
👨🏼🏫Assistant Research Professor 🔎Pain researcher studying acute ➡️ chronic pain in dept of emergency medicine 👨⚕️Doctor of Chiropractic
Joined December 2015
- Tweets 6,740
- Following 1,188
- Followers 2,287
- Likes 4,697
1,461 Photos and videos





Pinned Tweet

Mar 28
Pain catastrophizing may be shaped by more than pain intensity alone.
In exploratory analyses from our PREVENT cohort, a greater number of endorsed social need domains across the four domains we assessed was associated with higher PCS scores, even after accounting for current pain intensity. Each additional social need domain was associated with a 3.48-point higher PCS score (β=3.48, SE=1.65; p=0.042), whereas each 1-point increase in current pain was associated with a 2.51-point higher PCS score (β=2.51, SE=1.05; p=0.023).
This is an early finding from a small sample and should be viewed as hypothesis-generating. But it raises an important question: are the social needs we identify in acute pain care also shaping how patients interpret and cope with pain?
#PainResearch #HealthEquity #SocialDeterminantsOfHealth #EmergencyMedicine #PainScience
257
May 26
Over the past two years transitioning full-time into research and attending countless grant-writing conferences and workshops, I’ve found myself wondering how many phenomenal ideas simply die on the vine.
Like many entering academia, I initially believed that strong questions, rigorous methods, and meaningful potential impact would naturally rise to the top and get funded. But science conducted within human systems is rarely that straightforward.
Research funding is still shaped by people, institutions, incentives, timing, networks, communication, and perception. Even with safeguards against bias, we are still operating within systems we constructed ourselves. A well-researched hypothesis paired with a well-designed study does not guarantee extramural funding.
Ironically, some of my greatest assets as a researcher came from the decade I spent owning and operating a business. Learning how to market ideas, advocate relentlessly in unstable environments, build relationships, communicate value clearly, and keep moving despite rejection.
Maybe that’s the disconnect. Academics aren’t immune from the realities of persuasion and visibility. Our science often doesn’t stand on its own — at least not initially.
Maybe the old sales principle applies here too: Always Be Closing.
#research #academic #clinician
69

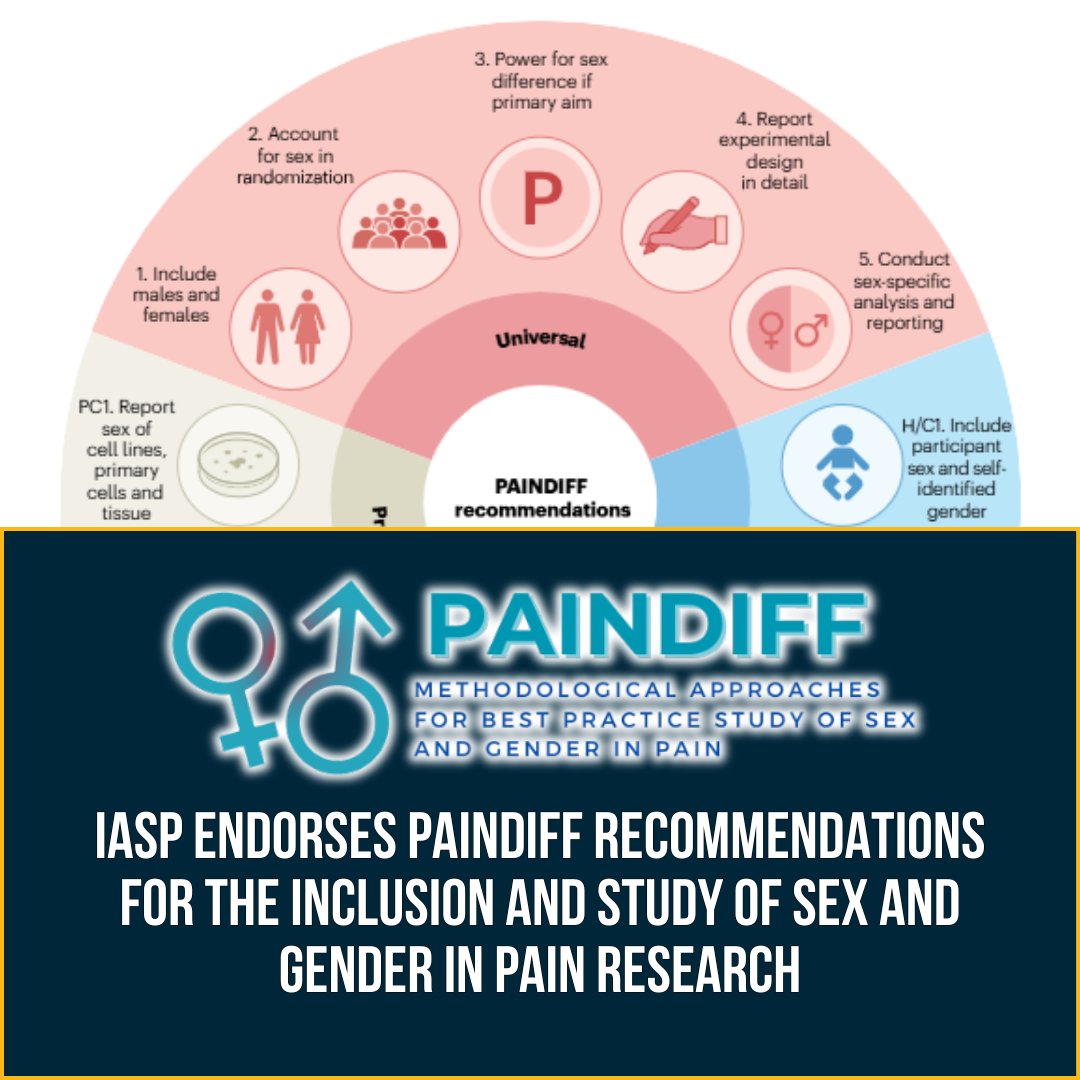
IASP endorses the PAINDIFF recommendations for the inclusion and study of sex and gender in pain research, supporting greater rigor, transparency, and reproducibility across preclinical and clinical pain research. Learn more: bit.ly/4dkFk0f
2
4
328
May 15
For me, the postdoctoral position at @GWSMHS through the Primary Care Research Training Program has been invaluable. Beyond the mentorship, resources, and connections, it gave me something equally important: time. Time to further establish myself as an investigator, gather preliminary data, and write grants.
Since July 2025, I have submitted $1.5 million in grant applications, submitted four manuscripts, had three accepted, and have two upcoming research presentations.
None of the grants have been awarded yet, but I’m optimistic that some will be soon.
Feeling grateful and hopeful. #research #grants #academic #clinician
2
160
May 12
I’ll be presenting first-year baseline cohort findings from PREVENT, our emergency department-based study focused on chronic pain prevention.
My presentation will focus specifically on social needs burden as an exposure and its relationship with pain-related cognitions, psychological symptoms, and functional outcomes among adults presenting to the ED with acute musculoskeletal pain.
The webinar is part of the @IASPpain Pain Education Resource Center session:
Advancing Research on the Social Dimensions of Pain: Emerging Evidence and Future Directions
May 20 | 7:00 AM
You can register here:
perc.iasp-pain.org/products/…
Please also check out the other speakers presenting on this important topic. Hope to see you there!
1
1
75

Strong framing. The prevalence/burden split is what makes this operationally useful: one tells you where to screen, the other where resources and follow-up capacity will be stressed. Without that second layer, care planning turns into a case-finding exercise.
1
1
113
May 6
I spent the past year examining the prevalence, burden, and correlates of chronic pain and high-impact (activity-limiting) chronic pain in the U.S.
The study—now in press at @TheJournal_Pain —uses nationally representative data from 2019–2023. Here’s what stood out:
🔹 Chronic pain is increasing
Prevalence rose from 20.5% to 24.3%, with high-impact pain increasing from 7.5% to 8.5%
🔹 Age shows the clearest pattern—but chronic pain spans the life course. Prevalence rises with age, but a substantial share of the population with chronic pain is under 65.
🔹 Socioeconomic disadvantage is consistently associated with chronic pain. Unemployment and poverty show strong, independent associations with both chronic pain and high-impact chronic pain.
🔹 Mental health and pain are closely linked. Frequent anxiety and depressive symptoms—and poor self-rated health—are strongly associated, especially for high-impact pain
🔹 High health care contact does not necessarily mean needs are met.
Greater health care utilization (ED visits, urgent care, home care) and cost-related barriers (delayed care, delayed prescriptions, medical bill strain) were independently associated with chronic pain.
---
A key insight from this work:
Prevalence and burden tell different but complementary stories.
- Prevalence helps identify who is most affected (e.g., case finding and screening)
- Burden shows where pain is concentrated across the population (informing resource allocation and care planning)
---
Takeaway:
Chronic pain—and especially high-impact chronic pain—is not just a clinical issue. It reflects a broader intersection of mental health, socioeconomic conditions, and health system factors, with substantial unmet need even among those already engaged in care.
Grateful to see this work coming to publication in and excited for what comes next.
📄 Pre-proof available at The Journal of Pain: jpain.org/article/S1526-5900…
@GWSMHS @GW_OVPR
1
84
Apr 22
Excited to share that I’ll be presenting preliminary results from the PREVENT study at the upcoming @IASPpain Social Aspects of Pain SIG webinar:
Advancing Research on the Social Dimensions of Pain: Emerging Evidence and Future Directions
Date: May 20
Presentation title: Social Vulnerability and Pain-Related Cognitions in Acute Musculoskeletal Pain: Implications for Early Intervention in the Emergency Department
Looking forward to contributing to this conversation.
Registration link below for anyone who’d like to attend:
perc.iasp-pain.org/products/…
@GWSMHS
#pain #research #academia #clinician #scientist
1
108
Apr 22
A key takeaway from my recent analysis of chronic pain and high-impact chronic pain in the U.S.:
“Pain-related need is concentrated not only among adults with high health care utilization and affordability barriers, but also within the broader population of adults with chronic pain who are already engaged with the health care system.”
Hoping the manuscript will be out soon.
#pain #research #epidemiology
1
1
87
Michael Ray retweeted

Please join us in congratulating the AIM-Back trial (PIs: Drs. Steve George & Nicki Hastings) on their recent results publication in @JAMANetworkOpen
Link here: tinyurl.com/mre27zxx
1
4
7
786
Apr 14
I’ve continued reviewing the 1-year baseline data from PREVENT to better characterize the emergency department cohort presenting with acute neck and low back pain (≤4 weeks) and to identify early patterns that can inform future study refinements.
Likely unsurprising to ED clinicians and staff, social needs burden is emerging as a meaningful signal associated with pain-related cognitions, psychological symptoms, and functional outcomes.
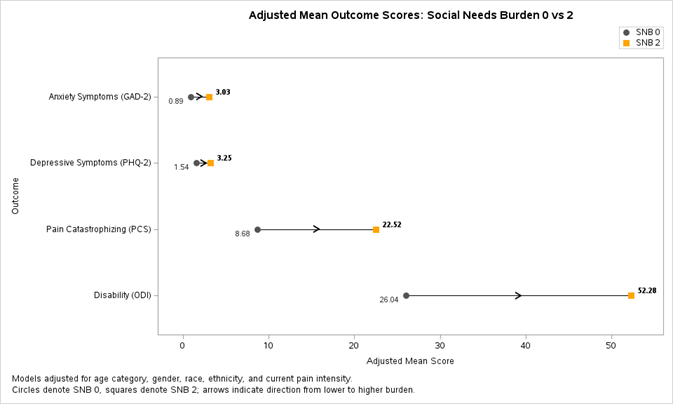
In recent linear trend analyses, increasing social needs burden from 0 to 2 was associated with higher scores on the Pain Catastrophizing Scale (PCS), PHQ-2, GAD-2, and the Oswestry Disability Index (ODI). These are still early signals, and I’m curious to see how additional baseline data collection shapes these patterns.
Practically, this may have important implications for how we think about screening and intervention in the ED. An initial screening process may need to include social needs burden alongside pain-related cognitions such as PCS. One possible pathway is for elevated social needs burden to trigger administration of PCS, with high, very high, or clinically elevated PCS scores then prompting a brief intervention.
For many patients in this cohort, the ED encounter may be one of the few opportunities to receive updated pain science education and practical self-management strategies. That makes the question less about whether these patterns matter, and more about how we can respond to them in a way that is brief, feasible, and useful in real-world care.
#EmergencyMedicine #PainResearch #HealthServicesResearch #SocialDeterminantsOfHealth #ChronicPain #MusculoskeletalPain #ImplementationScience
2
1
122
Michael Ray retweeted

Mar 23
Firima et al. assert that the elevated prevalence of chronic pain and high-impact chronic pain, associated with chronic conditions, supports the need for integrative chronic care involving pain management. Learn more in #PainReports bit.ly/4rup174

2
4
449
Michael Ray retweeted

⏳ It’s time for the 2026 USASP Annual Scientific Meeting!
Join leading scientists, clinicians & trainees advancing pain research and care.
📍 Philadelphia
📅 March 23–26, 2026
Learn more: usasp.org/2026annualmeeting
#usasp2026
1
3
172
Mar 19
Great study!

Original: Drs. Ruan, Yang, & Grol-Prokopczyk examined whether pain severity or pain interference is more strongly associated with all-cause mortality among U.S. adults aged 51 and older.
FULL: jpain.org/article/S1526-5900…
193
Mar 14
I’ve spent a lot of time working with National Health Interview Survey (NHIS) data over the years, most recently focused on social determinants of health and social needs vulnerabilities among people living with chronic pain and high-impact chronic pain.
As I’ve considered updates to my prospective observational study, PREVENT, I had initially planned to draw from recent NHIS items in this area. But after reading ISHOO, I’ll be looking to incorporate questions from Part B instead.
These days, when I think about how my research can best help in the pain space, I keep coming back to systems — and to the reality that we can only flourish as much as our systems allow. Paths long grooved by prior footwork are hard to change, and climbing out of those deep trenches is no easy task. Still, I’m hopeful.
Many thanks to all involved in finalizing these recommendations. A much-needed beacon of light in pain research. sciencedirect.com/science/ar…
#pain #society #culture #academic
#clinician #science
2
98
Mar 12
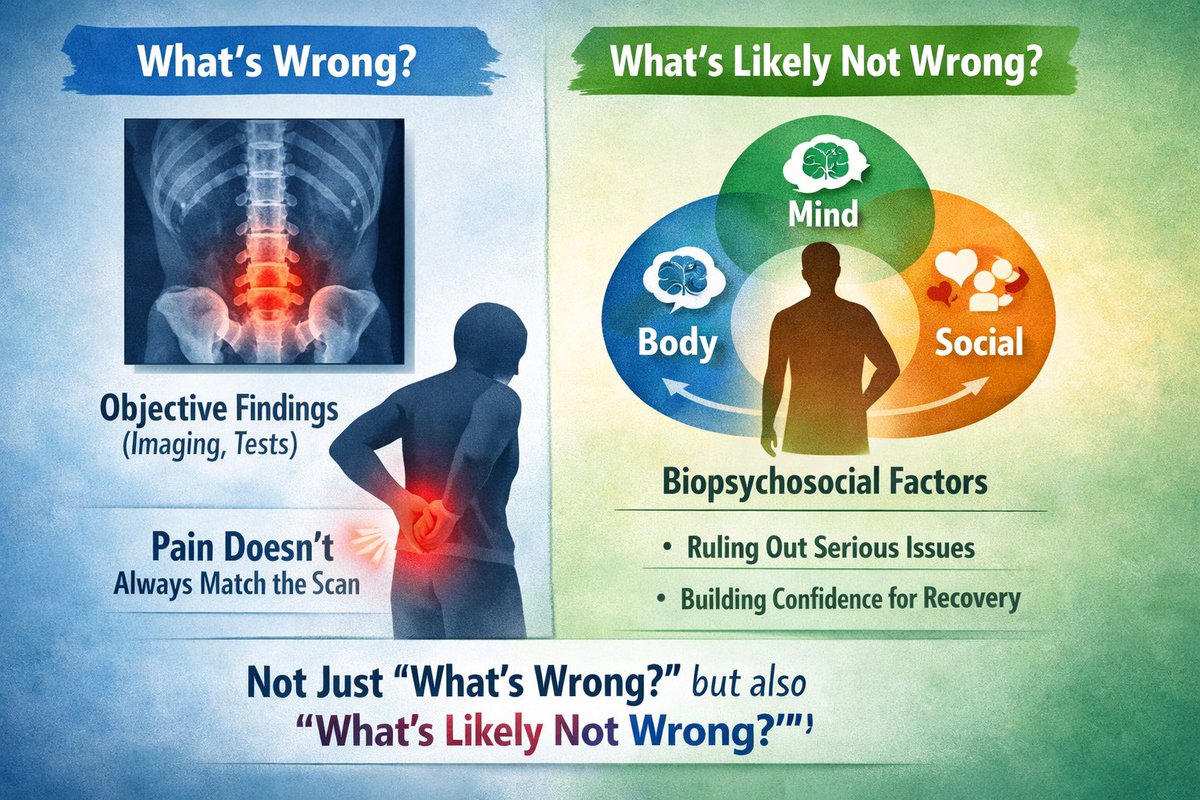
Through qualitative research and clinical practice, I often hear the belief that treating pain requires knowing exactly what is wrong in a body region. But pain is a subjective experience shaped by biopsychosocial factors, and objective findings like imaging do not always neatly explain symptoms. In many cases, a more helpful question is not only “What is wrong?” but also “What is likely not wrong?” That shift can build confidence, reduce fear, and help guide recovery. #pain #journey #recovery
66
Mar 12
Resubmitting my NIH K23 application this week — and feeling grateful for the many people who make clinical research possible.
A sincere thank you to the patients who participate in our studies, our research assistants and coordinators, collaborators and colleagues, my mentorship team, and the reviewers whose feedback helped strengthen this resubmission. Clinical research truly takes a team.
Our PREVENT study has now been ongoing for one year. PREVENT is a prospective observational study of patients presenting to the emergency department with acute (≤4 weeks) neck or low back pain. Over the past year, I’ve learned a great deal about conducting prospective observational research in the emergency care setting.
Importantly, this first year has given us the opportunity to analyze preliminary data, identify barriers to recruitment and follow-up, and revise study procedures to strengthen the next phase of the work. I’m optimistic about what we may learn in year two.
These preliminary data also informed my K23 resubmission, which is focused on building the training and knowledge needed to support development of a screening trigger for Pain-SBIRT (Pain Screening, Brief Intervention, and Referral to Treatment), followed by feasibility and usability work to prepare for a future R21.
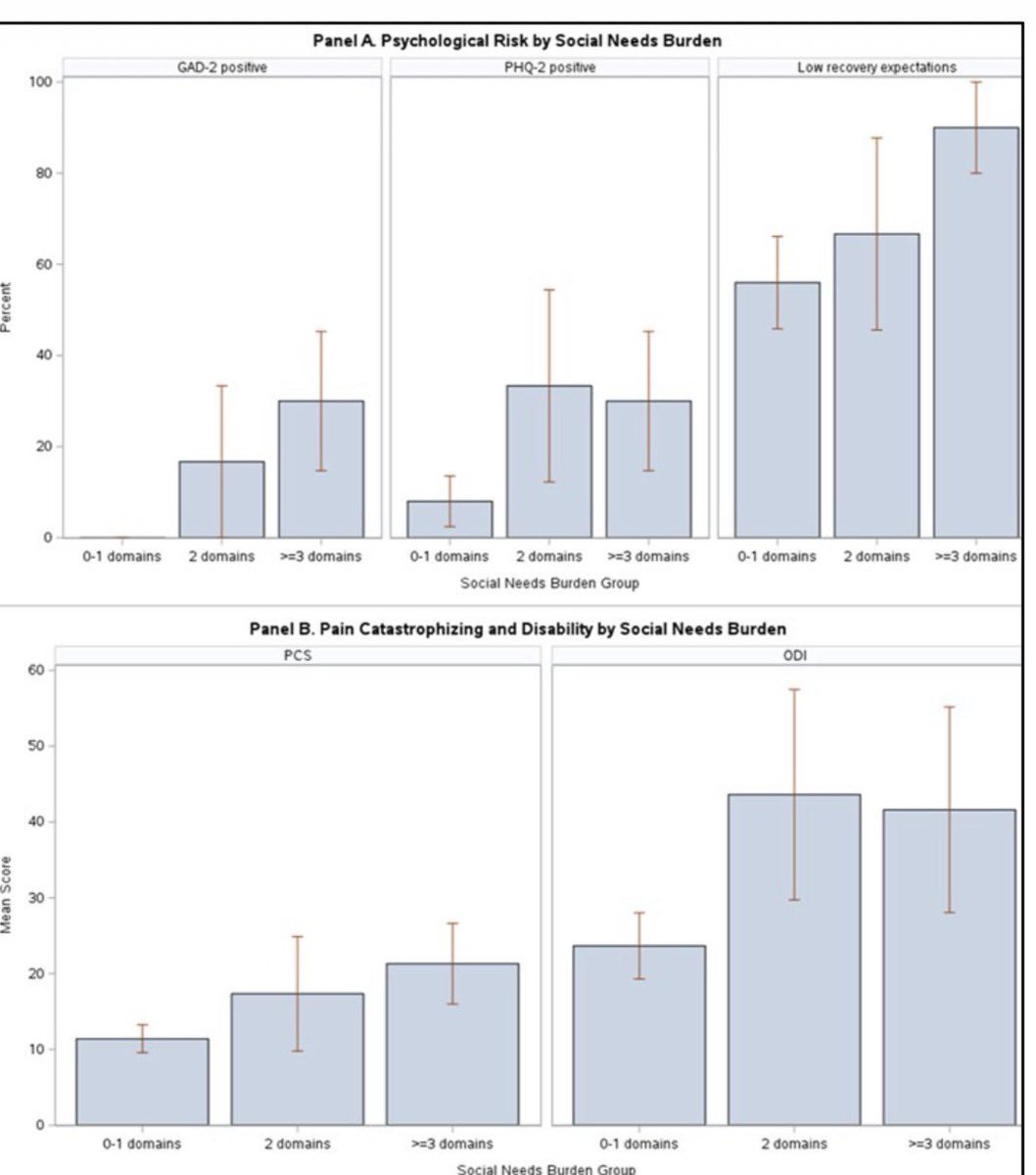
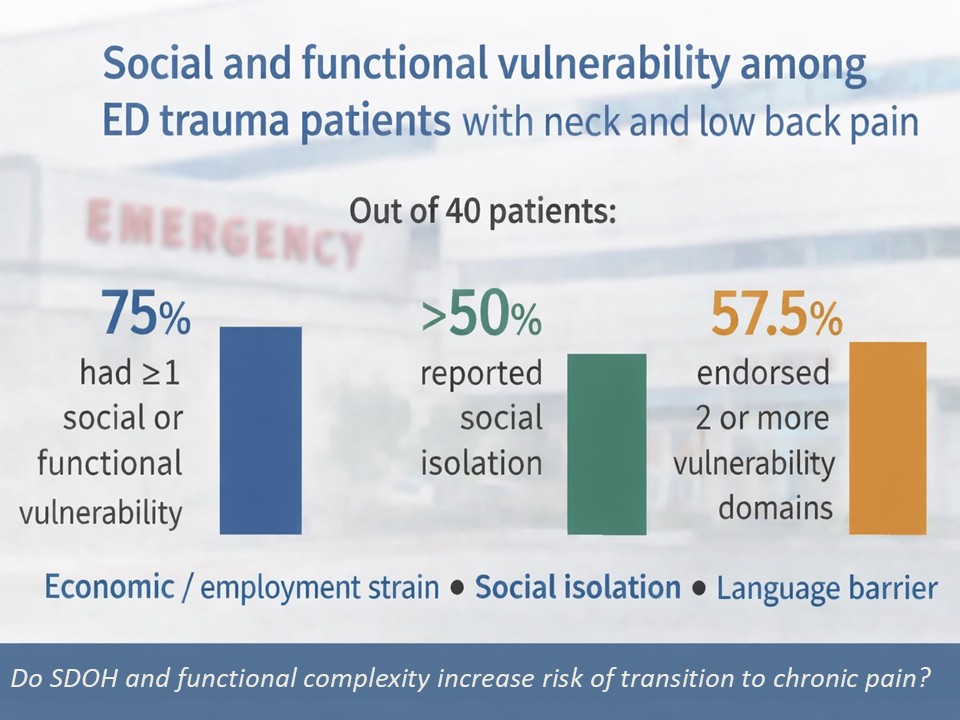
Among the first 42 PREVENT participants:
▪️ 16.7% screened positive for depressive symptoms on the PHQ-2
▪️ 9.5% screened positive for anxiety symptoms on the GAD-2
▪️ 39.2% reported at least some difficulty paying for basic needs
▪️ 31.7% reported at least sometimes feeling socially isolated
▪️ 17.1% reported needing assistance with employment or job training
Pain-related psychological factors were also present:
▪️ 11.9% demonstrated clinically elevated pain catastrophizing
▪️ 55% of participants with available data showed moderate or high fear of movement
▪️ 33.3% scored below the clinically meaningful threshold for pain self-efficacy
The figure below offers an early signal: pain catastrophizing, disability, and other markers of psychological risk appear to worsen as social needs burden increases.
These analyses are descriptive and based on a small sample, but they suggest that social vulnerability and maladaptive pain-related beliefs may cluster together among ED patients presenting with acute musculoskeletal pain.
If these patterns continue as PREVENT grows, they may help us identify patients earlier who could benefit from a targeted behavioral intervention.
This work is helping inform the development of Pain-SBIRT — an ED-deliverable behavioral intervention that we hope to refine, test for feasibility and usability, and ultimately evaluate in future studies.
More to come as PREVENT continues.
#ClinicalResearch #PainScience #EmergencyMedicine
#NIH
1
96