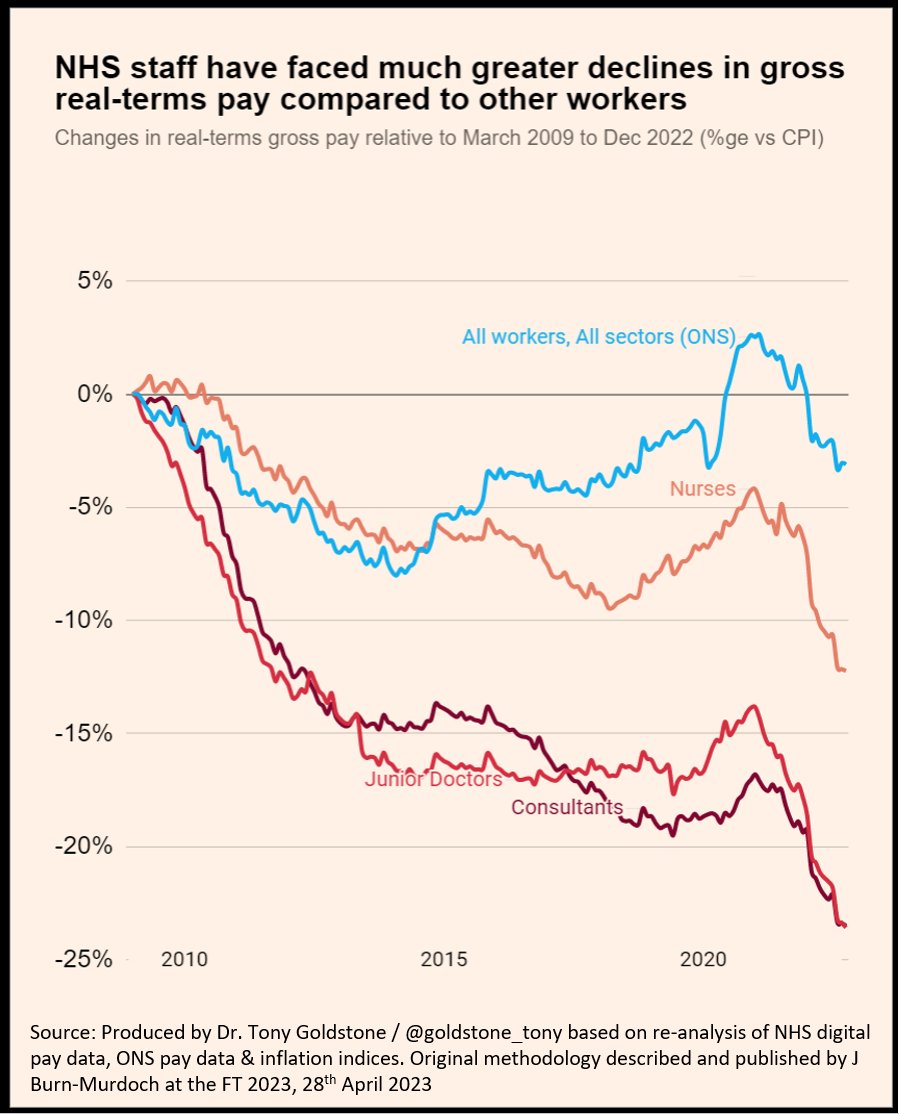
If we can't afford to pay good doctors and all other NHS staff the global market rate to keep them here to maintain a world class health service, then we cannot afford the NHS. It's as simple as that.
99
Kade 🧑🏻🔬🌌 retweeted

18 Jul 2025
My wife cheated on me at a Linkin Park concert but in the end, it doesn’t even matter.
230
1,041
48,780
2,268,377
Kade 🧑🏻🔬🌌 retweeted

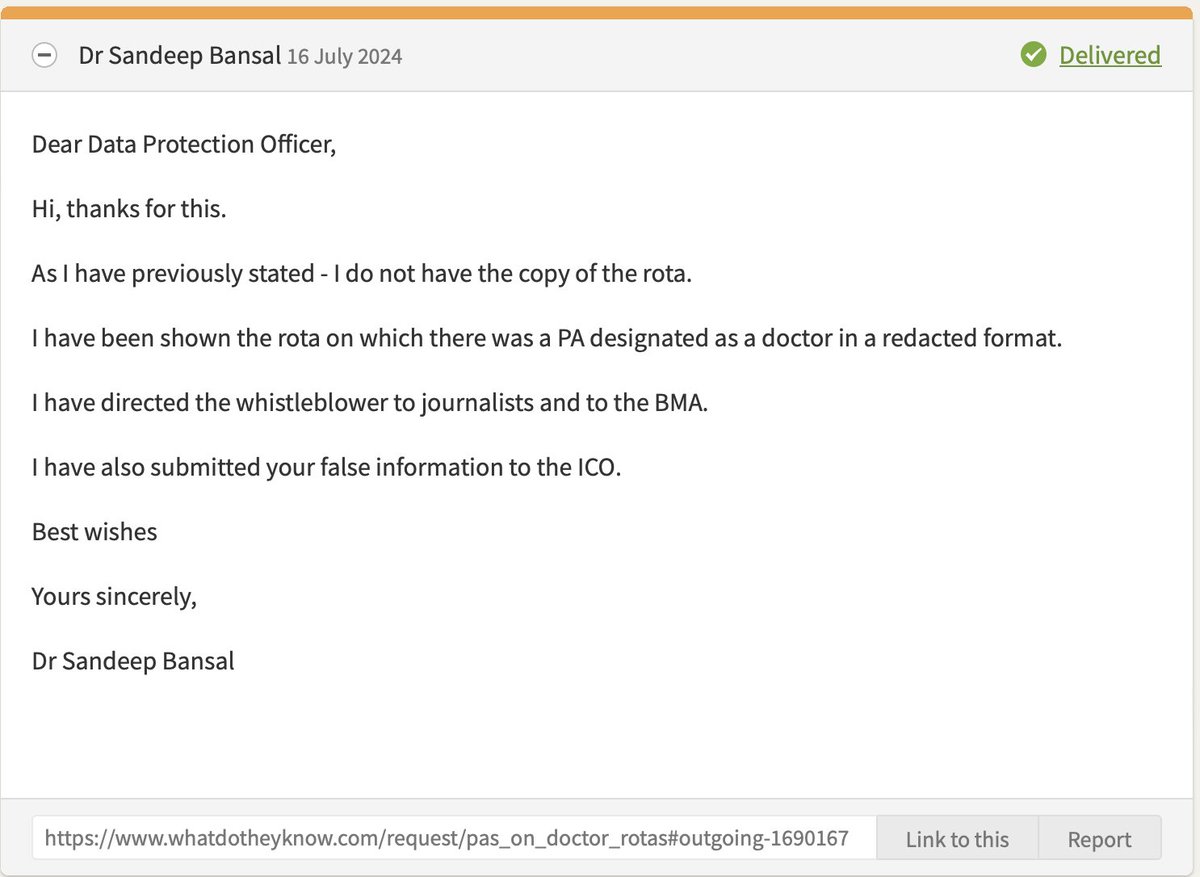
16 Jul 2025
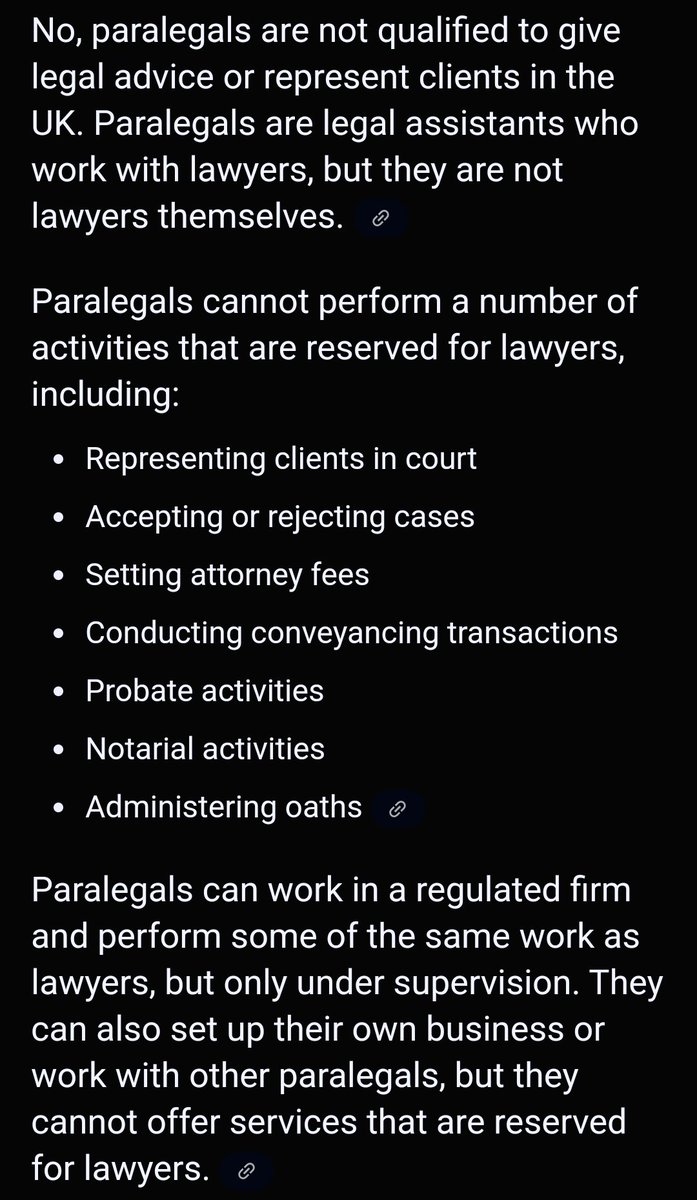
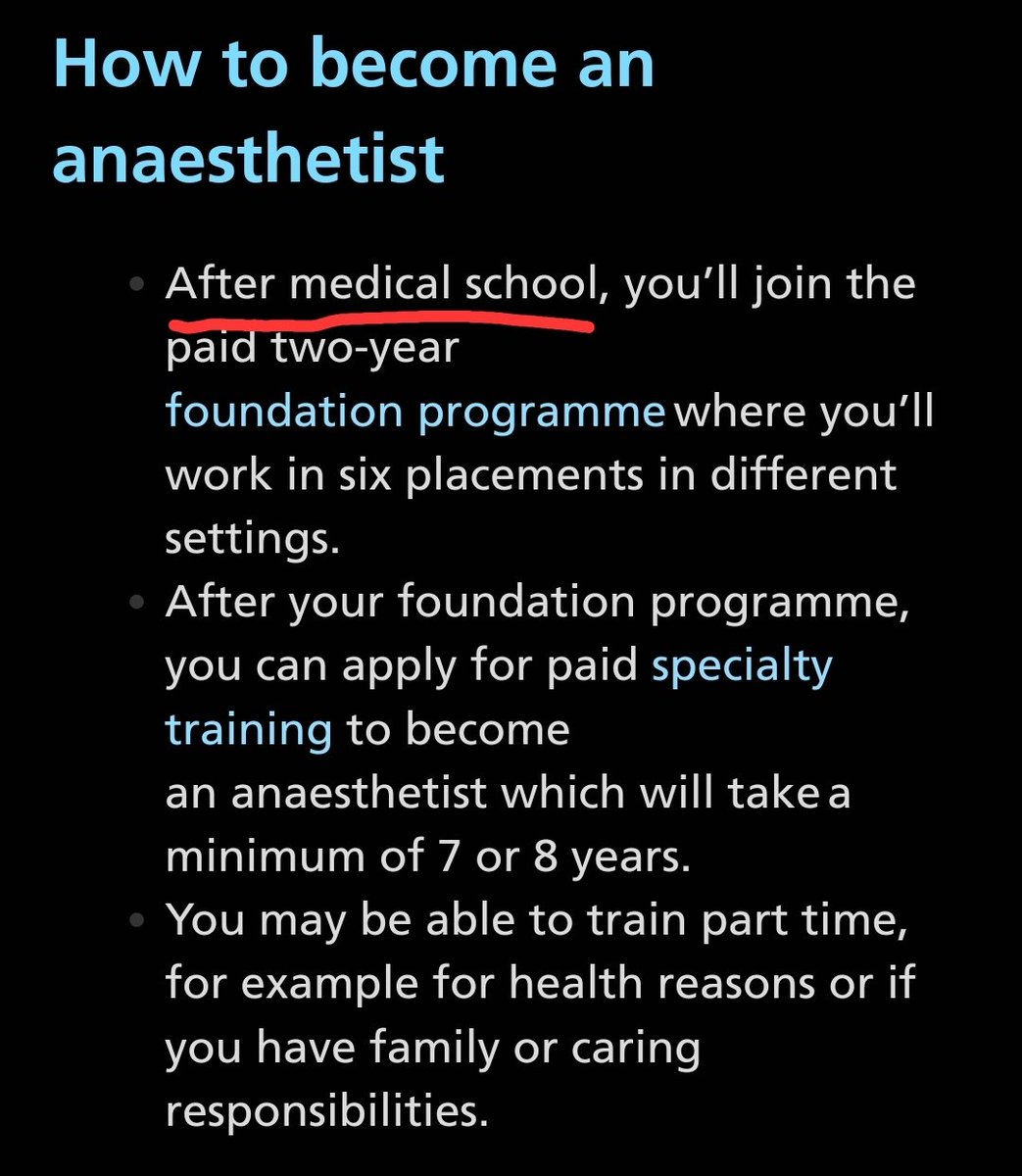
From a patient point of view PAs AAs should be none existent, leave it to Drs and Nurses not forgetting the hard working healthcare support workers.
Do the training necessary to become a qualified Doctor or Nurse.
21
138
2,713
24 May 2025
Absolutely delighted to have passed the module 1 and module 2 exams for part 2 of the Royal College of Pathologists. I never have to sit another exam again! Now to becoming a fellow and paying the RCPath £600 a year 😂
2
196
11 Apr 2025
USS Callister: Into Infinity was an absolute masterpiece! I loved it even more than the first one! As sequels go, that was pretty amazing. #BlackMirror #USSCallister
261
7 Apr 2025
This is very concerning. X isn't perfect, but one thing it is good for is allowing everybody to speak their mind and critique, which is essential for organisations as important as this. You can't just run away from criticism - listen and do better (your job) instead.

We will no longer be posting on Twitter/X as we’re focusing on platforms where we can engage more effectively with our audiences and provide information to support our registrants, patients, and the public.
We’ll keep our account to stay up to date on key issues and to help inform our communications on other channels. For more information on how we’ll use X, please read our social media policy: gmc-uk.org/disclaimer#social…
To stay updated with our latest news and information, we encourage you to follow us on our other channels - Instagram, LinkedIn, and Facebook - or visit our website.
If you have a question, visit our contact page via the link in our bio, and we’ll make sure you’re directed to the right team.
1
5
37
1,844
Kade 🧑🏻🔬🌌 retweeted

30 Mar 2025
I think my weather app is broke.

98
210
6,725
454,702
Kade 🧑🏻🔬🌌 retweeted

28 Mar 2025
A positive troponin is not an MI. A positive BNP is not heart failure. A positive lactate is not sepsis. Please for the good of society can this be properly taught in all medical training programs?
27 Mar 2025

A positive urinalysis is not a UTI. Please for the good of society can this be properly taught in all medical training programs?
61
201
1,592
224,834
3 Jan 2025
The fact that this is even being discussed is beyond belief 🤦🏻♂️
3 Jan 2025

Doctors SHOULD have a monopoly over medicine
Just as dentists have a monopoly over dentistry
Just as pilots have a monopoly over aviation
Just as teachers have a monopoly over teaching
It is simply undergoing the correct training for the job.
1
2
275
11 Dec 2024
#SPACE #FACT #5: Neptune has the fastest wind speeds in the solar system of up to 1,200 mph! For comparison, the fastest non-tornado windspeed ever recorded on earth was 253 mph, recorded in 1996 during cyclone Olivia on Barrow Island, Australia.
science.nasa.gov/neptune/nep…
106
8 Dec 2024
#SPACE FACT! Neutron stars are so incredibly dense that a sugar-cube sized amount of it's material would weigh a BILLION tonnes on earth. Not a million... a BILLION TONNES. That is 1,000,000,000,000 kg. This fact weighs me down.
1
1
231