
Short skirt and a long jacket. Galatians 5:23 and the 1951 Refugee Convention.
Joined April 2026
- Tweets 635
- Following 258
- Followers 45
- Likes 1,969
2 Photos and videos
At least you blew up USAID and taxpayers gave billions to GEO Group.
Jun 13

Republicans are in charge because we promised:
to Make America Healthy Again.
to start No New Wars,
to put people above corporations,
to put America above foreign countries,
to release the Epstein files,
to not spy on citizens,
to eliminate fraud,
what the hell happened?!
6
Lysa Strata retweeted

Jun 12
The world’s first trillionaire made a pedophile rapist the president of the United States and then personally made sure starving children couldn’t get food and medicine, with 14 million deaths projected from his actions alone. He’s possibly the most evil person in history.
653
8,123
39,711
409,159
Lysa Strata retweeted

Jun 12
The Billionaires don’t wake up at 5am. Teachers, nurses, bus drivers, etc., wake up at 5am. Billionaires wake up whenever they want because their wealth doesn’t come from their own labor.
It comes from the labor of people who will never be billionaires.
331
702
3,145
44,729

Jun 11
Horrific.

🚨Trump is going to deport Iranian women who PROVED to an immigration court that they would be persecuted in Iran to the Central African Republic, a country so dangerous to others the U.S. recommends no American travel there.
Trump is destroying this country's legacy of freedom!

13

Lysa Strata retweeted

Jun 9
Things the recovery industry will not tell you:
1. The drug worked. That is why people use it. Not weakness. Not moral failure.
A neurological event so complete and persuasive that any honest account of addiction has to start there.
The problem is not that the drug fails. The problem is that what it does is unrepeatable, and you will burn your entire life to the ground trying to get back to a place that no longer exists.
2. Shame is not guilt. Guilt says I did something bad. Shame says I am something bad. Guilt is appropriate. Shame is a cell with no windows. Most people use the words interchangeably. That mistake is lethal.
3. You cannot shame someone who has already named the thing you are holding over them. Say it first. Say it in plain light. The weapon drops.
4. Guilt can coexist with self-respect. Shame cannot. You can hold the damage and the dignity at the same time. I know because I live there.
5. Radical honesty does not give you back who you were. It hands you the clean slate of who you always wanted to be. The mask comes off. The cartoon other people drew of you stays on the page.
6. Nobody gets clean on a winning streak.
7. You have to be almost self-delusional in your forgiveness of yourself. (Go watch Chase Hughes)
8. The greatest sin was not the chaos. It was the absence. Being unavailable to the people who needed you.
9. Sustainable recovery starts with one thing: honesty with yourself. If you love an addict and want to help, that is the only door in.
10. I am only an expert on my recovery. Nobody is an expert on anyone else’s.
1,396
4,592
37,019
2,387,389
Lysa Strata retweeted

Democrats are so diabolical and ingenious at rigging elections that Republicans control the presidency, house and senate.
268
4,680
24,922
250,177
I’m reposting this so more people can read Hunter Biden’s reply. He’s hauling the whole Twitterverse into a 12 step meeting where we listen kindly and carefully as we stumble toward wholeness.

I have a young adult child in addiction. It isn’t just your recovery that gives me hope; it’s that you are now strong enough and honest enough to transform the endless vitriol and judgment into kindness and encouragement. Extraordinary.
3
28
Lysa Strata retweeted

Jun 7
So let me get this straight:
When immigrants take jobs, it’s a national crisis.
When AI takes jobs, it’s innovation.
Can someone explain why we’re supposed to fear people willing to work, but celebrate technology designed to replace workers?
945
7,671
26,743
308,529
Lysa Strata retweeted

Jun 8
I'm finally reading Dune. This quote, which is in the first few pages, hits hard:
"Once men turned their thinking over to machines in the hope that this would set them free. But that only permitted other men with machines to enslave them."
722
21,528
121,538
2,114,214
I hate to keep driving engagement to that article, but this thread adds specificity to the general and justified outrage.
Jun 6

This @WIRED piece is a clear illustration of the drawbacks of journalism as a method of investigation. It seems the general procedure for media coverage of contentious issues is to call up a few carefully preselected people, listen to their anecdotes…
🧵1/
1
108
Lysa Strata retweeted

What I’m excited about is that @HunterBiden is going to make sobriety great again. Actually it’s always been great but looking forward to him talking more about it.
149
651
7,113
110,632
Lysa Strata retweeted

From status conference this morning:
AUSA: The Court may take judicial notice of information posted on official public websites of government agencies.
Me: Your honor, there's currently a public website by a government agency suggesting noncitizens are not from planet Earth...
3
9
144
22,086

I love how it is impossible to gotcha @HunterBiden because he is the master of his own lore.
2
6
101
Lysa Strata retweeted

.@AlanLevinovitz Six years into #LongCOVID, with growing evidence of immune dysfunction, viral persistence, autonomic dysfunction, and neuroinflammation, a professor of religion writes a 10,000-word article on the disease and concludes that the real mystery is patient belief systems and that brain retraining deserves more attention.
The conclusions are remarkably consistent with the author’s questionable academic interests.
The ending was spoiled in the author bio.
To @WIRED: As a publication that covers science, medicine, and technology, perhaps your next Long COVID feature should be one that is actually grounded in science, medicine, and technology.
And perhaps written by a virologist, an immunologist, a neurologist, in the very least someone who is actually engaged in clinical research? What next? A full length feature from a physiotherapist who argues PEM is definitive evidence that LC = MECFS?
A disease affecting millions upon millions worldwide deserves reporting grounded in biomedical science, not a 10,000-word meditation on patient maladaptive belief systems and brain retraining.
My suggestion is you may wish to retract this article - or in the least run an opposing editorial in your next edition unless your ultimate plan was to not only lose millions of readers but also recklessly spread harmful misinformation that further amplifies narratives that downplay the biological reality of Long COVID, continues to put patients at risk of being dismissed by clinicians, denied appropriate care and support, and pushed toward ineffective interventions instead of evidence-based research and treatment.
All of this has lasting and very serious consequences for patients and in the most severe cases, without hyperbole, is a matter of life and death.
8
28
131
3,496
Lysa Strata retweeted

They say anything, & it's true & unimpeachable. We say anything, & it's "false illness narrative" & "negative identity formation." This is epistemic violence & iatrogenic violence. We're fighting for our gotdamn *lives*. They fight for their pet theories, status & clicks.
6
16
262
Lysa Strata retweeted

Jun 3
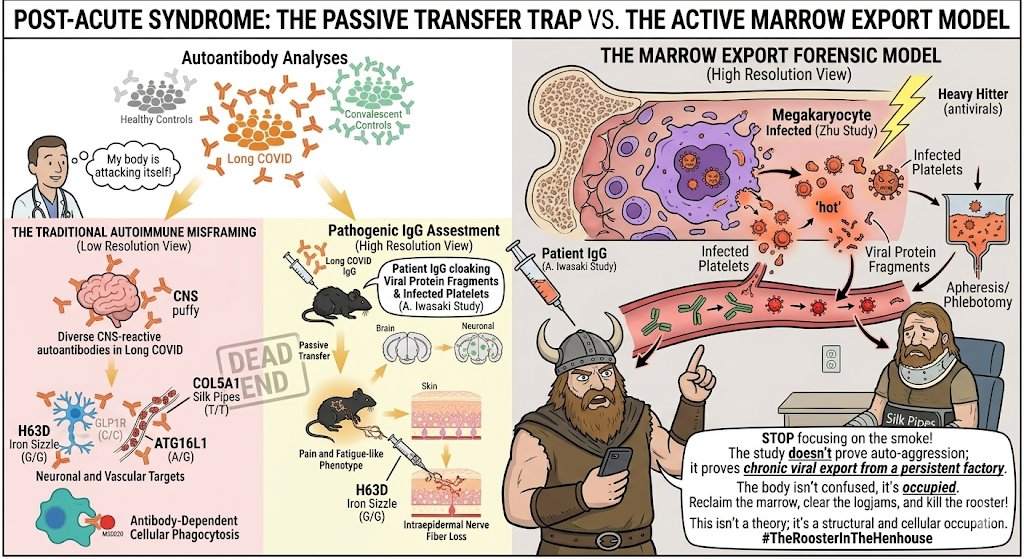
Five Years of Biological Receipts: How Chronic SC2 Destroys the Vascular System and Brain
For over 5 years, corners of the medical establishment have attempted to reduce a catastrophic, viral physical crisis down to anxiety, somatic symptom disorder, or an emotional attachment to labels. Meanwhile, the international scientific community has spent those same five years compiling an undeniable, structural ledger of organic damage.
PolyBio Research Foundation and the Long COVID Research Consortium (LCRC) have made one thing perfectly clear. This is a structural, endovascular, and neuroimmune war. It is not a psychological crisis.
How Chronic SC2 dismantles the vascular system and the brain over a multi-year horizon:
Tissue Persistence & Hidden Viral Factories
The virus doesn't clear after the acute phase. Digital transcriptomics and deep tissue biopsies show that SC2 viral RNA (antisense ORF1ab RNA, which indicates active replication) and Spike protein persist in deep tissue reservoirs including the gut wall, bone marrow, and lymph nodes years after initial infection. This ongoing cellular presence acts like an active factory, keeping the immune system locked in an inflammatory loop that drops virons directly onto vascular tissue.
The Vascular Toll
Continuous immune activation hits the cardiovascular infrastructure.
Endothelial Injury:
Current clinical data demonstrates a profound microvascular endotheliopathy, where the delicate endothelial cells lining the body’s smallest blood vessels are systematically injured, inflamed, and degraded.
Fibrin-Amyloid Microclots:
PolyBio's work with scientists like Dr. Resia Pretorius has mapped the widespread presence of anomalous fibrin-amyloid microclots and infected activated platelets. These dense, breakdown-resistant clots physically choke the microcapillaries, cutting off oxygen delivery to deep tissues and causing widespread cellular hypoxia.
NETs:
Innate immune cells (neutrophils) are hyper-activated, spitting out webs of DNA (NETs) that further clog the vascular highway and drive tissue degradation.
The Brain Attack: Perfusion & Leaky Barriers
When the microvascular highway is choked, the brain pays the price.
Hypoxia & Reduced Flow:
Studies confirm significantly reduced cerebral and microvascular blood flow. The brain is quite literally gasping for oxygen because clogged, narrowed capillaries cannot deliver adequate perfusion.
Blood-Brain Barrier Collapse:
Endovascular inflammation breaks down the tight junctions of the BBB. When the protective wall leaks, peripheral cytokines and inflammatory debris bleed directly into the central nervous system.
Neuroinflammatory Steady State:
Advanced neuroimaging (such as dual PET-MRI imaging by PolyBio-supported researchers like Dr. Michael VanElzakker) reveals active, neuroinflammation. Neural-derived exosomes show markers of severe astrocyte turnover. The brain is forced into a hyper-reactive inflammatory steady state, triggering profound cognitive deficits, verbal fluency drops, and severe dysautonomia.
🛑 Psychology Full Stop
When a patient has a leaky blood-brain barrier, amyloid microclots choking their capillaries, vascular compressions, and active virus in tissues, psychiatry and psychology are the wrong medical disciplines.
A psychologist cannot talk a fibrin-amyloid microclot out of a capillary.
Cognitive behavioral therapy cannot repair an injured endothelial lining or stop a viral reservoir in the bone marrow from churning out toxic proteins. Mindset tools for patients suffering from cerebral hypoperfusion and tissue hypoxia is a severe failure of basic clinical logic.
Reframing a measurable, multi-systemic vascular firestorm as an issue of identity is an act of clinical avoidance. Patients do not need coping to accept their own cellular disintegration. They need hematologists, vascular surgeons, immunologists, and targeted meds. The debate over semantics is over, the era of hard vascular mapping is here.
6
39
95
1,977
Mind body interventions are widely available without a prescription, copay, fee, or subscription. Few side effects. Research should be focused on rigorous investigation of medicines, not marketing for health coaches.

There might finally be a way forward for long Covid treatment—if only you were allowed to talk about it. wired.com/story/the-painful-…
1
47
A wonderful analysis of the “have you heard about exercise?” article.
Jun 3

Ok.
I've read "The Painful Truth About Long Covid" six times through, and I'm ready.
Here are ten clues in the article that point to the writer's bad faith.
2
8
942