
Dietitian | @SCCMSE & @GASPENGa & @ASPEN_nutrition | #WhatRDsDo #ICUNutrition | She/Her | Views my own. open.substack.com/pub/adepri…
Joined March 2009
- Tweets 8,989
- Following 1,750
- Followers 2,343
- Likes 30,568
674 Photos and videos








Pinned Tweet

24 Mar 2025
You can also find me where the ☁️ is 🔵! #ICUNutrition #WhatRDsDo
👉ashleydepriestrd
2
680
As dietitians we are often trained to make our recommendations as a to do list:
▪️start tube feeds
▪️add MVI
▪️start EN
But that often brings up more questions about implementation.
Framing your recommendations as solving a problem vs a task is more clear & effective.
48
A good reminder that antioxidants become oxidants when they run out of things to anti-oxidize, even if you do “just pee it out”
Individualized approaches are best!
Jun 10

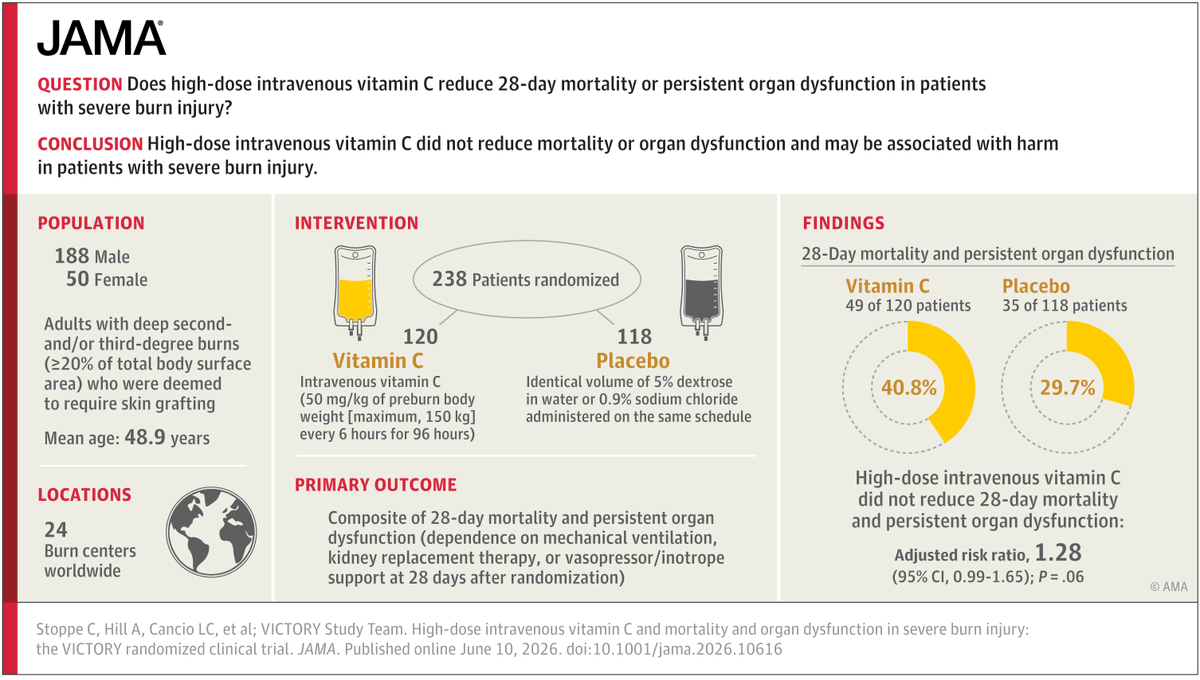
🧵 Among adults with severe burns enrolled in an international double-blind, placebo-controlled trial, high-dose intravenous #VitaminC did not improve survival, reduce hospital length of stay, or prevent organ dysfunction.
#CCR26 @CritCareReviews
ja.ma/49RpUzX
6
1,102
Dietitians add value to patient care. Full stop.
If we learn how to communicate that value with the right language then influence, credibility and, yes, pay, will follow.
#WhatRDsDo
1
2
397
Many RDs spend years mastering nutrition science but very little time learning how hospitals actually work.
The more you understand the workflows, pressures, and decision making processes of other disciplines, the more effective your recommendations become.
1
3
134
Patient care doesn't happen in the EMR. It happens through people, processes, and competing priorities.
Understanding implementation may do more for your credibility and influence than another certification ever will! (But I still endorse those certifications 😉)
105
There are subtle ways we as dietitians can undermine our own clinical authority.
I wrote about my experiences here:
open.substack.com/pub/adepri…
1
3
81
I’ve loved teaching the enteral nutrition tolerance portion of this series over the last two years. We have such great discussions and I always coming away having learned something as well!

📣 REGISTER Now for 2027 Duke Online Clinical Nutrition Fellowship to learn & interact with international nutrition experts!
📝 Apply by E-mail by sending your CV & letter of interest before 2027 class is full!
📧 APPLICATION EMAIL:
online.clinicalnutrition@dm.duke.edu
🔗Info: anesthesiology.duke.edu/clin…
#dukenutritioncourse #clinicalnutrition #meded #dietitian #icunutrition
@Duke_Anesthesia
@ICUnutrition @CriticalCareNu1 @ElisabethWaele @drshahrul80 @BrunoDietitian

1
4
1,049
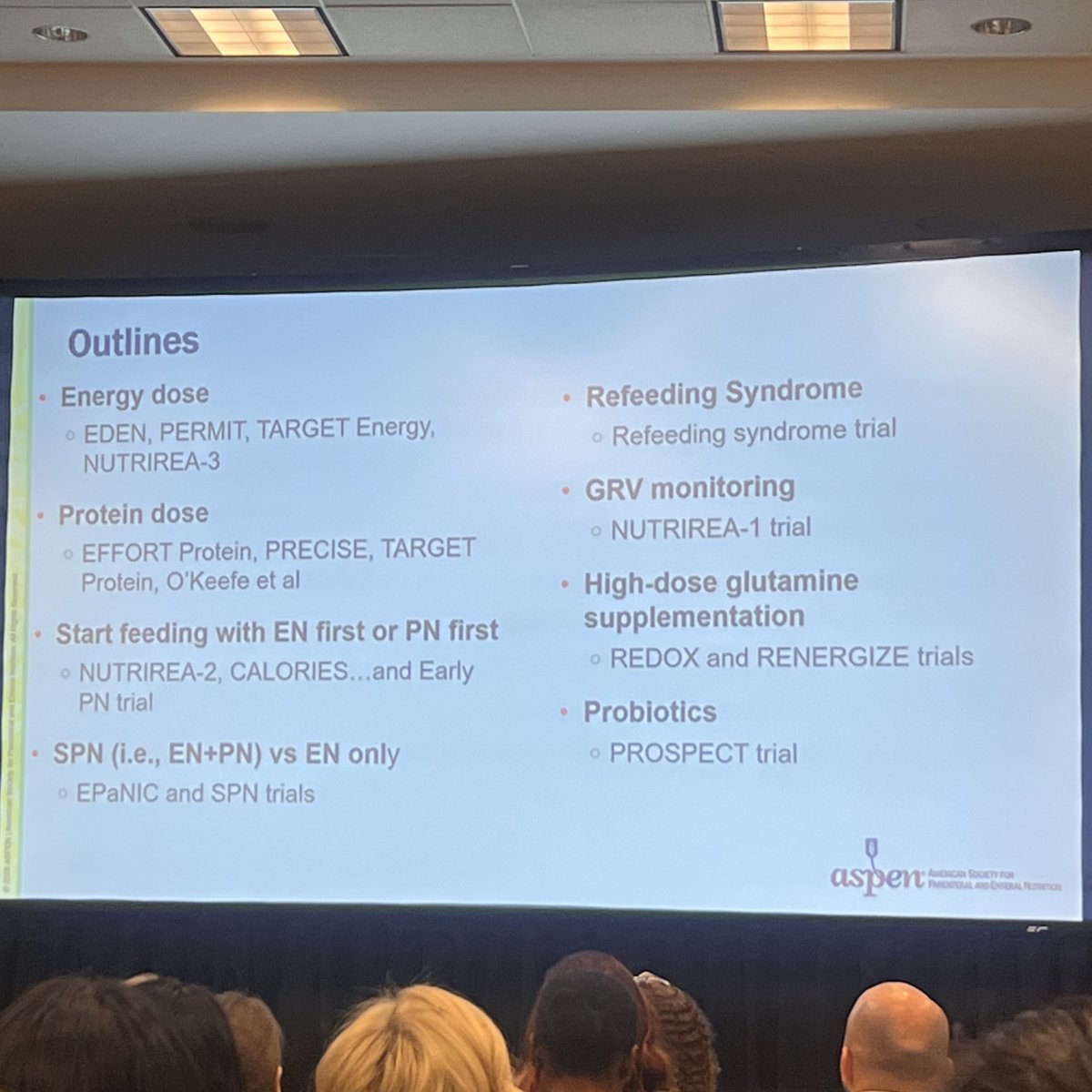
ICU patients typically receive only 50–60% of recommended energy and protein in the first week. The EuroPN cohort found patients hit just 65% of protein targets across European ICUs.
Why?
1
2
609
The field is shifting toward restrictive dose nutrition early, with escalation after the acute phase. The question is no longer "are we feeding enough?" it's "are we feeding right?"
And the best person to navigate these nuances?
💪🏼Registered Dietitian!
#WhatRDsDo
1
1
67
If you want to learn how to build and strengthen your nutrition credibility and influence to help close this gap check out my Substack!
substack.com/@adepriest?r=ch…
1
56
Are you a dietitian looking to build influence and credibility on your hospital unit?
Start with these 3 actions:
#WhatRDsDo
1
142
Track and report metrics. You can’t improve what you can’t measure!
1
35
What are you already doing? What challenges do you face?
If you’re interested in strengthening your credibility and influence with your hospital teams, take a look at my Substack for more!
open.substack.com/pub/adepri…
33
We write:
“Start EN when the patient is HD stable”
“Monitor tolerance closely”
“Consider PN if needed”
Then wonder why it isn’t followed.
Specificity builds trust AND credibility.
How would you adjust these phrases for better credibility?
1
71
I’ve started a Substack! Sure I’ll talk about data & trials (you know I love to!) But I’ll also be sharing about things we aren’t formally taught, like how to build influence with your clinical teams.
Check out my first post, I hope you’ll subscribe!
open.substack.com/pub/adepri…
1
78
When sending patients home on EN it’s so easy to continue what they are receiving inpatient. Consideration for usual long term nutrition, such as fiber intake, needs to be considered. Unless contraindicated, no patient should go home w/ fiber-free formulas long term. #WhatRDsDo
77