
Clinical Electrophysiologist
Joined February 2018
- Tweets 204
- Following 980
- Followers 357
- Likes 18
13 Photos and videos





11 Oct 2022
Help! Patient for both AF and PVC ablation. Mechanical AVR. On warfarin INR day of procedure 3.2, PTT normal. No baseline ACT. Weight adjusted IV heparin. First ACT over 400. Stayed about 400 for hours despite stopping IV hep. Changed ACT machines too. ??? Also ? Continue hep?
1
2
5
22 Aug 2022
75 yo, recurrent syncope, rhythm recorded by EMS, baseline ECG at R showing LBBB with first degree. Normal echo, Cath, MRI pending. Thoughts??

3
2
13
23 Aug 2022
I think other differential includes ARVC missed by echo, atriofascicular pathway, and moderator band VT
3
23 Aug 2022
Great thought, given incomplete LBBB in NSR definite possibility and many cases of BB reentry with normal EF described. I do think that the QRS morphology a bit unusual for BB reentry VT and expect more of an R-wave in V6, but EMS ECG
3
22 Apr 2022
Do we believe that we can see slow pathway conduction in NSR? Successful ablation of slow pathway at blue markers, His yellow, mapped with Grid
8
8
71
8 Aug 2021
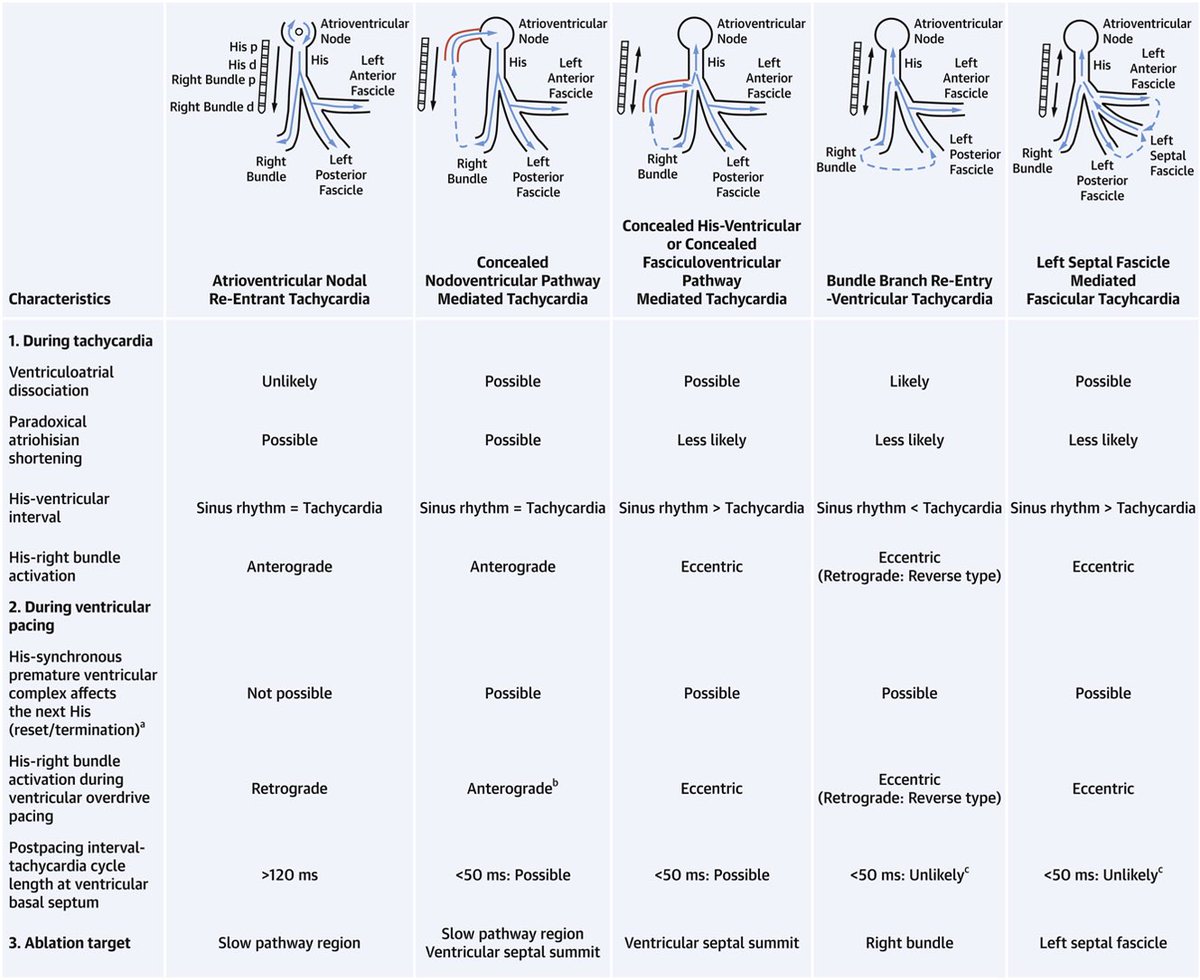
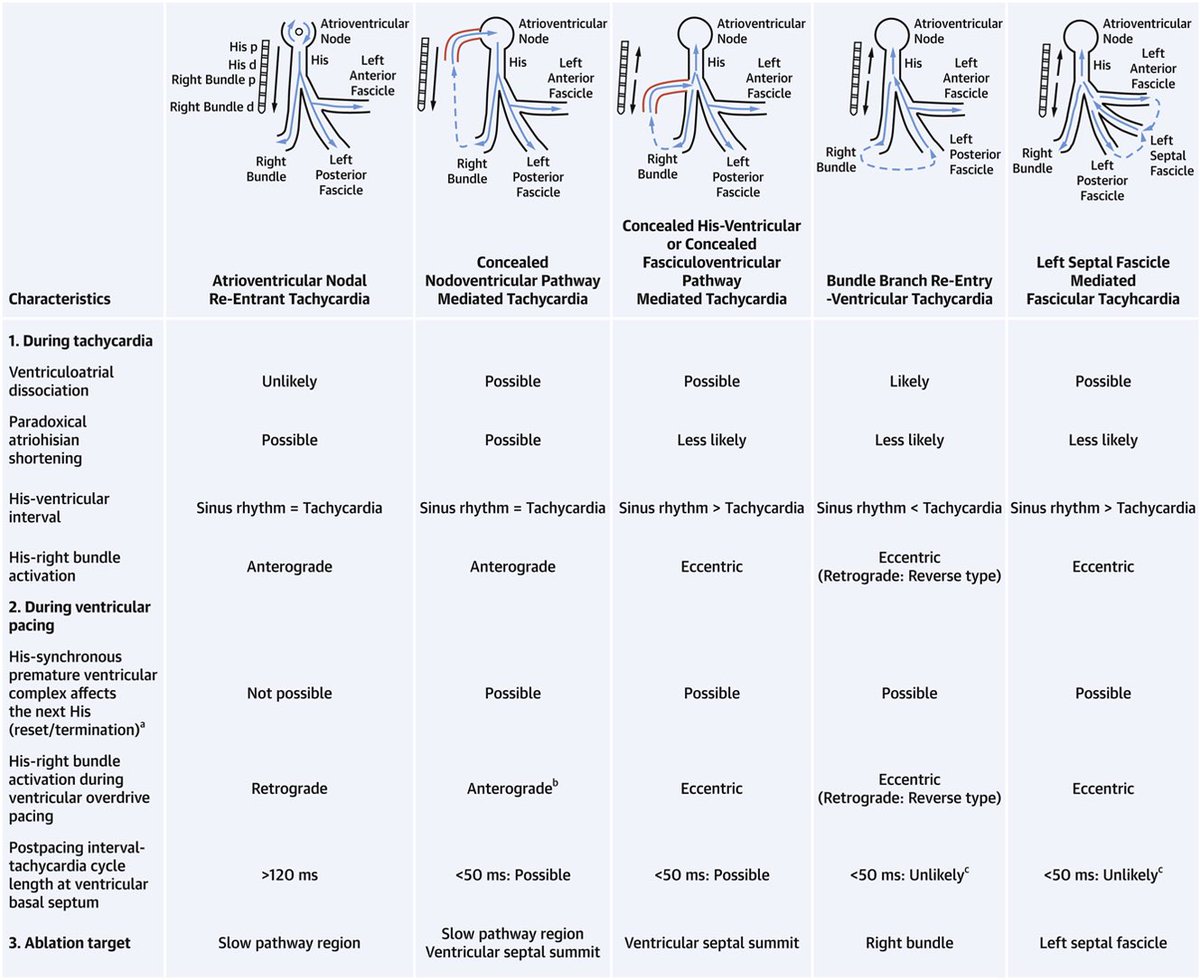
Can people help me? How do you know EXACTLY where to ablate concealed nodoventricular and fasciculoventricular pathways? VentricularSummit seems too broad.
3
1
8 Aug 2021
1
8 Aug 2021
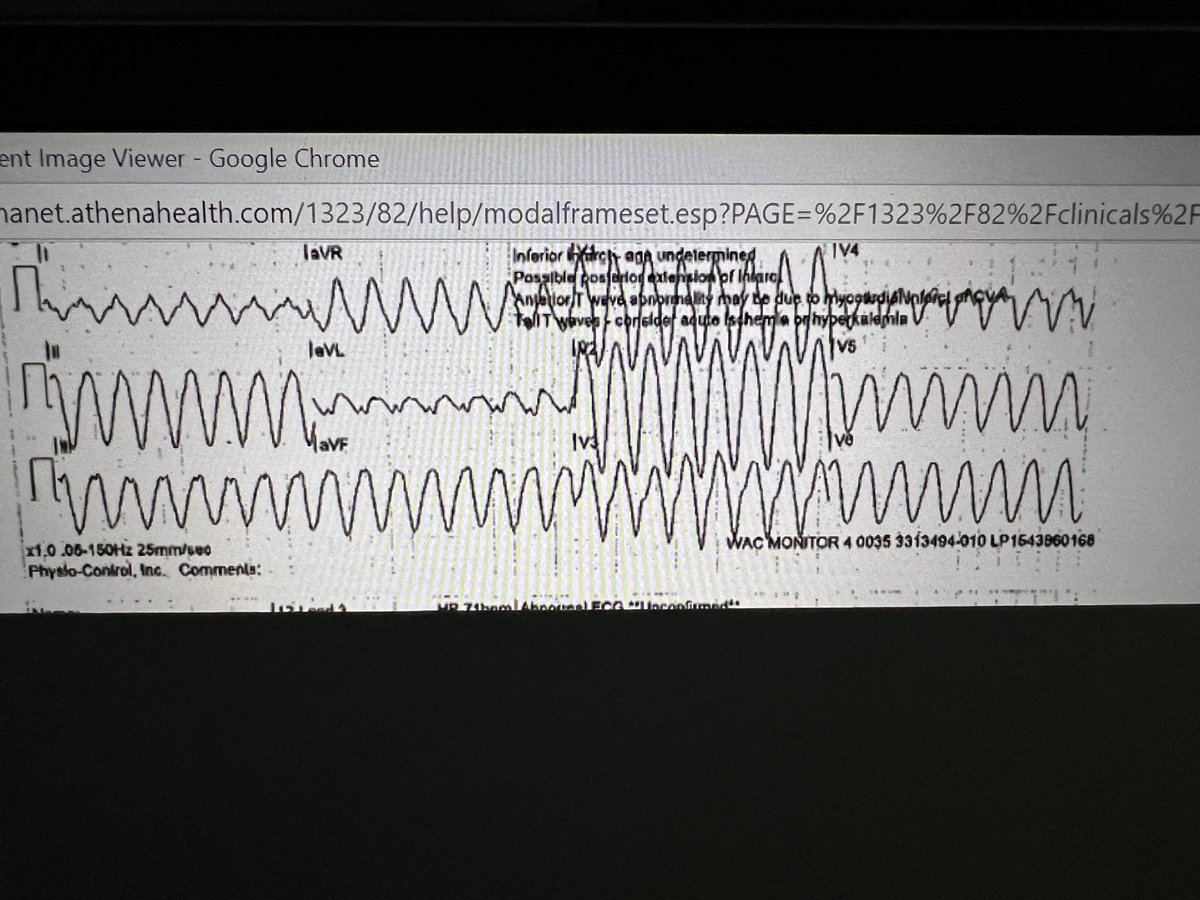
I know that in Bundle Branch Reentry clinically HV longer in tachycardia than NSR, but why? According to diagram it COULD theoretically be shorter if no delay in RBB during tachycardia?
2
1
7
8 Aug 2021
7 Jul 2021
I only seem to be able to find VOM (vein of Marshall) about 50% of time, any suggestions? I am doing occlusive balloon CS venogram with 10 cc full strength dye, possibly too Prox or distal or wrong techniques?@MiguelVldrbno @StevenZweibel
5
2
12
9 Feb 2021
Has anyone seen occlusion of vein of Marshall after ablation in CS? Had case where couldn’t find a hint of it after CS RFA. Or, was it just congenitally absent. Interested in thoughts.
@MiguelVldrbno @natale_md
2
4
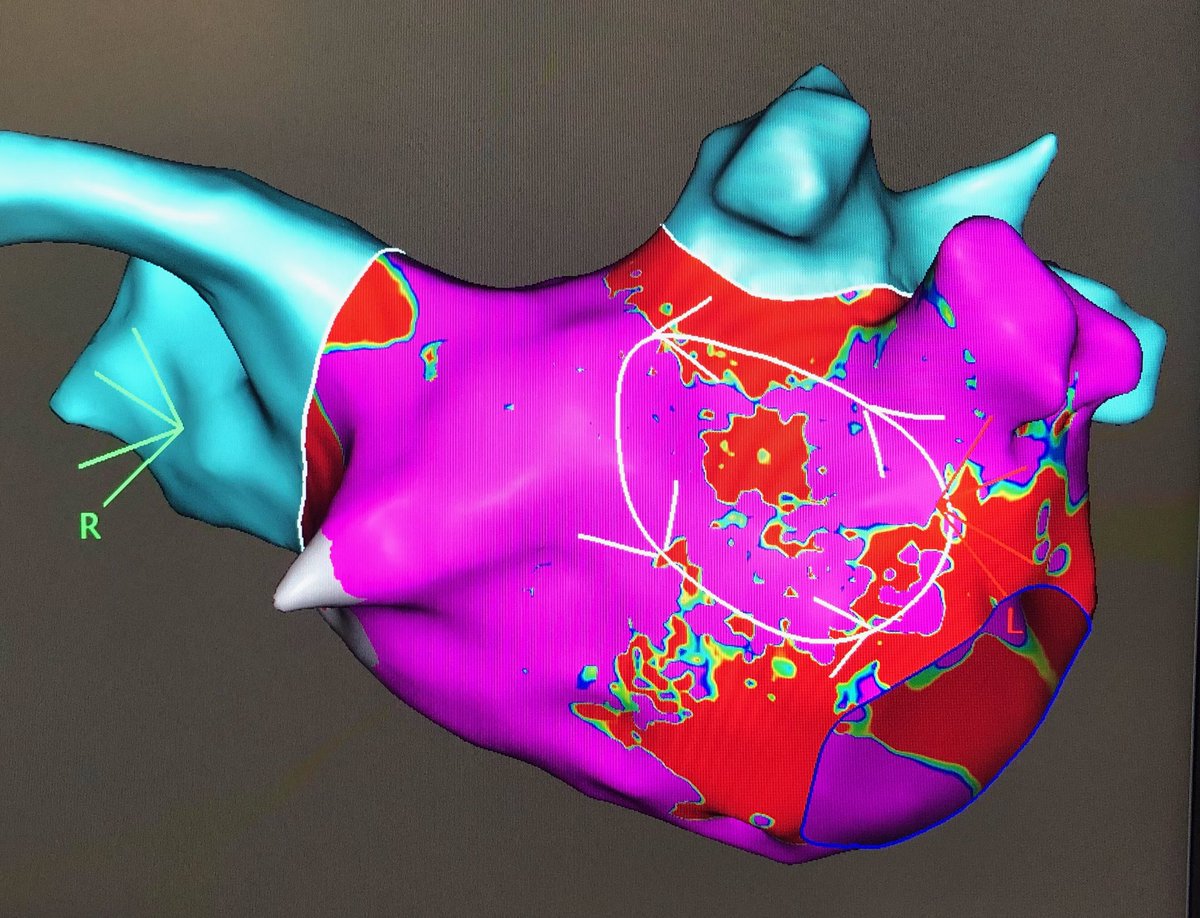
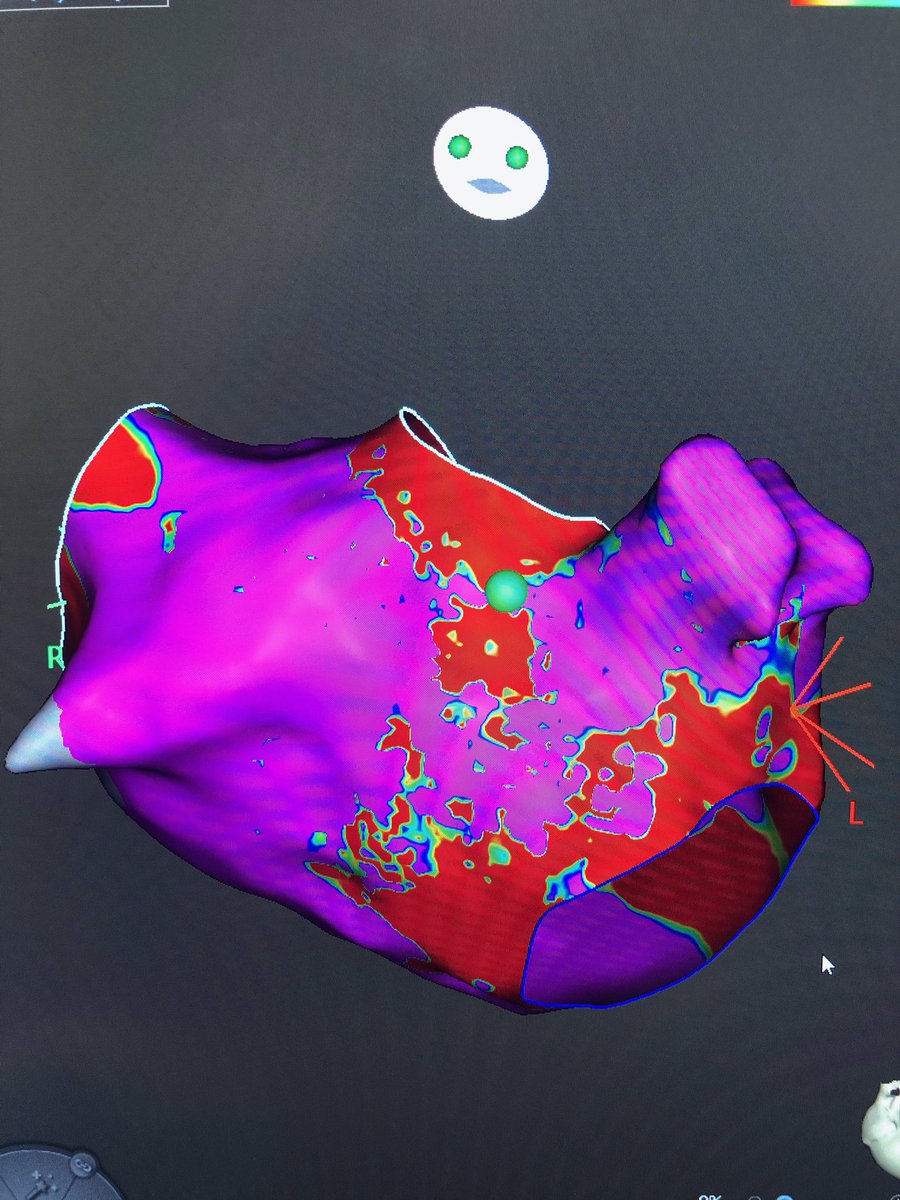
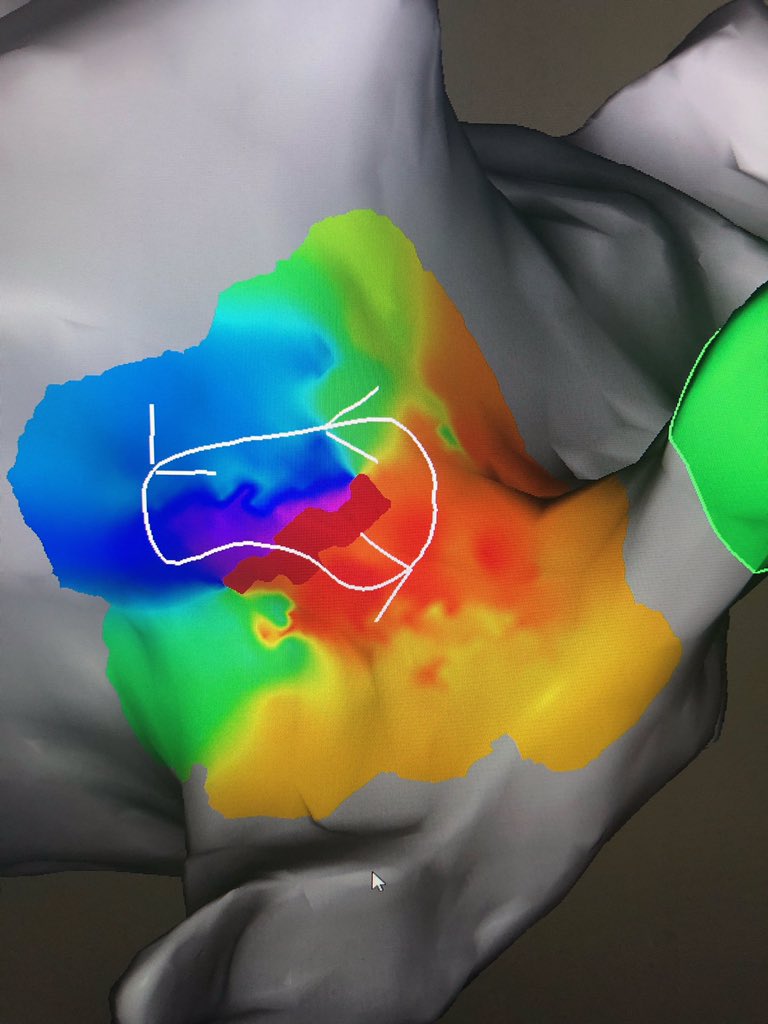
11 Nov 2020
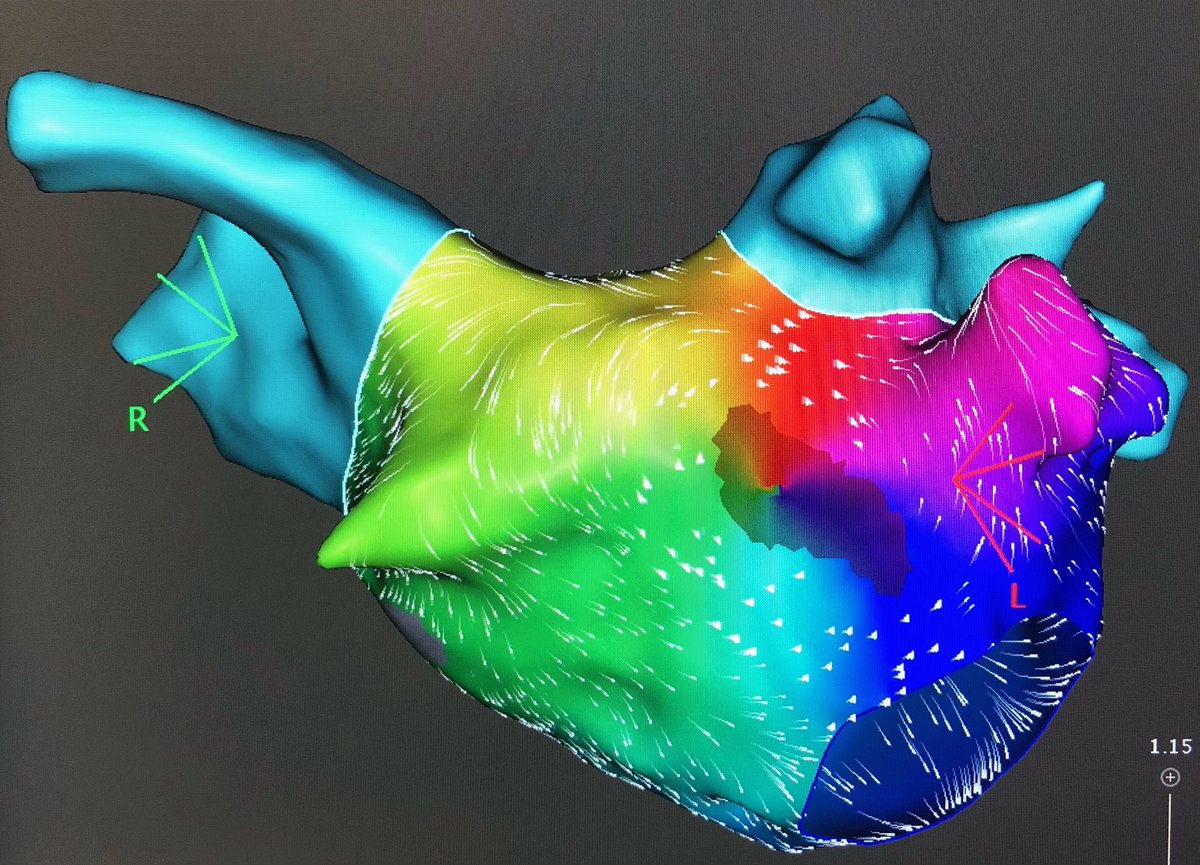
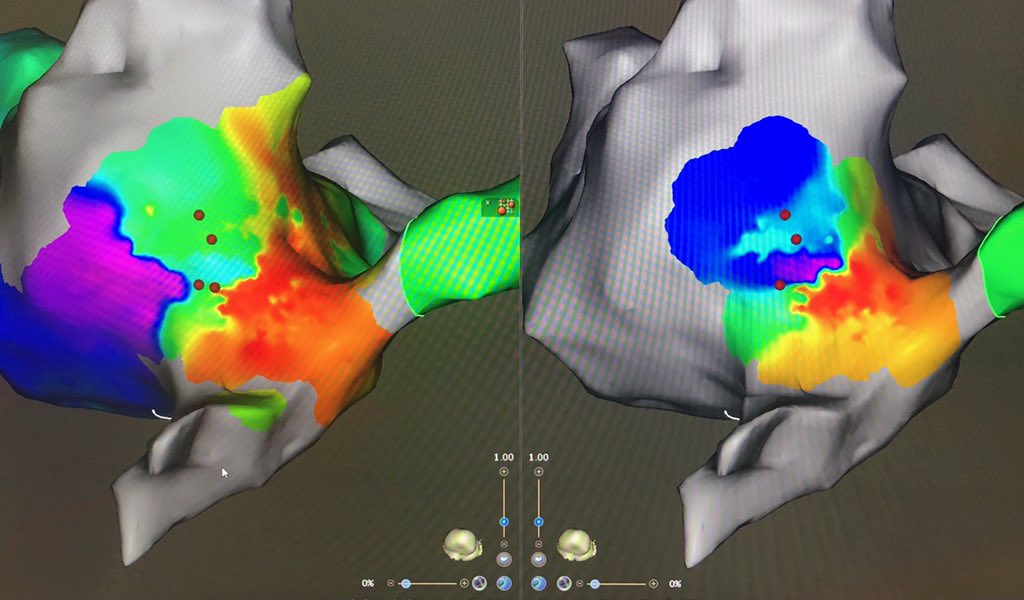
Very instructive for fellows. Prior CTI line, flutter looks focal, but fools you because late activation on other side of isthmus “hides” true circuit. Second and third maps after deleting passively activated points.
1
10
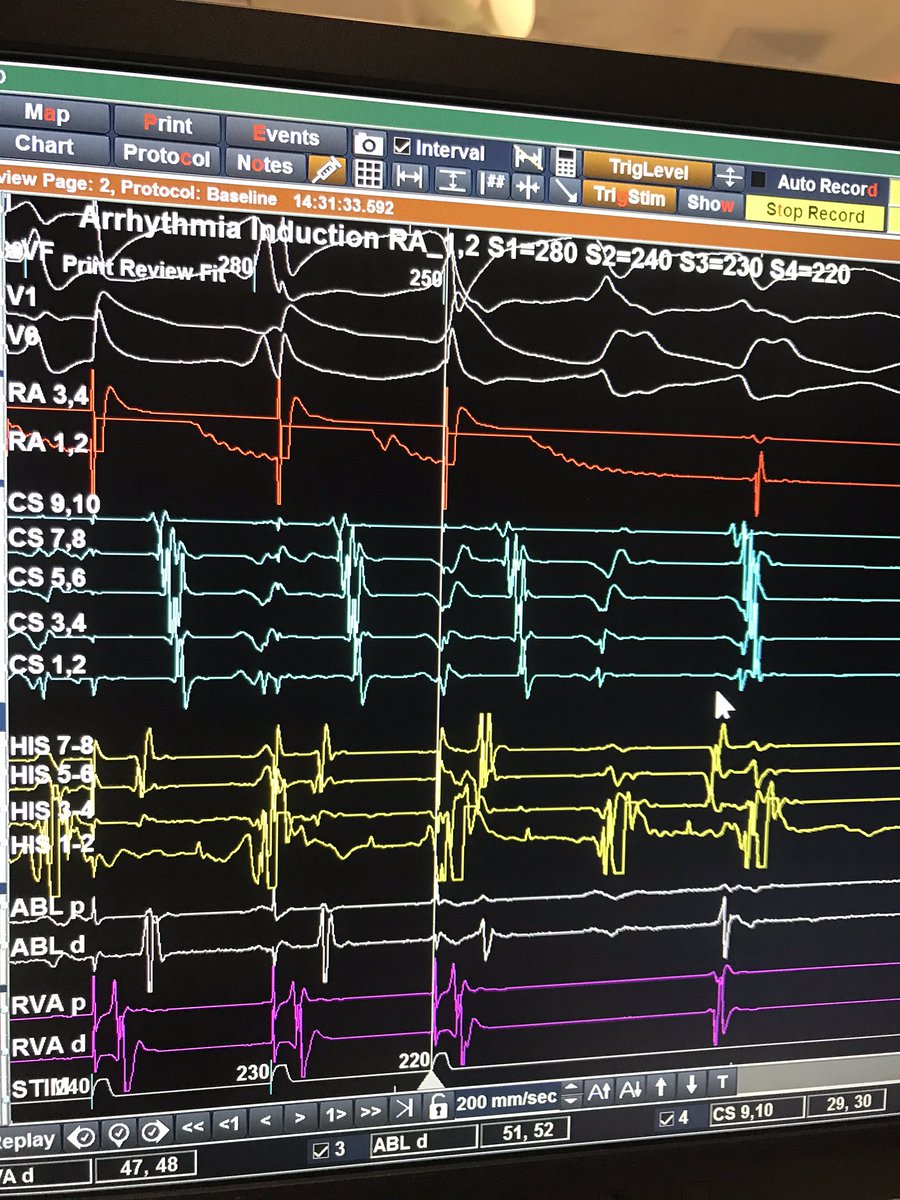
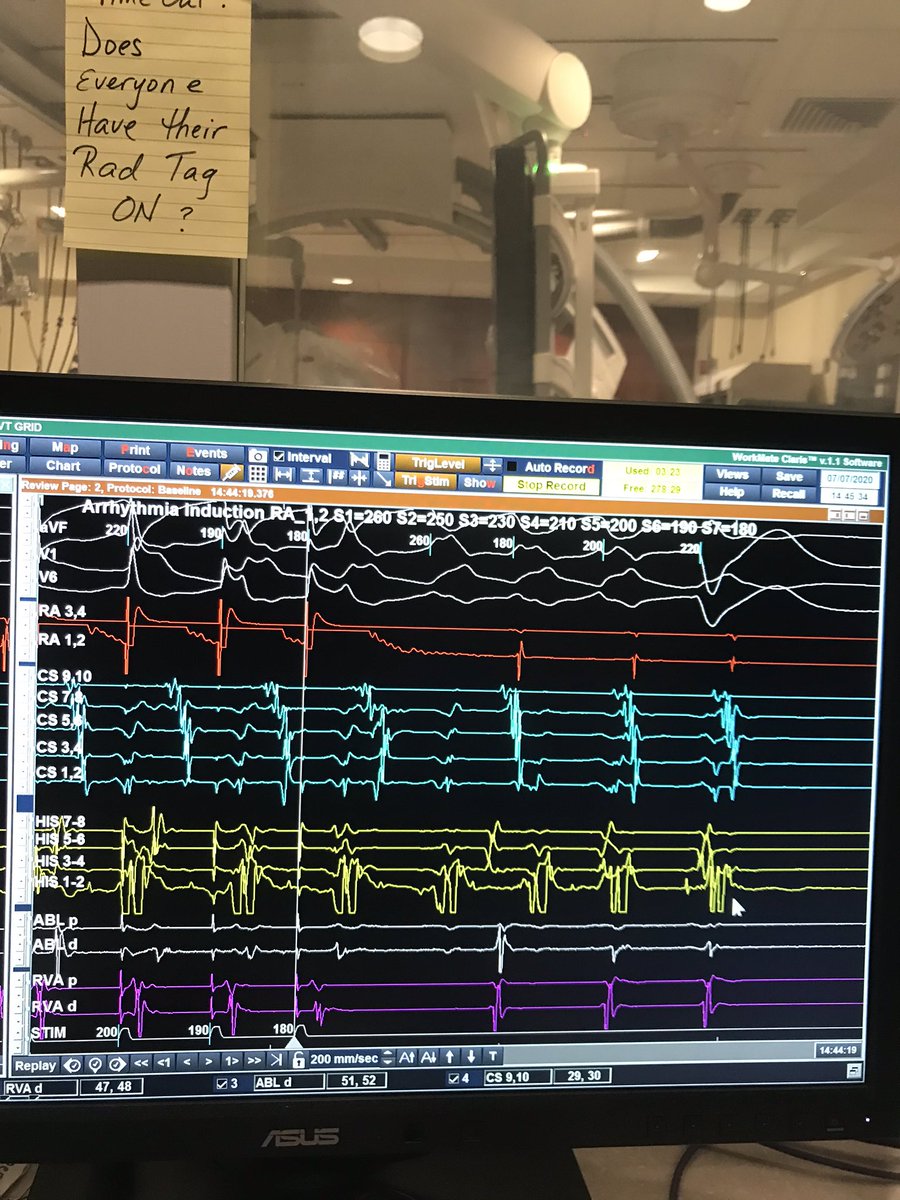
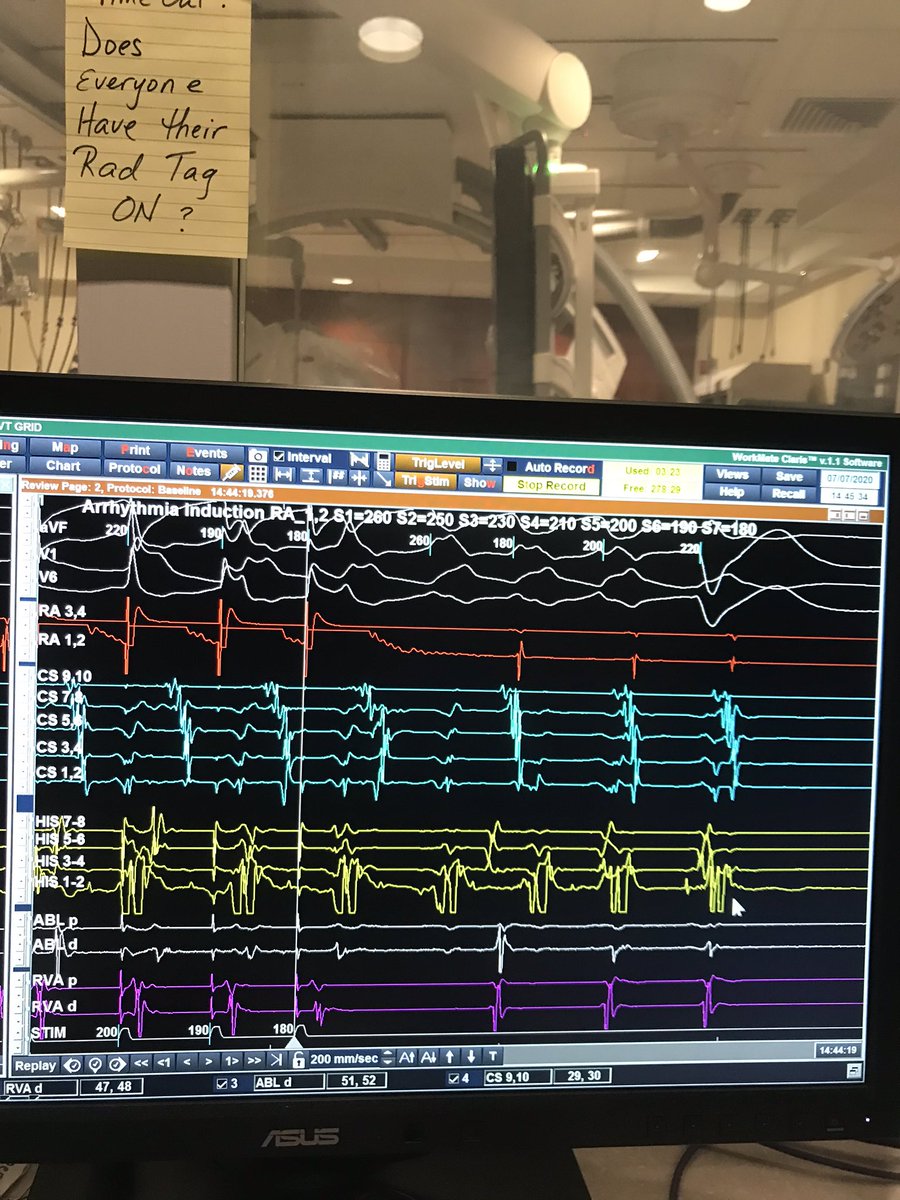
7 Jul 2020
The only way I can explain this is bundle branch reentry induces from the atrium in a young pt with incredibly enhanced AV nodal conduction, any other ideas?
1
1