
101 Photos and videos




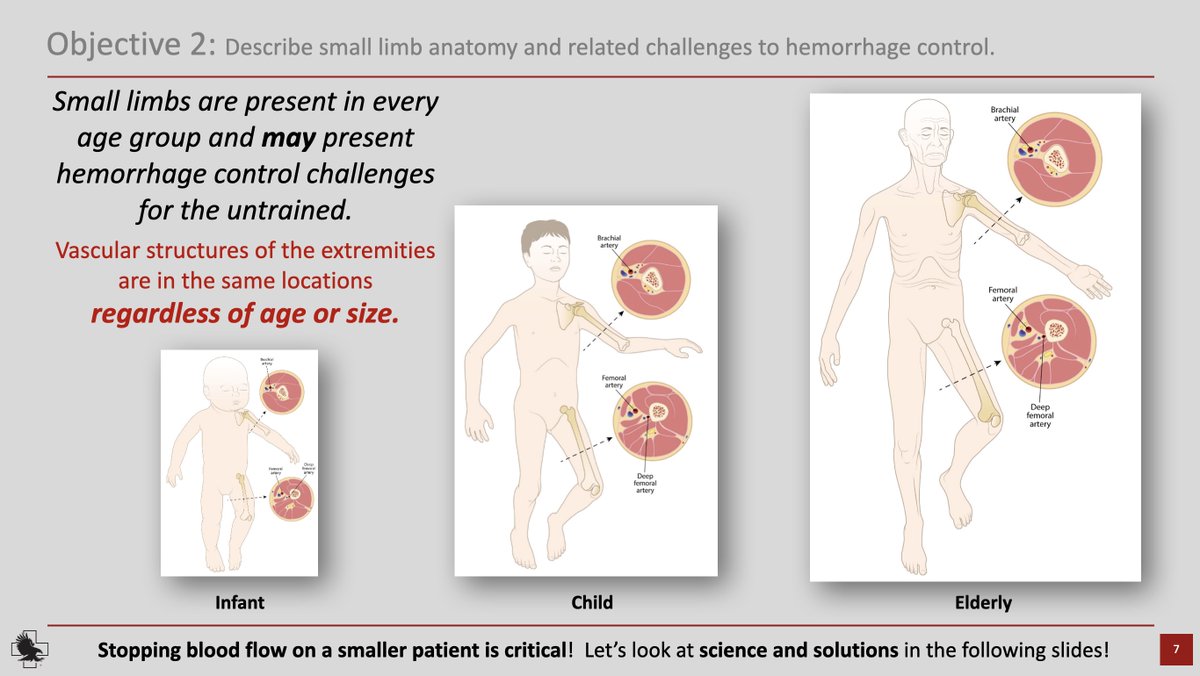
This is a very important point. @JHE360. With a US CCTA, we will be responding to various populations. This will, unfortunately, include the elderly, infants, children and K9s. This may mean that we need to look outside of TCCC approved equipment (for military-aged) to civilian medical equipment to be able to stop the bleed. Neither are inferior, just have different intended purposes.
1
4
59
M*A*S*H Recommended
CCTA Skills: Small Limb Bleeding Control
#CCTASkills #SaveALife #ComplexCoordinatedTerrorAttack
#StopTheBleed #SmallLimbBleedControl
This is an exceptional resource provided by @NARescue for stopping the bleed for infants, children and the elderly.
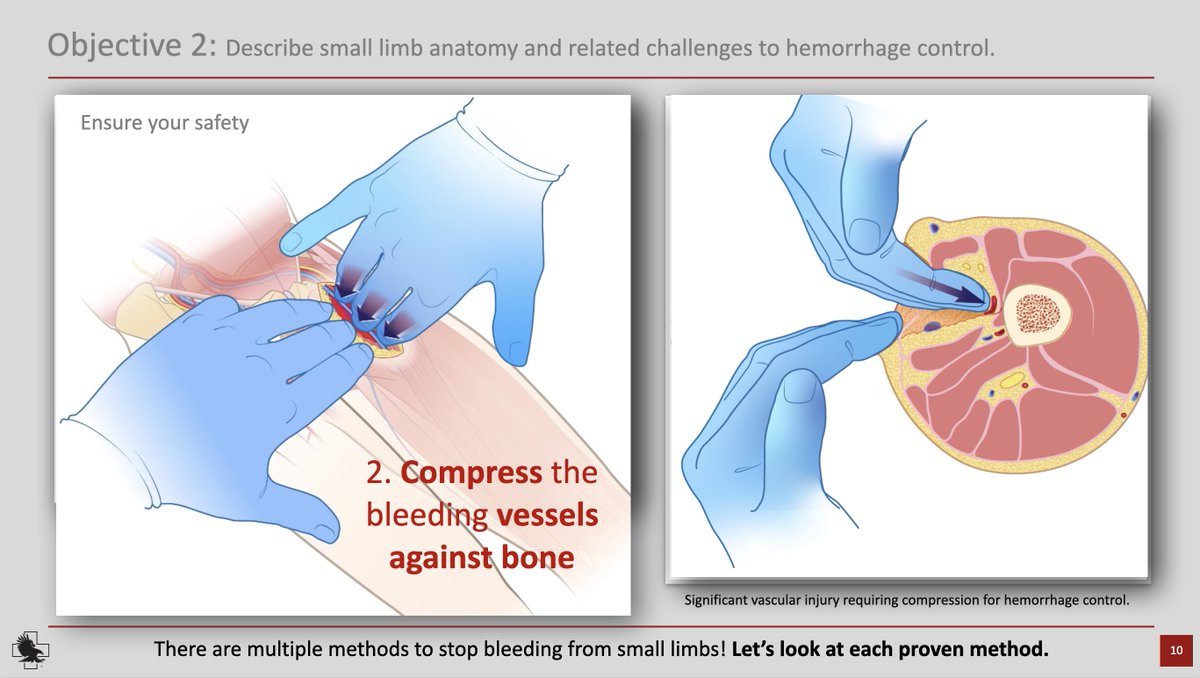
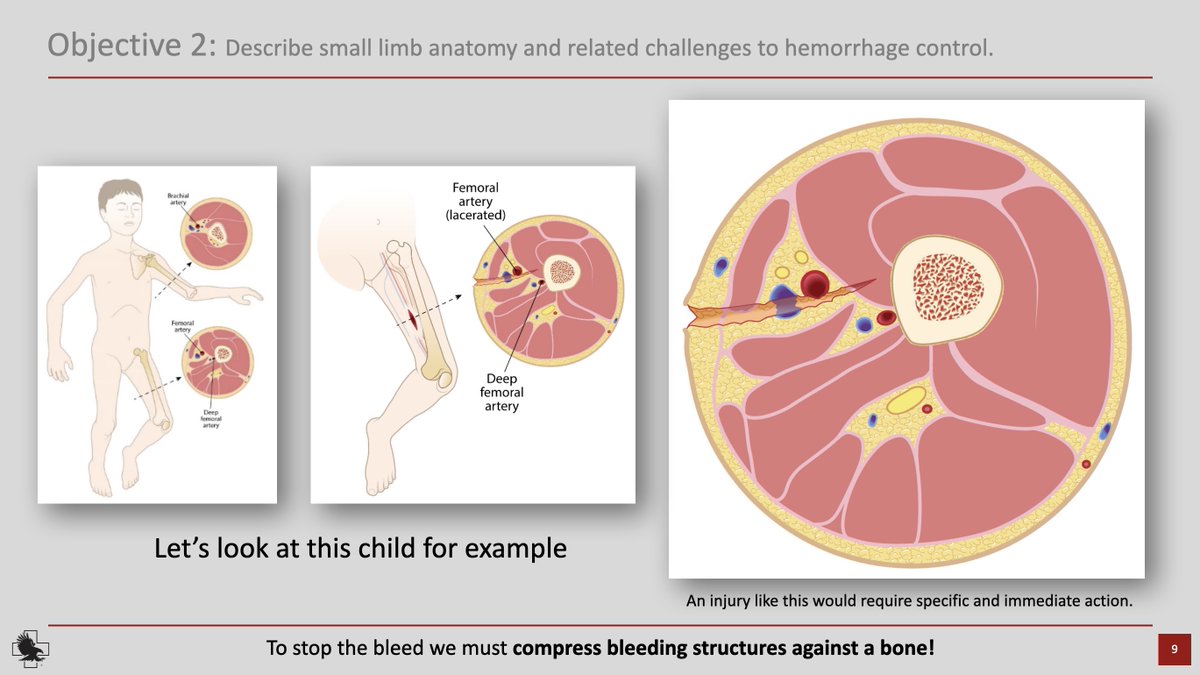
Controlling bleeds in infants, children and the elderly pose particular challenges for the lay-person as tourniquets (C.A.T.) may be too big for these smaller limbs. Additional training is necessary for an adequate response to a CCTA with these populations.
Please utilize this training resource from North American Rescue. Consider North American Rescue for your high-quality medical response supplies.
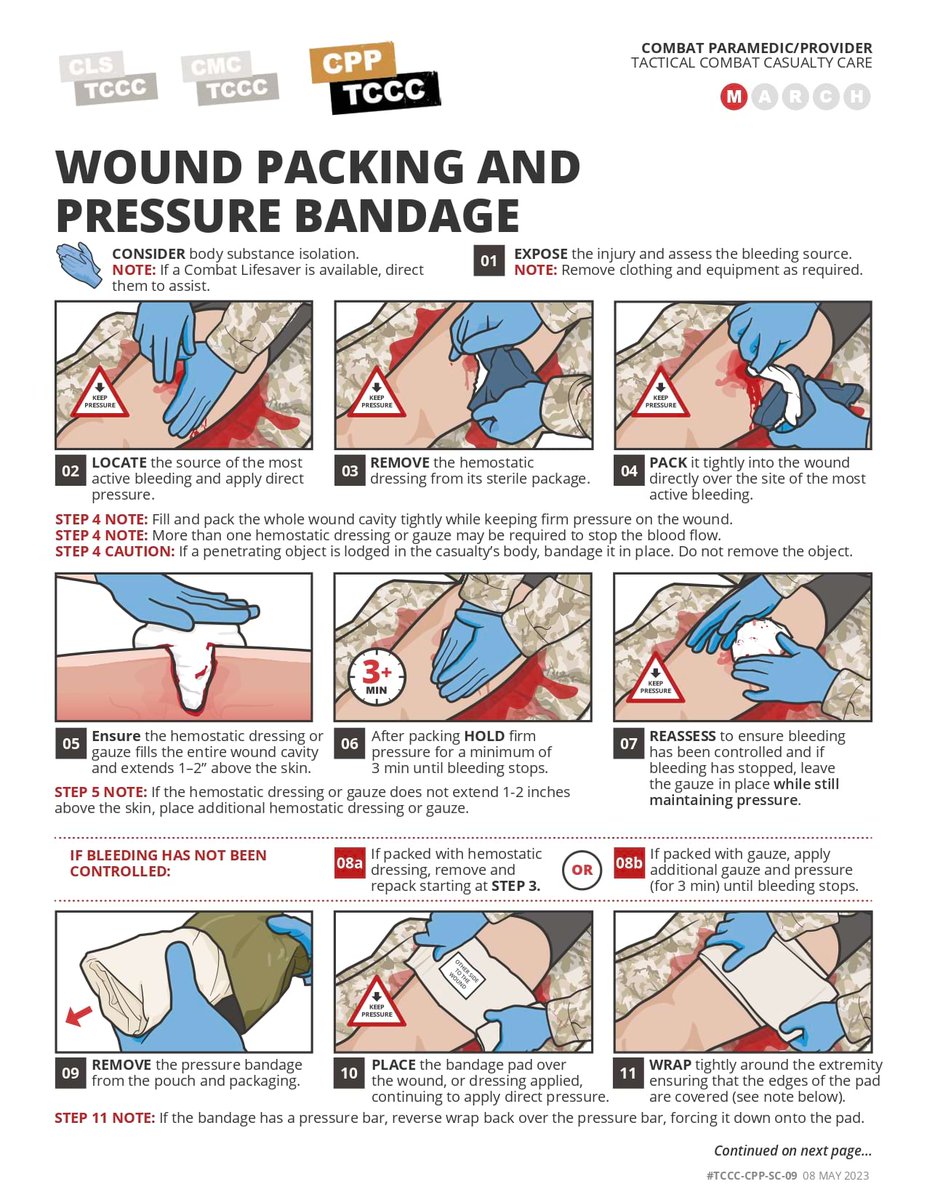
"Direct pressure: Application of dressing material and pressure directly on a wound (for minimal bleeding).
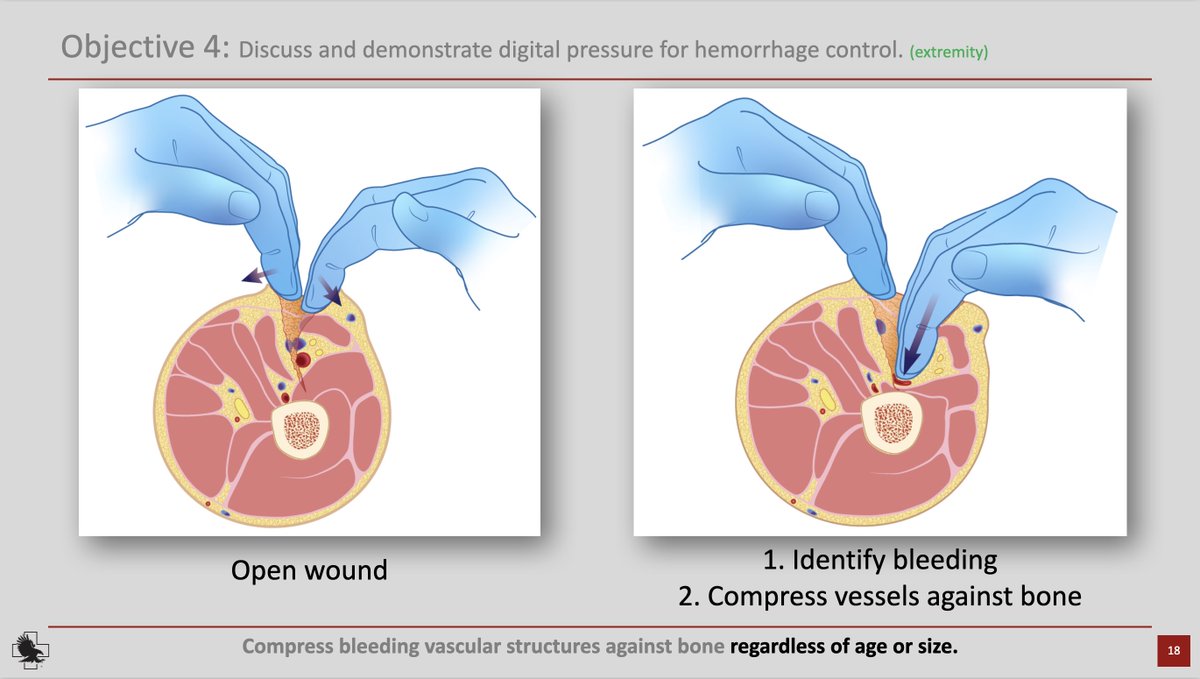
Digital pressure: Identification (visual or tactile) of bleeding vessel (s) with fingertip(s) pressing vessel(s) against the bone for moderate to severe bleeding).
Wound packing: In conjunction with digital pressure, dressing material is systematically placed under fingertip(s) into wound cavity. Packing of wound is complete when cavity is entirely full (for moderate to severe bleeding).
Pressure bandage: Applied in conjunction with dressing or wound packing material, to maintain pressure on injury site (for moderate to severe bleeding).
Tourniquet: Applied to eliminate ALL extremity circulation (for life-threatening bleeding).
drive.proton.me/urls/4F5QEPY…
2
25
61
10,983
M*A*S*H Recommended
Falling to Your Level of Training
How do you know, that you know, what you know?
Be tested and find out...
drive.proton.me/urls/95JYRMR…
3
6
311
TCCC Guidelines

M*A*S*H Recommended
TCCC Clinical Guidelines
#TCCCClinicalGuidelines
Current Tactical Combat Casualty Care (TCCC) Guidelines as of 25 JANUARY 2024. The TCCC
Guidelines are the standard of care for the modern battlefield.
drive.proton.me/urls/YCBNGMJ…
1
1
146
M*A*S*H Recommended
Introduction to Tactical Combat Casualty Care (TCCC)
The overall objective of TCCC is to teach service members how to effectively treat combat casualties while preventing additional casualties and completing the mission at hand. The three phases of TCCC include care under fire, tactical field care and tactical evacuation care.
* Care Under Fire (CUF) outlines strategies using limited medical equipment to render care at the point of injury while the first responder and the casualty are still under hostile fire.
* Tactical Field Care (TFC) provides casualty care guidelines once the first responder and the injured combatant are no longer under hostile fire.
* The Tactical Evacuation Care (TACEVAC) phase begins once the casualty has been transferred to a transport aircraft or vehicle. During this phase additional medical personnel and equipment may be available to provide augmented casualty care.
The Committee on Tactical Combat Casualty Care and the Joint Trauma System continuously reviews casualty data, best practices, lessons learned, research projects and medical literature to produce a set of evidence-based, best-practice prehospital trauma care guidelines customized for use on the battlefield.
These considerations notwithstanding, at the onset of hostilities in Afghanistan, most U.S. combat medical personnel were being trained using the following civilian-based principles of trauma care:
Rendering care with no structured consideration of the evolving tactical situation
No use of tourniquets to control extremity hemorrhage
Managing external hemorrhage with prolonged direct pressure, precluding the medic from attending to other injuries or rendering care to other casualties
No use of hemostatic dressings
Two large-bore intravenous lines (IVs) started on all patients with significant trauma
Treatment of hypovolemic shock with large-volume crystalloid fluid resuscitation
No special considerations for traumatic brain injury (TBI) with respect to avoiding hypotension or hypoxia
Management of the airway in facial trauma or unconscious casualties with endotracheal intubation
No specific techniques or equipment to prevent hypothermia and secondary coagulopathy in combat casualties
Management of pain in combat casualties with intramuscular (IM) morphine—a battlefield analgesic that dates to the Civil War
No intraosseous (IO) access
No prehospital electronic monitoring
No effective nonparenteral analgesic medications
No prehospital antibiotics
No delineation of which casualties might benefit most from supplemental oxygen during tactical evacuation
Spinal precautions applied broadly to casualties with significant trauma, without consideration of tactical concerns or mechanism of injury
1
4
242
M*A*S*H Recommended
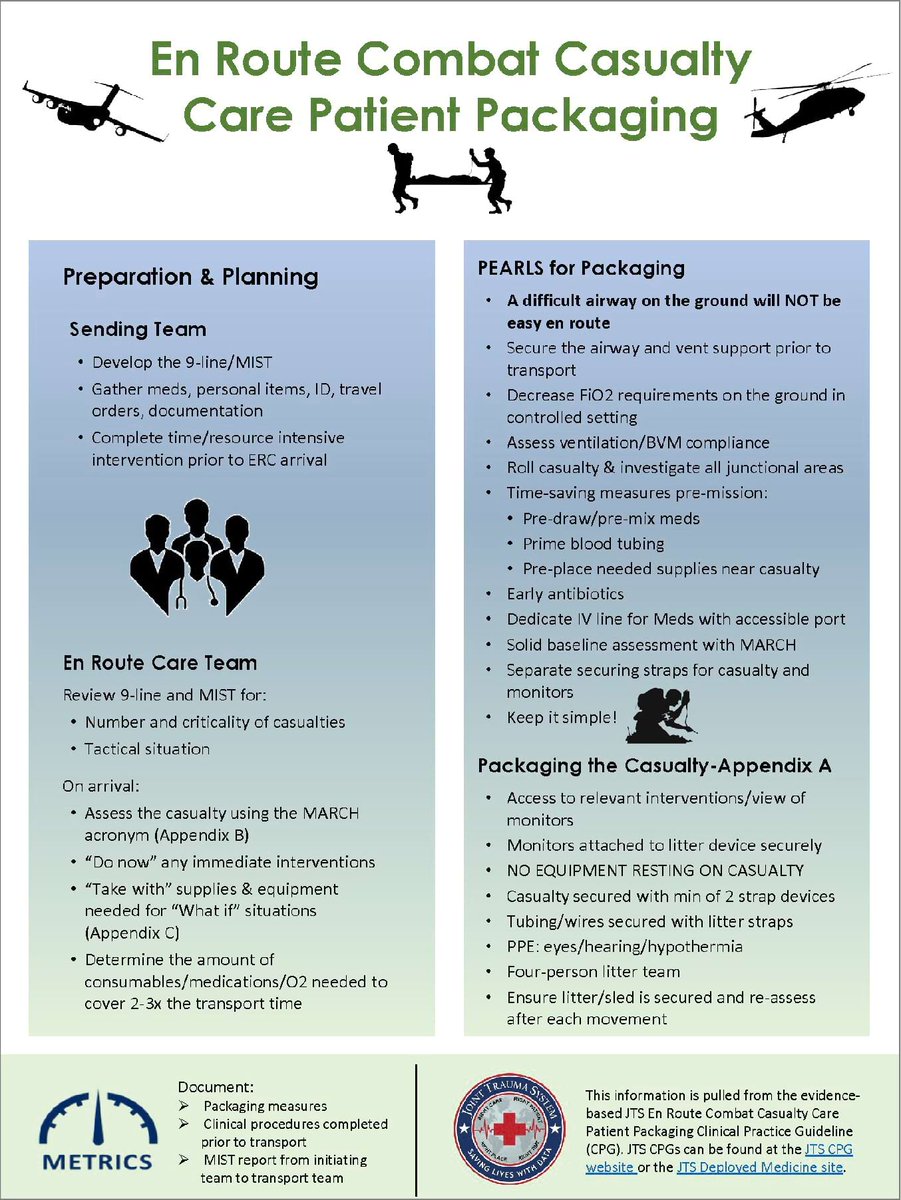
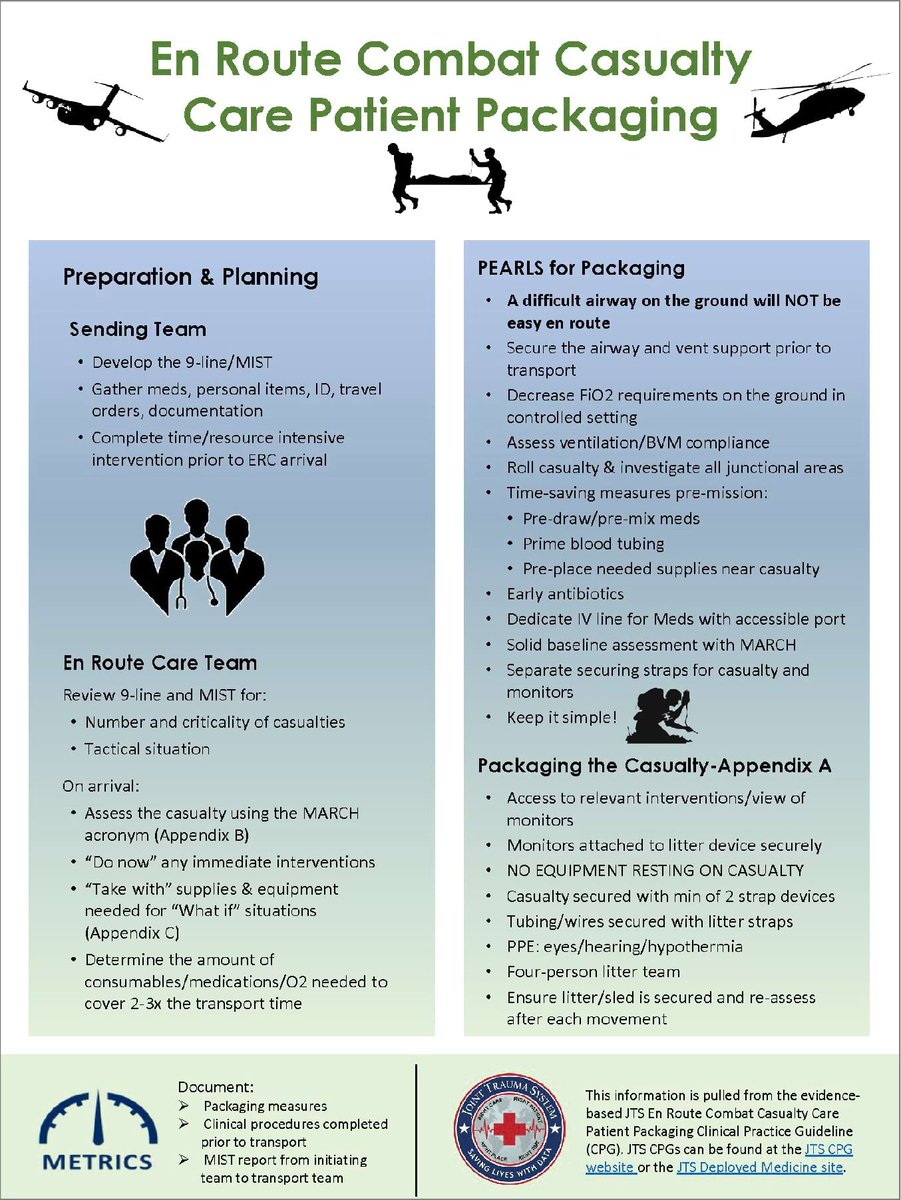
Patient Transfer: En Route Care
drive.proton.me/urls/7487ST3…
Background
Patient movement is the process which provides a continuum of care and coordinates the movement of patients from the site of injury or onset of disease, through successive roles of care, to and between medical treatment facilities (MTFs) that can meet the needs of the patient. Patients are moved only as far rearward as the tactical situation dictates and as clinical needs warrant. Prompt movement of patients to the required level of clinical care is essential to prevent morbidity and mortality. Each Service component has medical evacuation (MEDEVAC) or casualty evacuation (CASEVAC) capability to do so. Patient movement consists of three components:
~ medical regulating
~ patient evacuation
~ en route care (ERC)
En Route Care (ERC) is defined in Joint Publication (JP) 1-02, Department of Defense (DoD) Dictionary of Military and Associated Terms and JP 4-02 as the continuation of the provision of care during movement (evacuation) between the health service support capabilities in the roles of care, without clinically compromising the patient’s condition. ERC involves the provision of transitory medical care, patient holding, and staging capabilities during transport from the point of injury or onset of disease throughout the continuum of care.
To ensure the safe transport of casualties during evacuation to definitive care, patients must be adequately prepared for evacuation. The purpose of this Clinical Practice Guideline (CPG) is to provide a ready resource for those who are responsible for preparing a patient for en route care.
Patient Preparation
The goal of ERC casualty preparation is to provide the continued level of medical support as the casualty is transported throughout the battlespace and differing roles of care. Considerations for planning during transport can be categorized into groups of concerns: 1)safety, 2) access, and 3) organization. When planning for any casualty transfer, the transport team should prepare for 2-3 times longer transport time than initially projected (i.e. If the transport is anticipated to take 2 hours, plan for 4-6 hours).
Transport safety includes the safety of both the casualty and the ERC team’s interaction with the casualty. All casualties should be provided thermal regulation, visual protection, and auditory protection from the transport environment. Casualty preparation for transport can be divided into two phases: ground preparation and transport team preparation.
Ground Preparation
Prepare the patient for the transport team to arrive.
Sending facility develops the 9-Line casualty request and M.I.S.T. (Mechanism of injury, Injuries sustained, Signs/symptoms, Treatment given) report
Gather the casualty’s medications, personal effects, identification, travel orders, and documentation.
Complete any time or resource intensive interventions prior to ERC team arrival to optimize transport requirements and minimize delays.
Transport (ERC) Team Preparation
Consists of planning and execution phases.
Planning Phase
This phase begins upon receipt of the 9-line medical evacuation request and M.I.S.T. report. Each aspect of the 9-Line request is important for the transport team, but emphasis is placed on the number and criticality of casualties, as well as the tactical situation. Accuracy is key - as the incoming ERC team must ensure that the casualty load will not overwhelm their resources or capabilities. The ERC team’s clear understanding will lead to their arrival with the correct resources and the patient disposition to the appropriate medical facility.
Execution Phase
During this phase, time is of the essence. Upon arrival at the initiating facility, the ERC team should contact the provider requesting the evacuation. The goal is to decrease the amount of time spent preparing the patient and rapidly move to transport. The ERC team will assign tasks to ensure that each member is appropriately utilized. Tasks that should be completed by the team include receiving report, assessing the patient, validating the movement of the casualty, verifying correct packaging in preparation for departure, packaging the patient for transport, and development of the en route plan.
1. Report and Patient Assessment
The ERC team will guide the report and assessment process. The use of the MARCH acronym (Appendix B) can assist both the sending and transport teams in communicating the appropriate information in the least amount of time. Often the priorities of the sending team differ from those of the ERC team. The ERC team should receive report, ask questions pertinent to the status and transfer of the patient, and then provide an opportunity for the sending team to provide additional information. If hand off must occur in high ambient noise environments such as engines running on/off-load or helicopter hot-load sending, provider should point to each wound(especially areas of controlled or suspected hemorrhage) with confirmation of receiving team of wounds/injuries. Use of a communication device (such as the Atlantic Signal Tactical Medic Intercom) that allows sending and receiving team aircraft-side verbal communication is hugely beneficial and units/teams should coordinate this beforehand.
Once the report has been completed, an assessment will be performed to confirm findings and interventions. This assessment will develop the “Do Now” status of the casualty. The “Do Now” criteria are the current MARCH findings from the report and the assessment that need immediate intervention to prepare for transport. As each of the “Do Now” criteria are identified, secondary logistic supply needs and assessment needs are developed.
2. Validate the Movement of the Casualty
The findings of the ERC casualty assessment assist in the validation of the decision to transport the casualty. The JTS CPG on the Interfacility Transport of Casualties Between Theater MTFs gives clear guidance on the resuscitation goals that should be followed to identify when a casualty is safe to transfer. If one or more of these goals is not met, a plan must be developed to optimize the casualty in accordance with resources and tactical situations.
3. Verify Correct Packaging in Preparation for Departure
Once the casualty is validated for movement, supply needs can be filed under the “Take With” portion of casualty transport planning. The goal of this portion of the planning process is to ask the “what if“ question for each of the casualty’s interventions. This item list will include back-up support devices and batteries, dressing reinforcement supplies, next step interventions, medications for continued treatment, and documentation.
4. Packaging the Patient for Transport
Package the casualty to ensure safety of the casualty and team, access to all relevant interventions, and organization of resources. Monitors should be placed on the litter structure or attached to a litter device to ensure that NO EQUIPMENT IS RESTING ON THE CASUALTY, it is fully secure to the litter system, and that all team members have access to and can view the monitors. Securing devices, such as litter straps used for equipment, should not be used for the casualty. All casualties should be secured with a minimum of two strap style devices. It is also recommended that any tubing or wires be secured with litter straps to prevent snaring or disconnection during movement.
5. Development of the “En Route” Plan
Develop the assessment protocol for your casualty while in transport. This is an opportunity for the team to clearly subdivide tasks and ensure that all aspects of casualty care will be met. It is key to remember that vital signs should be checked regularly. This will create a pattern repetition or “battle rhythm” for the transport period.
Documentation and report are developed from the “en route” portion of the casualty transport plan. Depending upon the status and required effort of casualty care during transport, documentation on the DD1380 or DA4700 may prove to be difficult to maintain. It is imperative that, the team monitor, and document vital signs regularly as required by patient acuity, administer, and document medications, and perform and document any interventions in order that they have been completed in the casualty care record.
Pearls Of Preparation
A difficult airway on the ground will NOT be easy to maintain en route. Secure the airway and ventilator support as needed prior to transport.
Decrease FiO2 requirements on the ground in a controlled setting to ensure proper O2 levels and allocation of limited resources en route.
Predrawn/premixed medications, primed blood tubing, taping of reinforcement bandages near wound, pelvic binders, and preplaced tourniquets are all examples of time saving measures to be optimized on the casualty prior to transport. Time is an enemy in the provider resource constrained transport environment.
Early antibiotics can prevent long-term complications, ensure your casualty has antibiotic coverage or have a plan to initiate coverage when appropriate.
Dedicate an intravenous line for medication administration. Separate, mark, and place the administration port somewhere accessible to all team members during the transport.
During assessment, ensure that the casualty is rolled, all junctional areas are investigated for injuries, and that all team members auscultate lung fields, palpate chest for expansion, and assess compliance of bag valve mask ventilation.
Establish a solid baseline assessment with your team using the MARCH acronym. This will act as supporting problem solving battle rhythm for your team en route.
Keep it simple! Use practical and manageable interventions to optimize your casualty en route.
Use separate securing straps and devices for the casualty and any monitors. Remember casualty safety and security is the priority.
Equipment
En route care of patients requires adequate equipment to ensure safe and successful transport. Certain information such as length of flight, number of patients to be transferred, and severity of patient condition should be taken into consideration when deciding the type and number of equipment to be used. The goal of preparing equipment for patient transport is to ensure all necessary items are accounted for, both consumable and non-consumable.
In general, each patient will require:
~ Vital signs monitoring device with both invasive and non-invasive capabilities
~ External suction machine
~ A ventilator, depending on the patient’s respiratory status
Models of these pieces of equipment may vary between each service depending on availability. Additional items should be available so that for each possible equipment failure or for deterioration of the patient there is a backup plan and the proper materials available for these plans. For example, if the external suction machine fails, a manual suction should be available.
The length of the transport will determine the amount of medication and number of consumables that should be brought with the ERC team. At minimum, twice the length of the transport should be planned for when packing items. Oxygen needs and consumption rate should be calculated prior to transport to ensure enough supply is available for all legs of the transport. For example, the flight time may be 15 minutes, but the ground transport time from the landing zone to the next echelon of care may be an additional 20 minutes.
Consumable equipment is that which expires or cannot be reused on another patient. For all non-consumable items, fully charging batteries and performing any function checks should be ensured before transport. Although some platforms have the ability to charge the equipment, it is not guaranteed on every platform. These items must be properly inspected by biomedical per the maintenance requirement recommended by the company of each respective piece of equipment.
Non-consumable equipment should be secured on the patient litter or transportation device so that the ERC team members can view them during transport. Equipment may be secured down by litter straps, ratchet straps, tape, or other securement devices. Consumables may be carried by the ERC team members via bag or backpack or may be prestaged in the transport platform.
Guidance on equipment, consumables, medications, and fluids can be found in Appendix A. Quantities of each have been left out as it will vary by transport. Although not all items on the list will need to be included for every transport, supplies needed for potential emergencies during transport should be considered.
Patient Safety
Moving a patient from one echelon of care to another requires mitigation of safety risks through the use of personal protective equipment (PPE). PPE is determined, in part, by the mode of transportation and terrain. PPE must be applied prior to transport. Land, sea, and air are possible transport environments via ruck, truck, boat, or ship, rotary or fixed wing platforms.
Critical thought must be used when considering the appropriate protective equipment which may include but not limited to:
~ Hearing protection (single or double)
~ Eye protection (may or may not be ballistic grade)
~ Cranial protection (helmet or cranial)
~ Personal flotation device or life preserver unit
~ Hypothermia, commercial or standard warming (i.e. Hypothermia Prevention Management Kit (HPMK), wool blankets)
~ Securing straps to transport device.
Patient safety considerations also must be exercised when moving the patient to, from, and within the transportation platform. The patient must be properly secured to the litter or sled prior to movement. The securing devices must be reassessed after each movement to ensure all interventions are still in place. Consideration must also be given to have adequate numbers of personnel to move the patient from one echelon to another. A four-person litter team, directed by a medic, is the safest option when moving patients on a NATO litter. After the patient is transferred to a platform for transport, the final consideration is to ensure the litter or sled is secured to the conveyance. Though optimal, this final consideration may be omitted for the operational environment. If transporting via aircraft, work with air crew to determine the best patient position and securement method.
Performance Improvement (PI) Monitoring
Intent (Expected Outcomes)
Patient packaged to mitigate secondary injury (e.g., hypothermia prevention, hearing & eye protection, pressure injury prevention).
Completion of lifesaving interventions prior to transport.
MIST report given by the initiating team to the transport team.
All lines and tubes secured (e.g., endotracheal tube, intravenous line, Foley catheter, chest tube).
Vascular access immediately available.
Performance / Adherence Measures
Complete documentation of patient packaging measures.
Complete documentation of clinical procedures completed prior to transport.
Documentation of MIST report from the initiating team to the transport team.
Data Source
Patient record DD FORM 1380 or other relevant patient document.
Department of Defense Trauma Registry
System Reporting & Frequency
The above constitutes the minimum criteria for PI monitoring of this CPG. System reporting will be performed annually; additional PI monitoring and system reporting may be performed as needed.
The system review and data analysis will be performed by the JTS Chief and the JTS PI team.
Responsibilities
It is the ERC team leader’s responsibility to ensure familiarity, appropriate compliance, and PI monitoring at the local level with this CPG.
REFERENCES
Joint Health Services, Joint Publication 4-02. Dec 11, 2017.
U.S. Department of the Air Force. Aeromedical Evacuation Equipment Standards (AFI10-2909). Jul 23, 2013.
Headquarters Department of the Army. Medical Evacuation (ATP 4-02.2) Army Techniques Publication No. 4-02.2 Aug 12, 2014.
Headquarters Department of the U.S. Army. Casualty Evacuation (ATP 4-25.13) Army Techniques Publication No. 4-25.13, Feb 9, 2013.
U.S. Department of the Air Force. En Route Care and Aeromedical Evacuation Medical Operations (AFI 41-307). Jan 7,2017.
JTS: Interfacility Transport of Patients Between Theater Medical Treatment Facilities
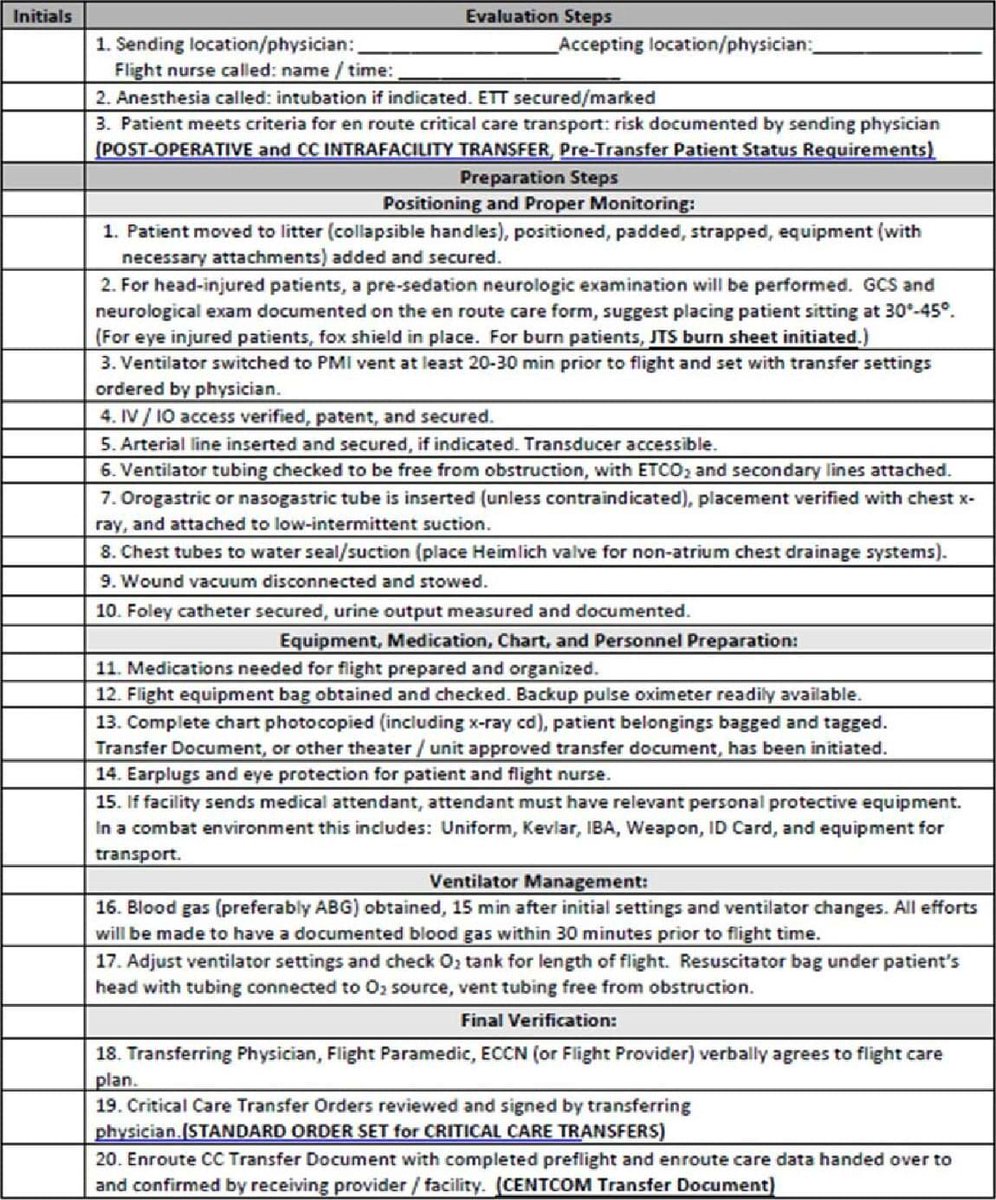
Appendix A: Patient Packaging Checklist
Source: U.S. Army Aeromedical Evacuation Standard Medical Operating Guidelines, CY24 Version, Published 1 Feb 2024
PRE-FLIGHT CHECKLIST
(for Critical Care and Post-Surgical Transfers)
Once the decision is made to transfer a patient and an accepting physician has been obtained, the following steps will be taken to prepare the patient for transport:
Appendix B: M A R C H
MASSIVE HEMORRHAGE
Address major hemorrhage threats and sending interventions
Mark all bleeding on dressings
Pre-stage loose tourniquet above prior arterial bleed for easy application during transport if re-bleed occurs
AIRWAY
Ensure that the airway is secured for flight with bilateral lung sounds and EtC02 monitoring.
Cuff inflated and confirmed with manometer/ secured appropriately
Prepare emergency airway device (BVM with mask, re-intubation, supraglottic, surgical airway)
RESPIRATION
Perform Breathing assessment
Check recent arterial blood gas and compare results against current ETCO2 monitoring
**Ensure collaborative assessment for chest expansion and bag valve compliance
Placing the patient on the transport ventilator should be weighed with oxygen consumption.
CIRCULATION
Roll the casualty to assess posterior prior to transport!
Visually inspect perineal area for hemorrhage and injury.
Assess all junctional areas for bleeding.
Assess and mark all distal and central pulses, consider doppler prior to transport if necessary.
Ensure a minimum of two IV access and flush saline locked sites to ensure patency. If using IO, ensure continuous security of the device.
**Place pelvic binder or junctional tourniquets for all thoracic and abdominal injuries, as well as any traumatic lower leg amputations.
If necessary, ensure arterial catheter security and continuity, and arterial pressure monitoring system. Best practice to be secured with suture and adequate dressing.
HYPOTHERMIA
Ensure wet clothing is removed and place patient in an Absorbent Patient Litter System or HPMK if available. If only sheets or blankets are available, place one underneath and on top of patient for full coverage.
Appendix C: En Route Equipment List
Equipment
Vitals monitor
Suction
Ventilator
Oxygen tanks
Consolidated PT support system (alternate to all above equipment)
Blood/fluid warming system
Defibrillator (if not part of vitals monitor)
IV Pumps
Consumables
Endotracheal Tubes
NPA
OPA
Cricothyrotomy kit
10cc Syringe
Soft tip suction (or in-line suction if available)
Suction tubing
BVM
LMA
Extra O2 Tubing
Tension Pneumothorax needles
Heimlich valve
Scalpel
IV start kits
10cc NS flushes
Chux pads
Tourniquets
Pressure bag
IV tubing
Blood tubing
Blood warmer with tubing
Back up handheld suction
Commercial Blood container/Vampire box if traveling with blood
APLS or HPMK
Thermal Blanket
Eye protection
Ear protection
Tape
Transfer needles
Medications & Fluids
Blood Products (Best: Whole Blood, Better: 1:1:1 if available, Good: pRBC, plasma)
IV Fluids – Lactated Ringer's and normal saline
3% NaCL
Analgesia, sedation, antiemetic medications (consider use of rigid case to carry medication vials and syringes to avoid accidental waste)
Calcium
Appendix D: Telemedicine / Teleconsultation
Appendix E: Information Regarding Off-Label Uses In CPGs
Purpose
The purpose of this Appendix is to ensure an understanding of DoD policy and practice regarding inclusion in CPGs of “off-label” uses of U.S. Food and Drug Administration (FDA)–approved products. This applies to off-label uses with patients who are armed forces members.
Background
Unapproved (i.e. “off-label”) uses of FDA-approved products are extremely common in American medicine and are usually not subject to any special regulations. However, under Federal law, in some circumstances, unapproved uses of approved drugs are subject to FDA regulations governing “investigational new drugs.” These circumstances include such uses as part of clinical trials, and in the military context, command required, unapproved uses. Some command requested unapproved uses may also be subject to special regulations.
Additional Information Regarding Off-Label Uses In CPGs
The inclusion in CPGs of off-label uses is not a clinical trial, nor is it a command request or requirement. Further, it does not imply that the Military Health System requires that use by DoD health care practitioners or considers it to be the “standard of care.” Rather, the inclusion in CPGs of off-label uses is to inform the clinical judgment of the responsible health care practitioner by providing information regarding potential risks and benefits of treatment alternatives. The decision is for the clinical judgment of the responsible health care practitioner within the practitioner-patient relationship.
Additional Procedures
Balanced Discussion
Consistent with this purpose, CPG discussions of off-label uses specifically state that they are uses not approved by the FDA. Further, such discussions are balanced in the presentation of appropriate clinical study data, including any such data that suggest caution in the use of the product and specifically including any FDA-issued warnings.
Quality Assurance Monitoring
With respect to such off-label uses, DoD procedure is to maintain a regular system of quality assurance monitoring of outcomes and known potential adverse events. For this reason, the importance of accurate clinical records is underscored.
Information to Patients
Good clinical practice includes the provision of appropriate information to patients. Each CPG discussing an unusual off-label use will address the issue of information to patients. When practicable, consideration will be given to including in an appendix an appropriate information sheet for distribution to patients, whether before or after use of the product. Information to patients should address in plain language: a) that the use is not approved by the FDA; b) the reasons why a DoD health care practitioner would decide to use the product for this purpose; and c) the potential risks associated with such use.


2
3
686
M*A*S*H Recommended
Resources for Medical Centers
ASPR TRACIE
"Brought to you by HHS ASPR, the Technical Resources, Assistance Center, and Information Exchange (TRACIE) was created to meet the information and technical assistance needs of regional ASPR staff, healthcare coalitions, Medical Reserve Corps (MRC) units, healthcare entities, healthcare providers, emergency managers, public health practitioners, and others working in disaster medicine, healthcare system preparedness, and public health emergency preparedness."
files.asprtracie.hhs.gov/doc…
Supplies List
asprtracie.hhs.gov/dash-tool
"Mass violence incidents require efficiency and coordination among multiple response entities. Efforts may need to be directed toward doing the greatest good for the greatest amount of people, which is counter to day-to-day trauma triage. These ASPR TRACIE-developed resources can help our stakeholders prepare for, respond to, and help their communities recover from these traumatic incidents. If you are unable to find what you are looking for, or if you would like to submit a resource for possible inclusion, contact our Assistance Center."
files.asprtracie.hhs.gov/doc…
3
4
163
M*A*S*H retweeted

Mar 2
👀

🚨HEZBOLLAH THREAT🚨
FT BRAGG AREA
Southern Pines
Research Triangle
3 - 6 Weeks Time-Frame
EAST COAST & LA
Ex-pat Communities
2
7
541
Resources you need.
M*A*S*H Recommended
Printable Resources for Everyone: Skill Cards
Download and Print for Your Medical Library
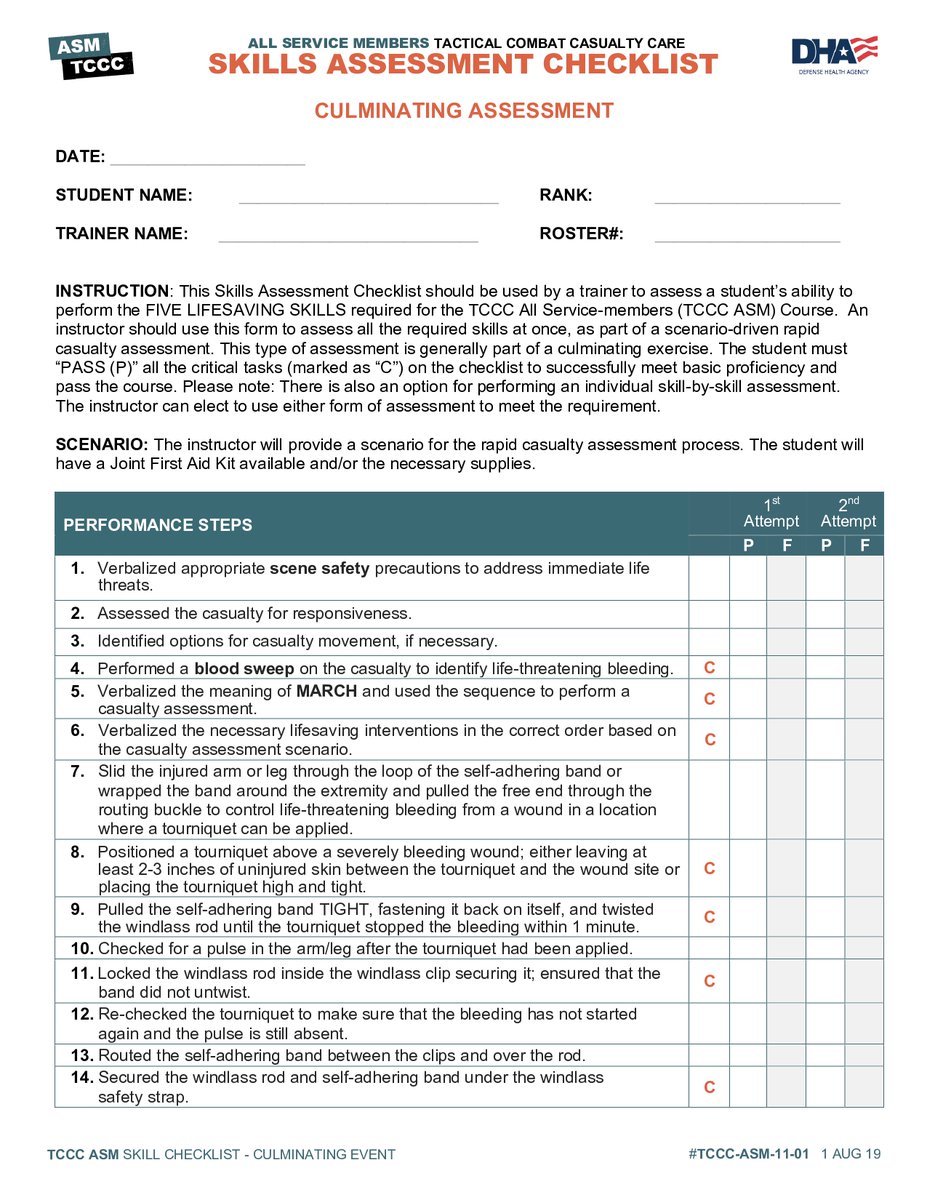
This collection contains the Tactical Combat Casualty Care Standardized Training Program for All Service Members (TCCC ASM) developed by the Joint Trauma System, part of the United States Health Agency.
Skill Instructions
Introduction:drive.proton.me/urls/MM0DRVQ…
Speaker Notes: drive.proton.me/urls/64EKVWS…
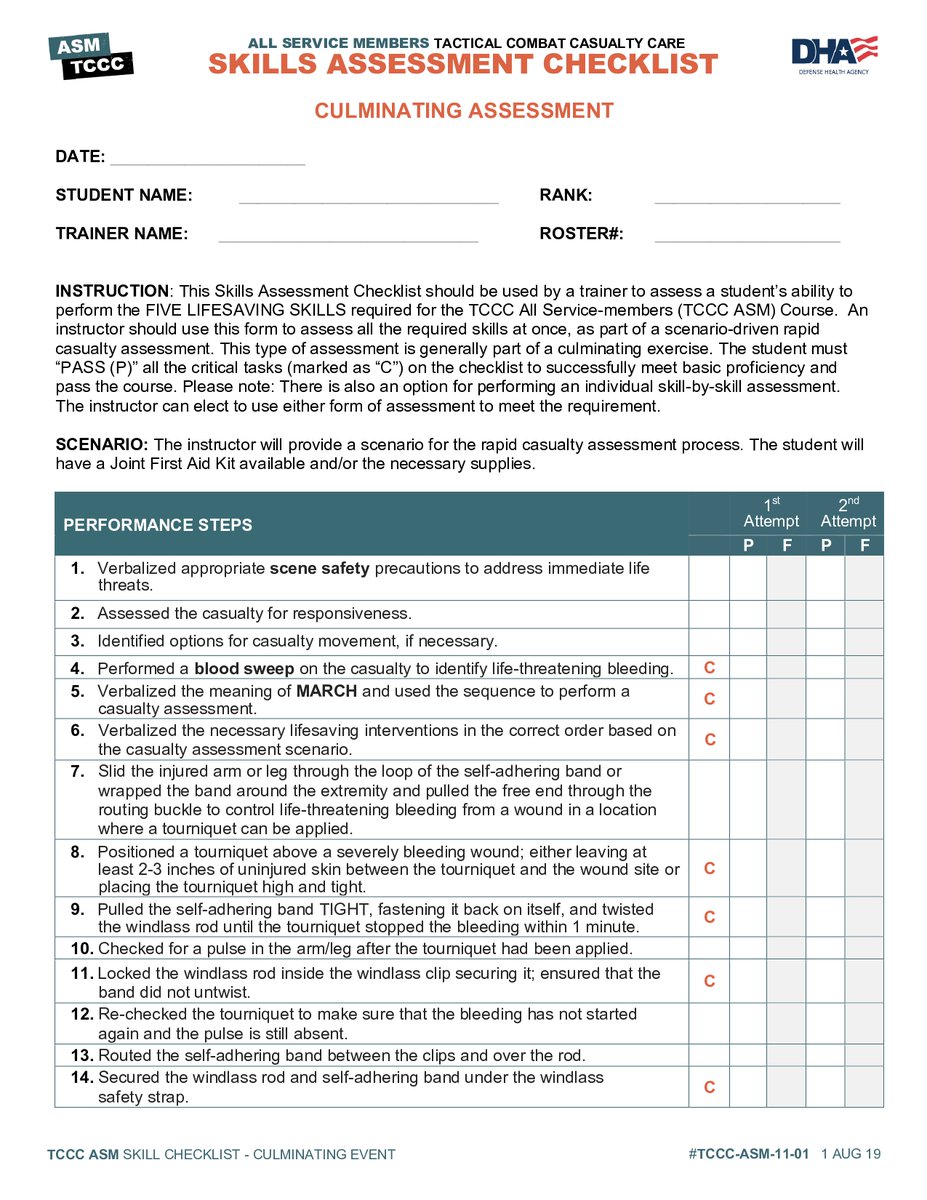
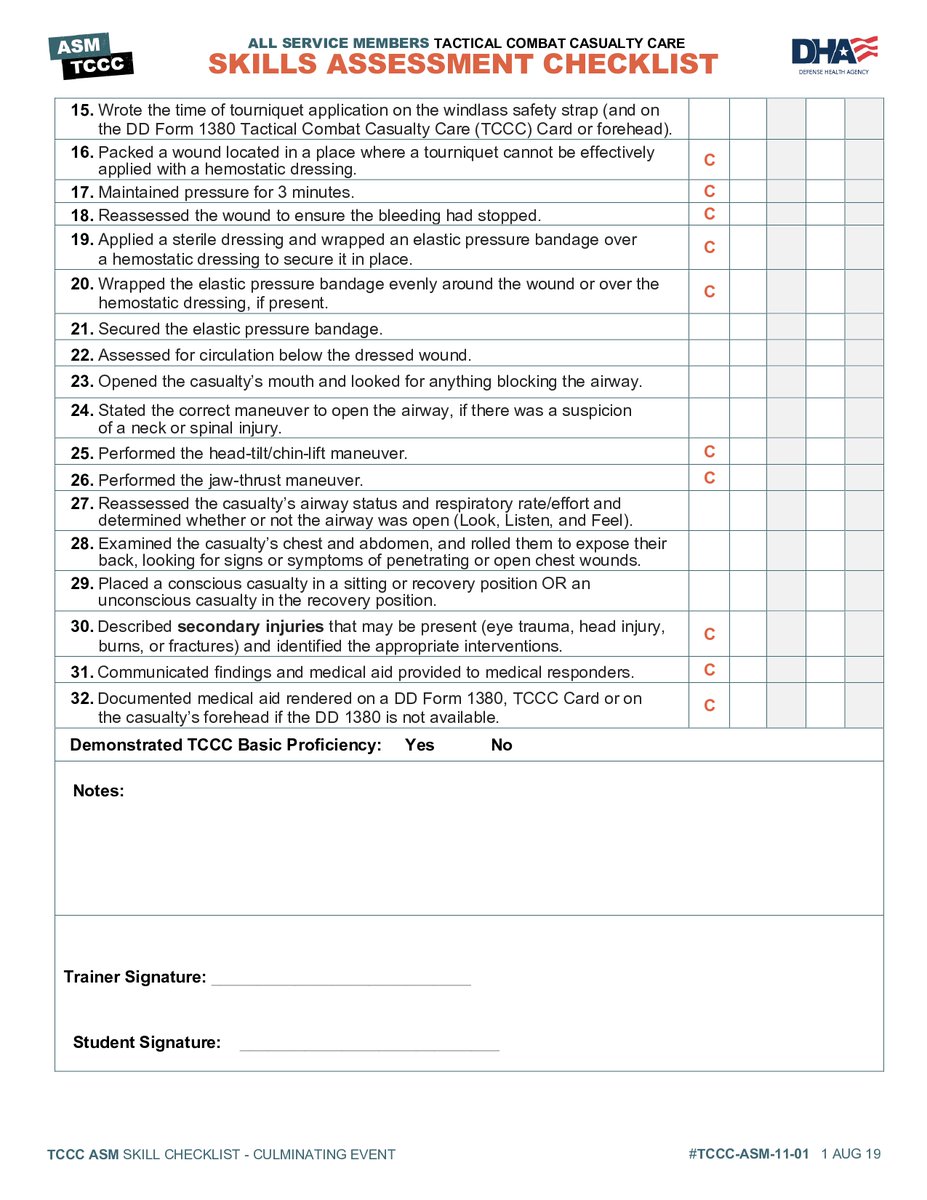
Skill Checklists
Culminating Event: drive.proton.me/urls/CAH7W30…
Individual Skill-by-Skill Assessment: drive.proton.me/urls/2SBJ8PT…
Skill Cards
Rapid Casualty Assessment: drive.proton.me/urls/5CGQ6MV…
Tourniquet Application: drive.proton.me/urls/BX6BVZQ…
Pressure Bandage: drive.proton.me/urls/2SNRNAA…
Wound Packing: drive.proton.me/urls/VK8SERK…
Airway Maneuvers: drive.proton.me/urls/1SCWEHA…
All 5 Life Saving Skills: drive.proton.me/urls/T95SVYW…
13
M*A*S*H Recommended
Printable Resources for Everyone: Skill Cards
Download and Print for Your Medical Library
This collection contains the Tactical Combat Casualty Care Standardized Training Program for All Service Members (TCCC ASM) developed by the Joint Trauma System, part of the United States Health Agency.
Skill Instructions
Introduction:drive.proton.me/urls/MM0DRVQ…
Speaker Notes: drive.proton.me/urls/64EKVWS…
Skill Checklists
Culminating Event: drive.proton.me/urls/CAH7W30…
Individual Skill-by-Skill Assessment: drive.proton.me/urls/2SBJ8PT…
Skill Cards
Rapid Casualty Assessment: drive.proton.me/urls/5CGQ6MV…
Tourniquet Application: drive.proton.me/urls/BX6BVZQ…
Pressure Bandage: drive.proton.me/urls/2SNRNAA…
Wound Packing: drive.proton.me/urls/VK8SERK…
Airway Maneuvers: drive.proton.me/urls/1SCWEHA…
All 5 Life Saving Skills: drive.proton.me/urls/T95SVYW…
1
6
12
1,170
EMS just outside? Know what to do.
M*A*S*H Recommends
What To Do if EMS is Waiting Just Outside
#EMS #EmergencyMedicalServices #CasualtyCollectionPoints #OrganizeTreatmentofCasualties
The Problem
When you are in an Active Sh**ter Event, standard protocol for most Emergency Medical Services is to post around the event and wait for police to secure the area and then go in, once secure to treat the wounded.
EMS must stay safe while they treat the wounded. If they are injured or killed attempting to treat casualties before the 'Scene is Safe’, they could become a casualty, which helps no one. This creates a moral issue first responders often face, delayed care translates to poor outcomes for the injured. This problem is compounded in a Complex Coordinated Terror Attack.
The Solution
Casualty Collection Points (CCP) are an impactful solution to this dilemma. It is a way to organize casualties and medical treatment in the field.
If you find yourself on the X, but are not under direct fire, coordinate efforts to move casualties to designated points just outside of the CCTA zone. Have EMS bring their gear and treat casualties in a Casualty Collection Point while Police and Military protect EMS and the casualties while they work.
Here is an Overview of How CCPs Work
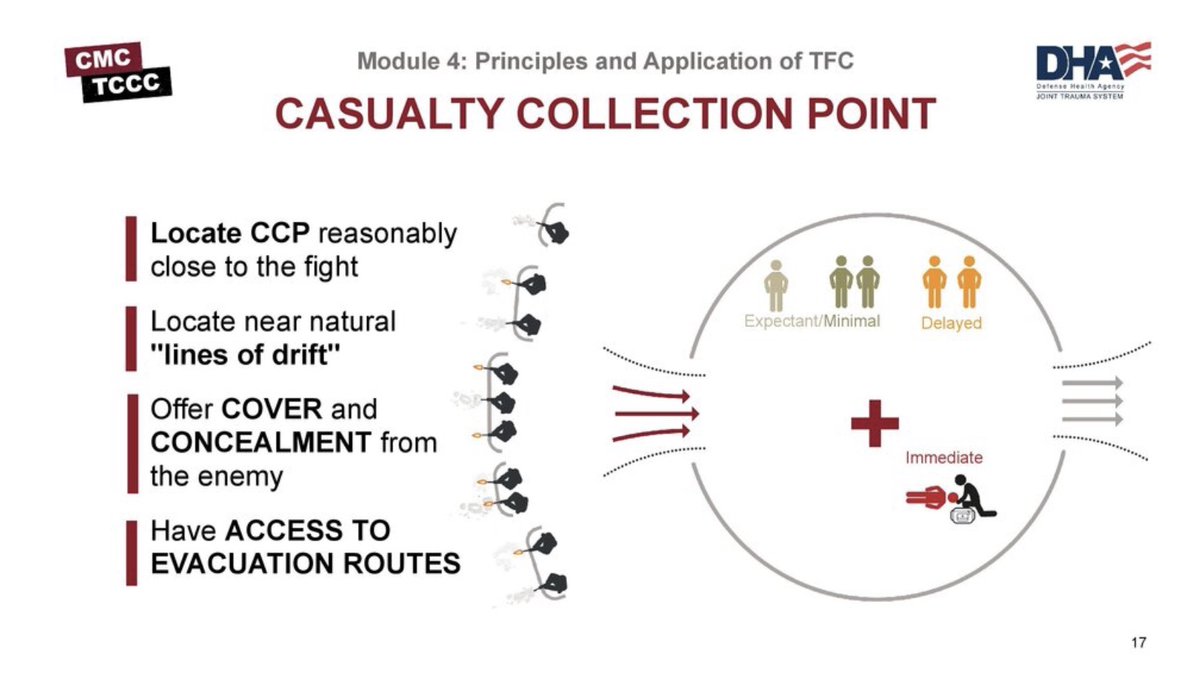
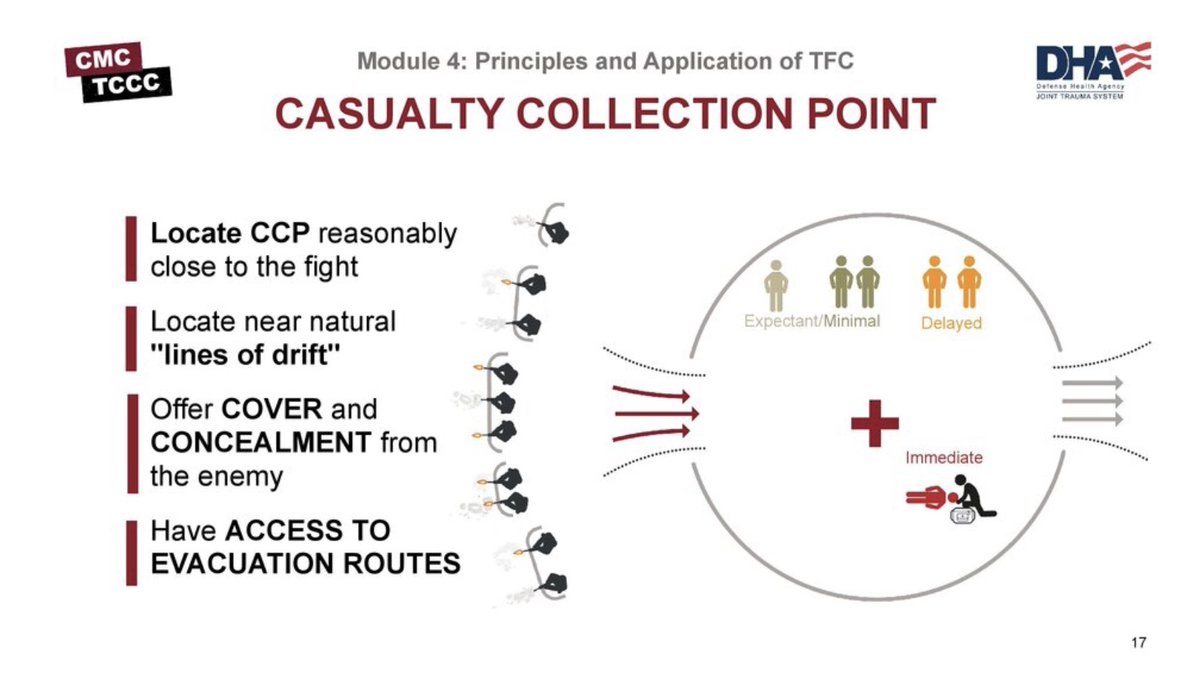
Tactical Casualty Collection Points (CCPs) should be established reasonably close to the fight where casualties are likely to occur, be near natural “lines of drift,” provide relative cover and concealment from the enemy whenever possible and have access to evacuation routes.
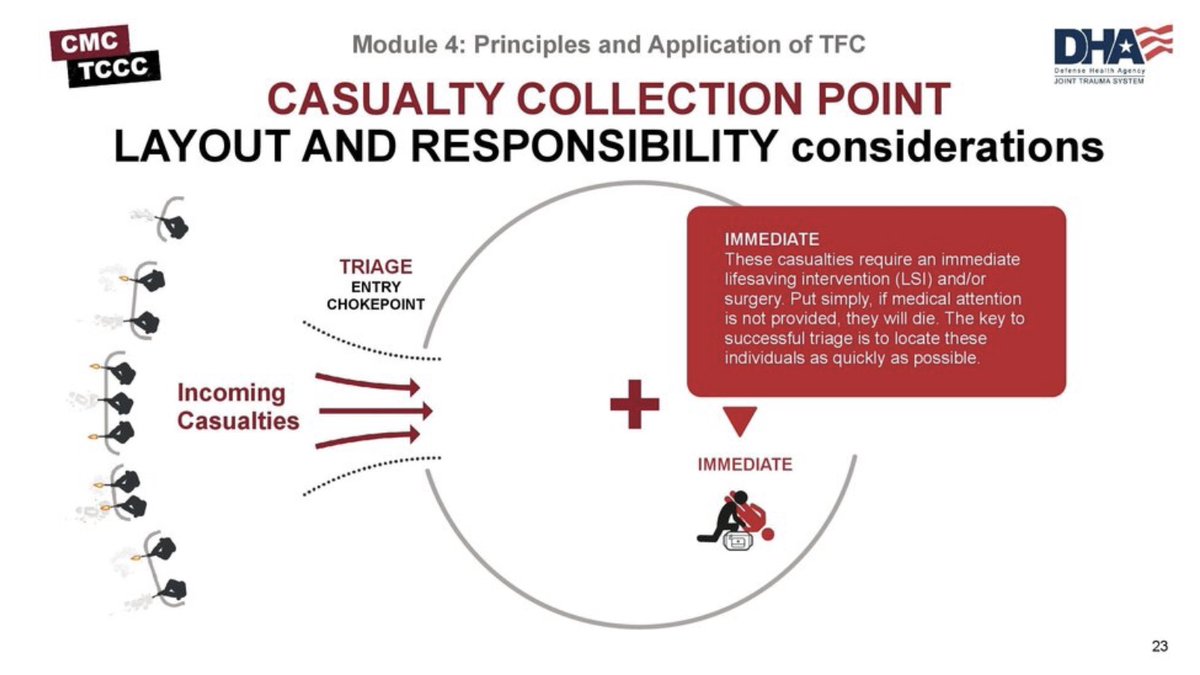
Medical personnel are responsible for everything inside the CCP, including triage, casualty treatment and monitoring, packaging and staging casualties for evacuation, requesting assistance as needed from other unit assets, providing guidance and recommendations to leadership on casualty management and evacuation, medical equipment and supplies. In an ideal layout, there are separate entry and exit points (which are potential chokepoints) to control casualty flow through the CCP, similar to what is seen in this example.
Establish a security perimeter in accordance with unit tactical standard operating procedures and/or battle drills. Casualty movement will be provided by unit personnel in accordance with unit tactical operating procedures and/or battle drills. Triage/chokepoint will be unit leadership categorizing patients. Patients will then be placed in the CCP, which should be marked/identified.
IMMEDIATE
These casualties require an immediate lifesaving intervention (LSI) and/or surgery. Put simply, if medical attention is not provided, they will die. The key to successful triage is to locate these individuals as quickly as possible.
DELAYED
This category includes those wounded who are likely to need surgery but whose general condition permits delay in surgical treatment without unduly endangering the life, limb, or eyesight of the casualty. Sustaining treatment will be required (e.g., oral or IV fluids, splinting, administration of antibiotics, and pain control) but can possibly wait.
MINIMAL
Casualties in this category are often referred as the “walking wounded.” Although these patients may appear to be in bad shape at first, it is their physiologic state that tells the true story. Casualties who fit into the minimal category may not present themselves until late in the triage process.
EXPECTANT
Casualties in this category have wounds that are so extensive, that even if they were the sole casualty and had the benefit of optimal medical resources, their survival would be highly unlikely. Even so, expectant casualties should not be neglected. They should receive comfort measures and pain medication if possible, and they deserve re-triage as appropriate.
The medic is in charge of categorizing the casualties by evacuation category (Urgent, Priority, Routine).
URGENT
Evacuation within 2 hours, denotes a critical, life-threatening injury. Suggestions for different injury patterns in this category are:
~ Significant injuries from a dismounted IED attack
~ Gunshot wound or penetrating shrapnel to chest, abdomen, or pelvis
~ Blunt chest, abdominal, or pelvic trauma with suspected noncompressible hemorrhage
~ Ongoing airway difficulty
~ Ongoing respiratory difficulty
~ Unconscious casualty
~ Known or suspected spinal injury
~ Hemorrhagic shock
~ External bleeding that is difficult to control
~ Extremity injury with absent distal pulses
~ Moderate/severe TBI
~ Burns greater than 20% TBSA
PRIORITY
Evacuation within 4 hours, serious injury. Suggestions for different injury patterns in this category are:
~ Isolated, open extremity fracture with bleeding controlled
~ Extremity injury with a tourniquet in place
~ Penetrating or other serious eye injury
~ Significant soft-tissue injury without major bleeding
~ Burns of 10% to 20% TBSA
ROUTINE
Evacuation within 24 hours, mild to moderate injury. Suggestions for different injury patterns in this category are:
~ Concussion (mild TBI)
~ Gunshot wound to extremity - bleeding controlled without tourniquet
~ Minor soft-tissue shrapnel injury
~ Closed fracture with intact distal pulses
~ Burns of <10% TBSA
Not every situation allows for separate entry and exit points (as seen in the first example); it is easy to see how having a single entry and exit point for the CCP could create a problem with casualty flow if casualties continue to arrive as others are being moved out to the evacuation point.
Nonmedical unit leadership are typically responsible for security, casualty flow and movement, and everything outside of the CPP. Also, they are responsible for providing assistance to medics with augmentation, directing aid and litter teams, gathering and redistributing casualty equipment and sensitive items, providing accountability and reporting to higher authority, requesting evacuation and establishing CASEVAC or MEDEVAC link-up points, and managing KIA remains.
KIA Morgue should be out of sight from casualties suffering life-threatening trauma. Ensure to have at least one first responder present to protect and guard KIA personnel.
This transition includes preparing the casualty for transport on one of a number of possible evacuation platforms aircraft, ground vehicles, or water craft. Some of the essential elements in this preparation are securing loose dressings and straps, casualty marking, and completion of the TCCC Casualty Card. These actions will help to ensure a smooth handover of the casualty to TACEVAC personnel. Once moving out with the casualties they will then pre-stage the casualties near the landing zone and prioritize evacuation by establishing who is Urgent, Priority, or Routine.
Medically regulated casualty movement using dedicated medical evacuation platforms. These are crewed by medical attendants and generally have more medical treatment equipment available than nonmedical platforms. MEDEVAC platforms are predesignated assets that bear Red Cross markings and carry no offensive weaponry such as rockets or missiles. MEDEVAC movements may include both clearing casualties from the battlefield and moving casualties between medical treatment facilities.
The unregulated movement of casualties from the point of wounding to the first point of surgical care (Role 2 Forward Surgical Team or Role 3 Combat Support Hospital). CASEVAC platforms are typically armed tactical assets that bear no Red Cross markings. These may be aircraft, vehicles, or maritime vessels of opportunity.
Tactical Field Care is the care rendered once the combat medic/corpsman and casualty are no longer under direct threat from effective enemy fire. This allows for the time and the relative safety for a more deliberate approach to casualty assessment and treatment.
The tactical situation is fluid and can change quickly. Maintain situational awareness. Establish a security perimeter in accordance with unit standard operating procedures and/or battle drills. Casualties with altered mental status should be disarmed and weapons communications equipment, and other sensitive items should be secured/redistributed.
In the Tactical Field Care phase, MARCH PAWS is followed for a more deliberate approach to the assessment and treatment of casualties than was possible during Care Under Fire. A full tactical trauma assessment should follow the steps of the MARCH PAWS sequence.
In TFC the Combat Medic/Corpsman should communicate with the casualty throughout assessment and treatment, communicate with other first responders, Combat Lifesavers, and medical providers regarding casualty assessment and treatment (using the DD 1380), communicate casualty status and evacuation requirements with tactical leadership, and communicate with the evacuation system (TACEVAC) including 9-line MEDEVAC requests and MIST reports.
When there are multiple casualties, the combat medic/corpsman may need to triage casualties into prioritized treatment groups (immediate, delayed, minimal, expectant) based upon severity of injuries prior to providing or assisting other first responders, combat lifesavers, and medical personnel with casualty care. The Combat Medic/Corpsman should consider MARCH in deciding how to prioritize treatment and evacuation of multiple casualties in the TFC phase of care.

2
5
954
M*A*S*H retweeted
May 28
it will be said, who would have thought they would attack such a place. from "The Gathering Storm" tfpineapple.org/tgs-book/
4
12
600
M*A*S*H retweeted

May 28
❌JIHADIST KNIFE ATTACK❌
📍Zurich, Switzerland
3x Stabbed
31 Year Old Arrested

4
12
772
M*A*S*H retweeted

May 27
Uzbeki Organized Crime Group Busted in Philadelphia on May 8
Investigators also said they recovered 24 firearms, more than 10,000 rounds of ammunition, more than 200 magazines, two 3D printers that were used to manufacture weapons, a tactical vest, an ammunition bag and more than $19,000 in cash.
The weapons included an AK-47, multiple AR-15 rifles, a desert eagle, an assault-style shotgun and a 50-caliber rifle.
The type of weapon recovered has raised serious concerns among investigators due to its potential use in large-scale acts of violence or terrorism.
May 26

Uzbeki Organized Crime Group Busted With Drugs, Guns & Anti-Helicopter Weapon In Philly.
Authorities say an alleged Uzbeki organized crime group was busted in Northeast Philadelphia after a major investigation uncovered a large-scale drug distribution and gun manufacturing operation.
Investigators seized roughly $1.5 million worth of narcotics, dozens of firearms, thousands of rounds of ammunition, ghost gun equipment, cash, and what officials described as a military-style anti-helicopter weapon during raids in the Somerton section of the city.
The type of weapon recovered has raised serious concerns among investigators due to its potential use in large-scale acts of violence or terrorism. Two suspects were arrested as the investigation remains ongoing.
By @LeeroyPress
For licensing email Leeroypress@gmail.com
4
17
35
5,267
M*A*S*H retweeted

IDF to begin conducting large scale airstrikes on Beirut.
Wouldn’t be surprised to see a wave of terrorist attacks across Europe & UK in the coming weeks.

🚨 Israel Declares War on Lebanon
PM Benjamin Netanyahu has ordered the IDF to begin airstrikes on Hezbollah targets located in the Dahiyeh district of Beirut.
Last week Israel also began remobilization of ground forces and reserve troops.
1
2
321

M*A*S*H retweeted
Jun 1
Agri-Food Systems Are Critical Infrastructure and National Security Depends on Them
This essay is from the Security & Defence PLuS Emerging Voices Series, which highlights the next generation of scholars and practitioners shaping thinking on strategy, security, and defense. The series brings together perspectives from PhD candidates and early career researchers, grounded in the complex geopolitical realities of the 21st century.
The collection explores a “Latticework of Resilience” that connects often-overlooked sectors, such as subnational diplomacy and critical infrastructure inherent in agriculture security, to the core of national security. Taken together, the essays emphasize the importance of adaptive, multidisciplinary approaches to building resilience in an increasingly complex global environment.
National security is often framed in terms of military capabilities, technological competition, and geopolitical strategy. Yet recent global disruptions – from the COVID-19 pandemic to supply chain crises and geopolitical conflicts – have exposed a critical gap in this perspective. The stability of nations depends not only on defense systems, but on the resilience of the infrastructures that sustain everyday life by ensuring economic and social well-being. Among these critical infrastructures, agri-food systems stand out as foundational yet under-recognized.
Link to article in comments ⬇️
4
4
18
1,136
M*A*S*H retweeted
🚨DOMESTIC ENEMY COLLABORATING IN RUSSIA 🚨
Candace Owens In Russia
Collaborating With Anti-USA
Russian Active Measures Dugin &
Russian Intelligence Assets
She Is Speaking At The SPIEF
Which Purpose Is Ideological Warfare Against The USA
Sources 👇
2
11
16
1,728
M*A*S*H retweeted
🚨NATIONAL SECURITY THREAT 🚨
Elizabeth Lane (Naturalized Citizen)
& Buckley Carlson
Inciting Violent Armed Revolution
Against The US Govt
In Violation Of
18 U.S.C. § 2383
@FBI_Response
Jun 3

Candace Owen’s foreign friend is on a podcast with Buckley Carlson, the brother of Tucker Carlson, calling for a violent revolution in America. She says we need violence for America to be free.
Free from what?
Also why is a foreigner allowed to stay in America when she’s calling for violence and political destabilization? She lives in Utah…
She should be deported. @SecRubio @DHSgov @ICEgov x.com/BeezlyKre/status/20622…
1
3
10
405
M*A*S*H retweeted
🚨CONSPIRACY TO COMMIT REBELLION🚨
Tucker Carlson & His Brother Buckley
Are Conspiring With Elizabeth Lane
Inciting Armed Rebellion Against
The US Government
In Violation Of USC 2383
@FBI_Response

Both Tucker Carlson and Elizabeth OnlySpies Lane (among many others) are coordinating messaging and promoting a violent overthrow of the US government.
Treason.
3
18
552