
123→66 kg | Not your weight loss motivator | Science is greater than slogans | Super chimera, heterobivalent & logic-gated ligands | Yes, Dr DiMarchi replied
Joined April 2025
- Tweets 827
- Following 44
- Followers 618
- Likes 60
529 Photos and videos





Jun 14
Over time on Mounjaro, the body seems to adapt.
The early stomach heaviness, burps and extreme appetite suppression reduce. Hunger comes back, not to the pre-Mounjaro level, but enough to notice.
In my case, maybe 20% of the hunger control & satiety effect has faded.
2
5
409
Jun 10
First time in 14 months of Mounjaro that I’ve had a small injection site lump.
Same routine. Same pen. New little surprise.
Nothing dramatic, but a useful reminder. Rotate sites, inject patiently & slowly and don’t assume every dose behaves exactly the same.
1
2
226
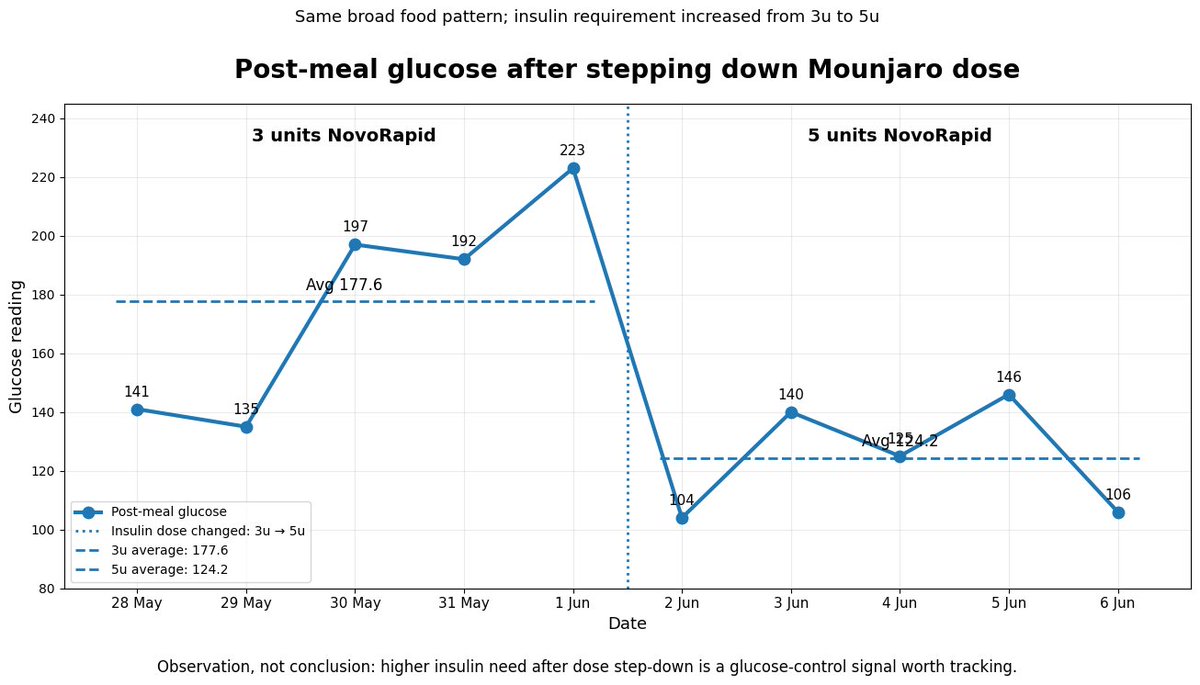
This feels like glucose control signal and @EliLillyandCo should study this mechanistically.
10 mg needed X insulin.
Moved to 12.5 mg hoping for insulin independence. Didn’t happen.
Moved back to 10 mg.
Now insulin requirement is higher than it was earlier on 10 mg.
No major change in food, exercise, sleep or weight.

Since stepping down from 12.5 mg to 10 mg Mounjaro, my post meal glucose has changed. Same broad food pattern, but higher readings and almost double the insulin needed. Too early to call it permanent, but this is a glucose control signal I need to watch.
1
206
Since stepping down from 12.5 mg to 10 mg Mounjaro, my post meal glucose has changed. Same broad food pattern, but higher readings and almost double the insulin needed. Too early to call it permanent, but this is a glucose control signal I need to watch.
1
402
Modern GLP1 drugs have a wild origin story.
One early breakthrough came from Gila monster saliva, which contained a GLP1 like compound that lasted longer in the body.
From desert lizard spit to Ozempic/Mounjaro. Nature is a terrifying pharmacist.
youtube.com/shorts/LbnUKFb9B…
1
218
Loose skin after major weight loss is real. You can improve it with time, strength training, protein, hydration, collagen support, and patience. The last option is of course, surgery. Just remember, no magic cream will shrink 30 kgs history.
1
1
5
405
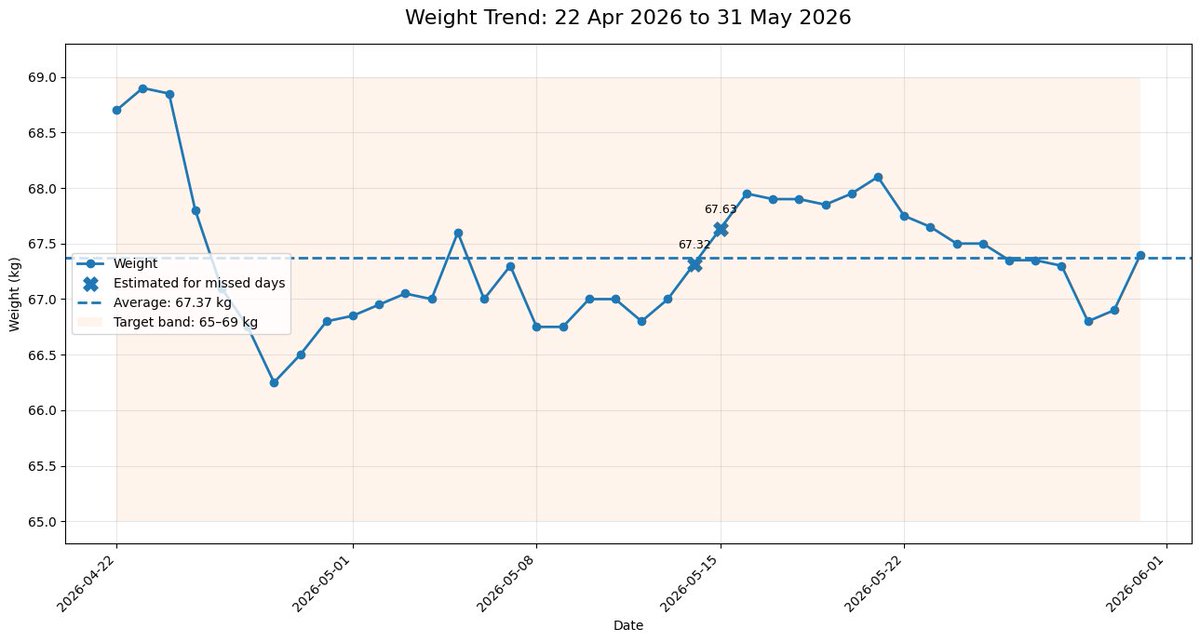
May 31
Once you reach your ideal weight band, the body seems to behave differently. My target was 65–69 kg. For weeks now, despite dose experiments, food changes and daily noise, I keep hovering in the same range. Maybe this is the body finally accepting a new set point.
This is it!
1
1
1
205
May 29
Retatrutide data is getting absurd.
12 mg dose in Phase 3 obesity trial:
• 28.3% mean weight loss at 80 weeks
• 45.3% achieved ≥30% weight loss
• Extension showed 30.3% loss at 104 weeks
• Improvements in waist, lipids, BP and hsCRP
This is not “weight loss drug” territory anymore.
This is pharmacological bariatric surgery territory.
1
3
260
May 28
Cannabis linked to lower weight and diabetes risk in mice.
Mice are now skinny, metabolically flexible, and presumably listening to Pink Floyd in a lab corner.
Humans, please wait before declaring “joint-based endocrinology” the next GLP1
sciencealert.com/cannabis-li…
1
1
122
May 27
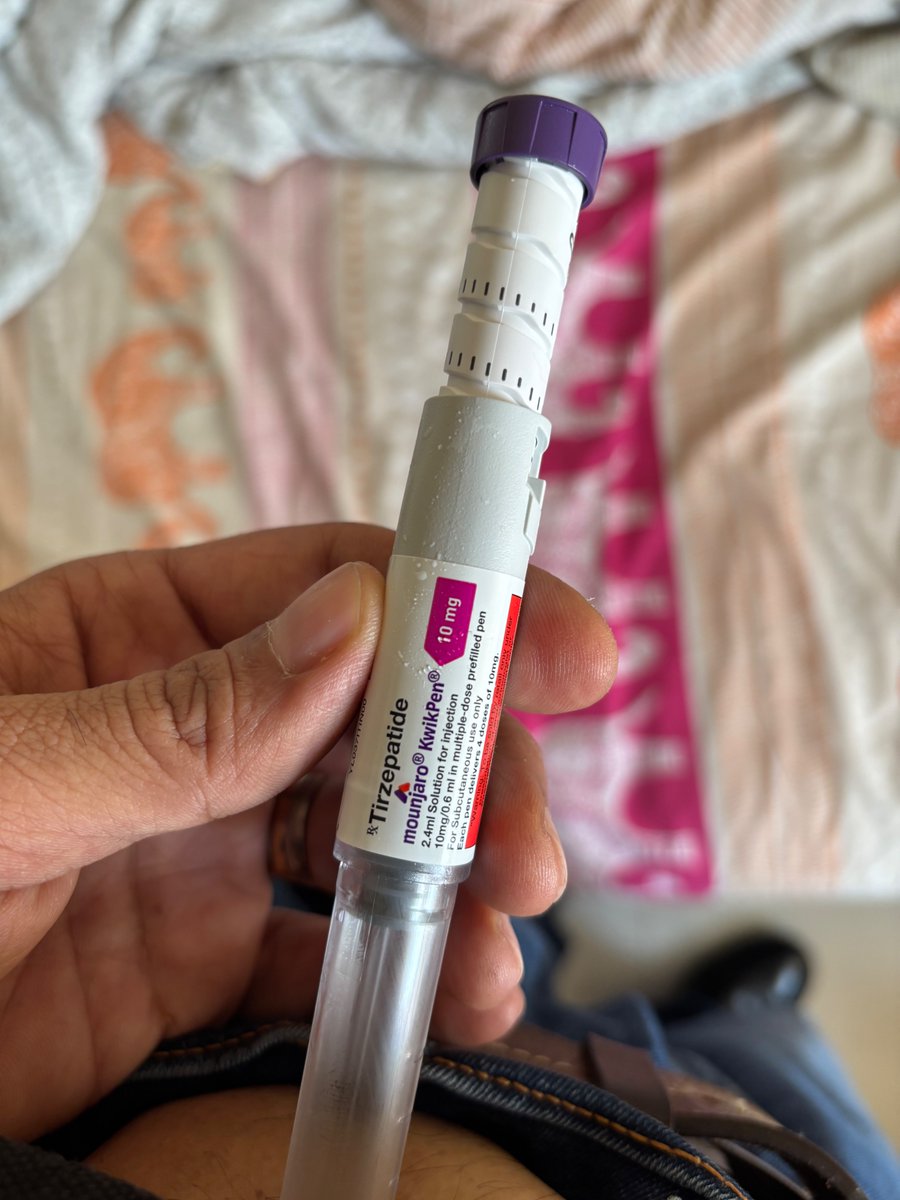
After 5 doses of 12.5 mg tirzepatide, golden dose included, I’m moving back to 10 mg.
Reason - No clear incremental benefit, especially on insulin independence.
Higher dose is not necessarily progress. Figured out 10 mg is my right dose.
1
1
3
270
May 26
AI scanned 400k Reddit posts on GLP1 drugs and finds hidden side effects.
GI issues showed up, but so did fatigue, chills, feeling cold, hot flashes and menstrual changes.
Not proof of causation.
But Reddit may be an early warning radar for side effects trials under capture.
sciencedaily.com/releases/20…
1
1
2
273
May 25
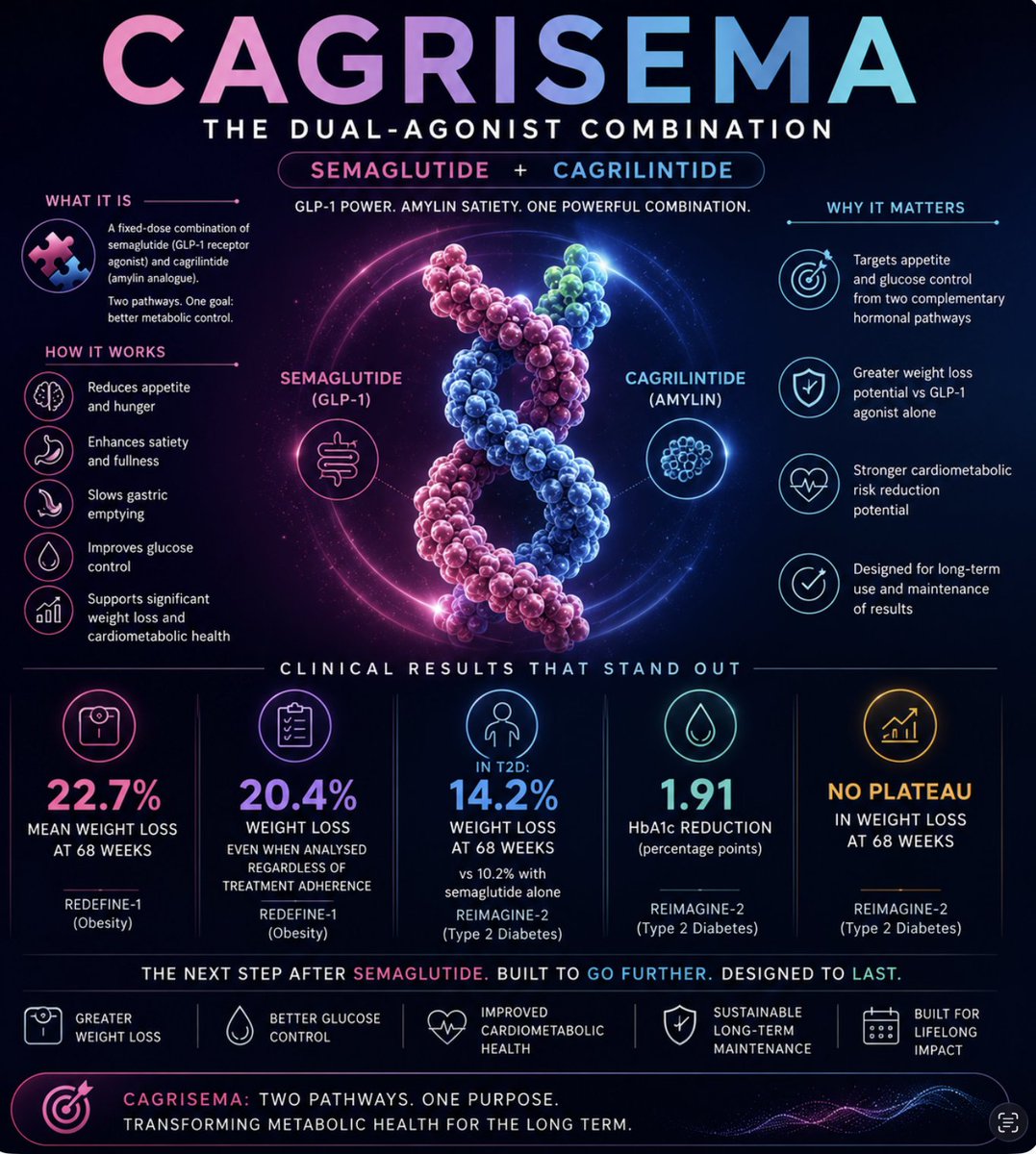
CagriSema is not “just a stronger Wegovy.”
It is a fixed-dose combination:
Semaglutide cagrilintide.
Translation: GLP-1’s glucose and appetite biology, paired with amylin’s satiety signal, one molecule controlling metabolic drive from two angles.
Clinical data so far has been solid:
• 22.7% mean weight loss at 68 weeks in REDEFINE-1 obesity data
• 20.4% weight loss even when analysed regardless of treatment adherence
• In T2D, 14.2% weight loss at 68 weeks versus 10.2% with semaglutide alone
• HbA1c reduction of 1.91 percentage points in T2D data
• No weight-loss plateau seen at 68 weeks in the T2D readout
This is why CagriSema matters.
Not because it is the flashiest peptide in the race.
Because it may become the practical next step after semaglutide: same GLP1 foundation, but with amylin added to deepen satiety, improve weight loss, and attack cardiometabolic risk harder.
It is not winning over death.
But it may be Novo’s most serious attempt to turn metabolic control into a long-term maintenance platform.
1
1
190
May 24
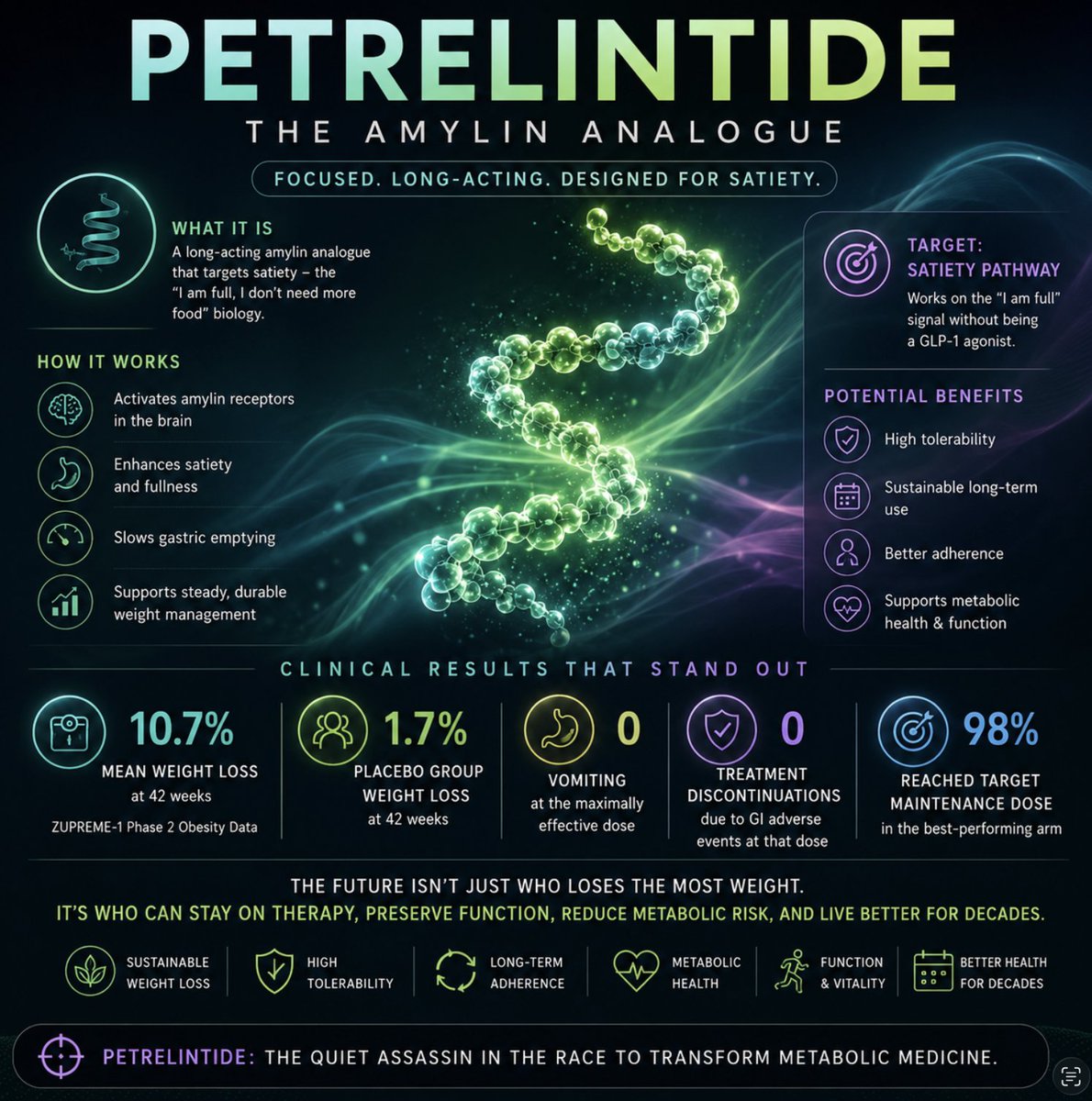
Petrelintide is not trying to be the loudest weight-loss drug in the room.
It is a long-acting amylin analogue.
Translation: it works on satiety, the “I am full, I don’t need more food” biology, without directly being another GLP-1 hammer.
Clinical data so far is interesting for a different reason:
• Up to 10.7% mean weight loss at 42 weeks
• Placebo group lost 1.7%
• No vomiting at the maximally effective dose
• No treatment discontinuations due to GI adverse events at that dose
• 98% reached the target maintenance dose in the best-performing arm
This is why petrelintide matters.
Not because it beats retatrutide on raw weight loss.
Because it may solve one of the biggest problems in metabolic medicine: tolerability.
The future is not just “who loses the most weight.”
It is who can stay on therapy, preserve function, reduce metabolic risk, and live better for decades.
Petrelintide may be the quiet assassin in that race.
1
2
190
May 20
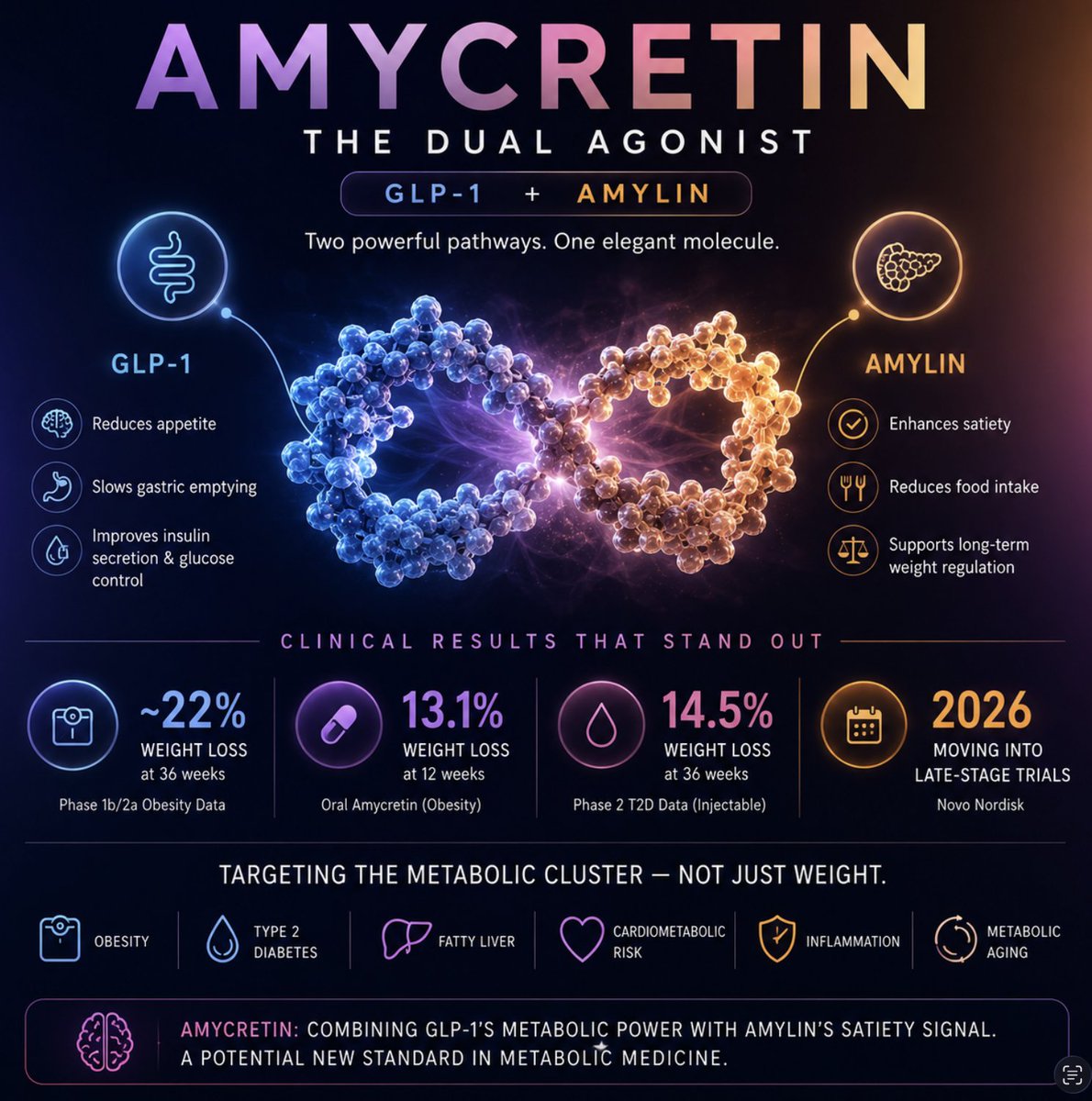
Amycretin is not “just another GLP1.”
It is a dual agonist:
GLP-1 amylin.
Translation: it targets appetite, satiety, gastric emptying, glucose control, and the “I am full, stop eating” signal — all in one molecule.
Clinical data so far has been seriously impressive:
• Up to ~22% weight loss at 36 weeks in Phase 1b/2a obesity data
• Oral amycretin showed up to 13.1% weight loss at 12 weeks
• In Phase 2 T2D data, injectable amycretin showed up to 14.5% weight loss at 36 weeks
• Novo is moving amycretin into late-stage trials in 2026
This is why amycretin may be one of the most elegant next-generation metabolic peptides.
Not because it only helps people lose weight.
Because it combines GLP-1’s metabolic control with amylin’s satiety biology — potentially attacking overeating, glucose dysregulation, obesity, and long-term cardiometabolic risk from two complementary angles.
It is not winning over death.
But it may help close one of death’s favourite gateways: chronic metabolic dysfunction.
1
175
May 18
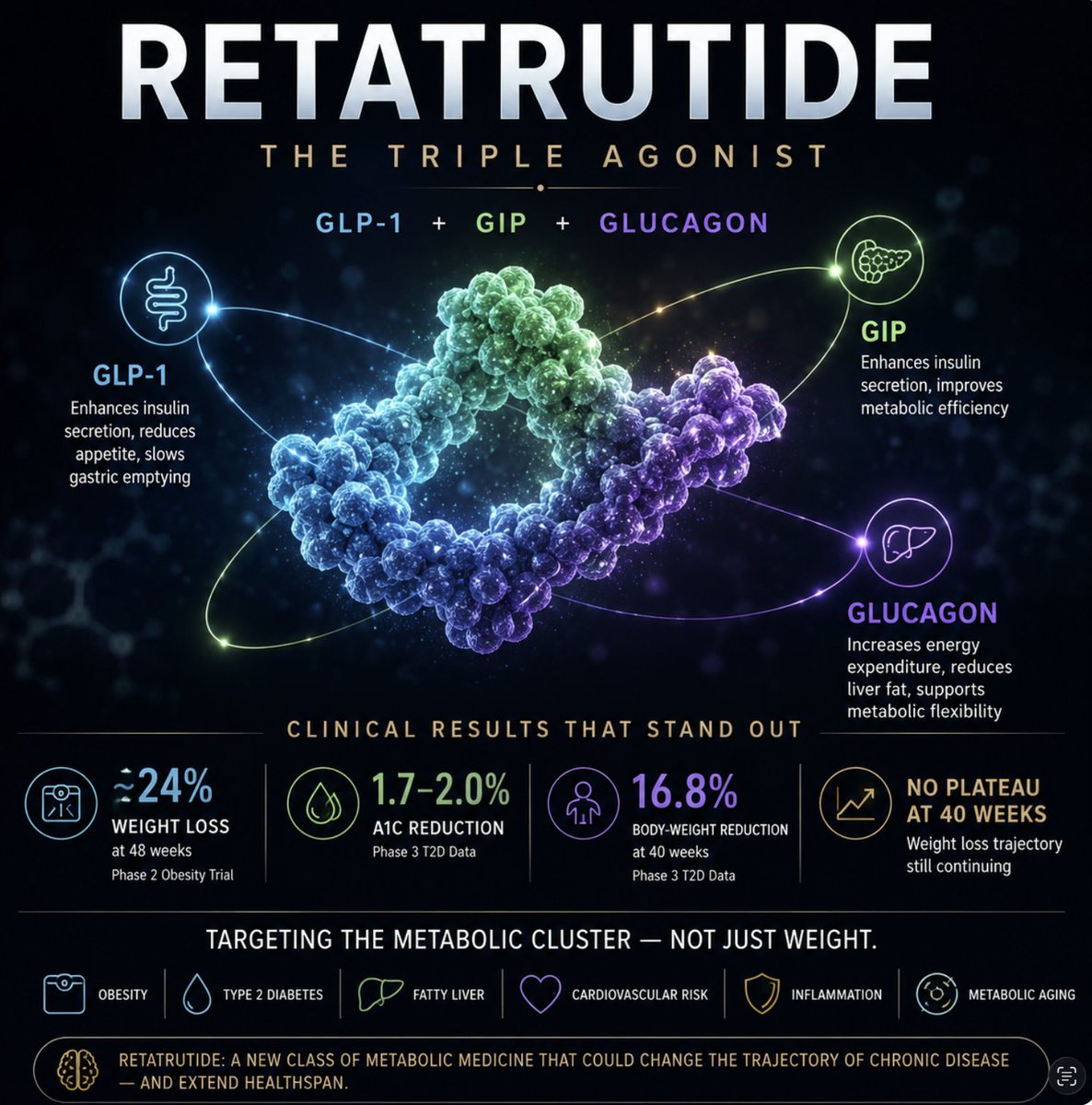
Retatrutide is not “just another GLP1.”
It is a triple agonist:
GLP-1 GIP glucagon.
Translation: it targets appetite, insulin biology, energy expenditure, weight, glucose control, liver fat and broader metabolic risk, all in one molecule.
Clinical data so far has been ridiculous:
Up to 24% weight loss at 48 weeks in Phase 2 obesity data
A1C reduction of 1.7–2.0% in Phase 3 T2D data
16.8% body-weight reduction at 40 weeks in T2D patients
Weight loss still had not plateaued in the 40-week Phase 3 readout
This is why retatrutide may be the first true “next era” metabolic peptide.
Not because it helps people lose weight.
Because it attacks the cluster: obesity, diabetes, fatty liver, cardiovascular risk, inflammation, and the slow metabolic decay we politely call “ageing.”
It is not winning over death.
But it may be one of the closest things pharma has built to delaying its favourite entry points.
1
3
4
1,032
May 17
The next metabolic wellness is not just GLP1
The 4 peptides I’m watching closely, purely on scientific merit:
1. Retatrutide
2. Amycretin
3. Petrelintide
4. CagriSema
Each attacks the problem differently: appetite, satiety, glucose control, liver fat, tolerability, and long-term maintenance.
This is where things get interesting.
1
3
275
May 15
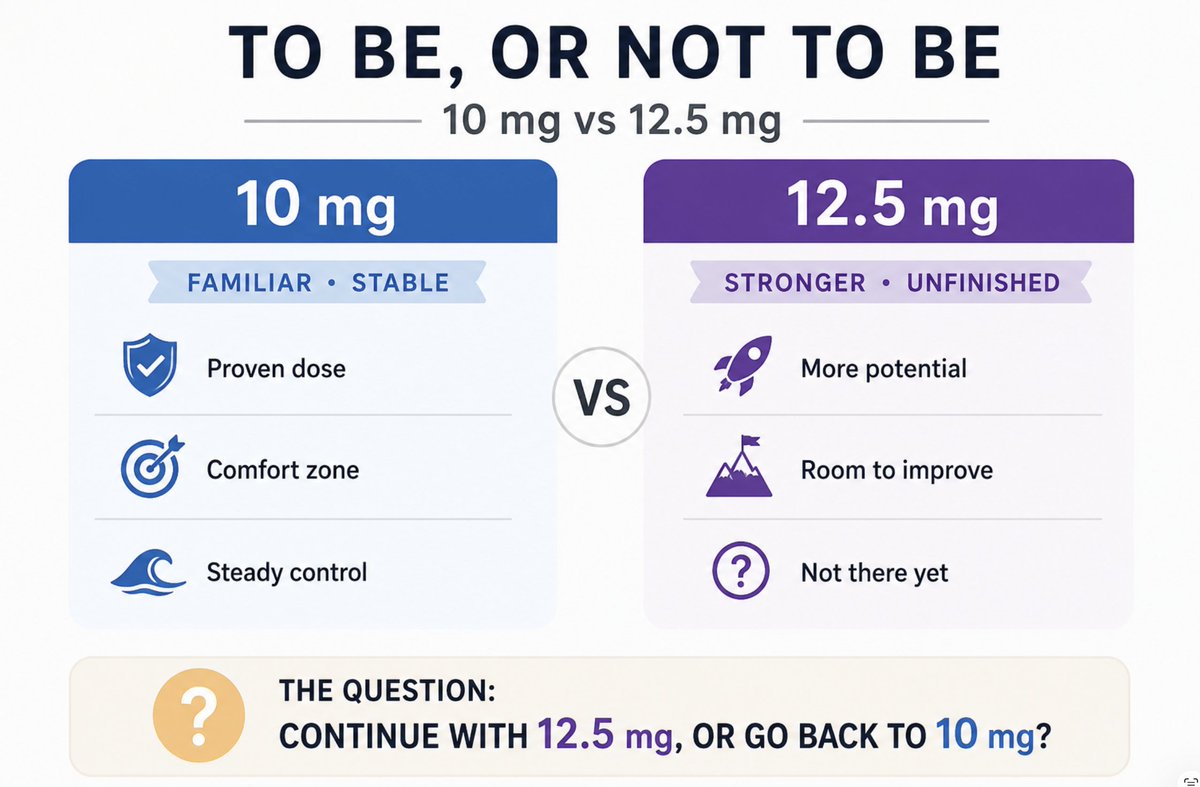
12.5 mg has not yet given me insulin independence. So the question now is: stay on 12.5 mg, or go back to 10 mg?
To be, or not to be.
1
1
178
May 14
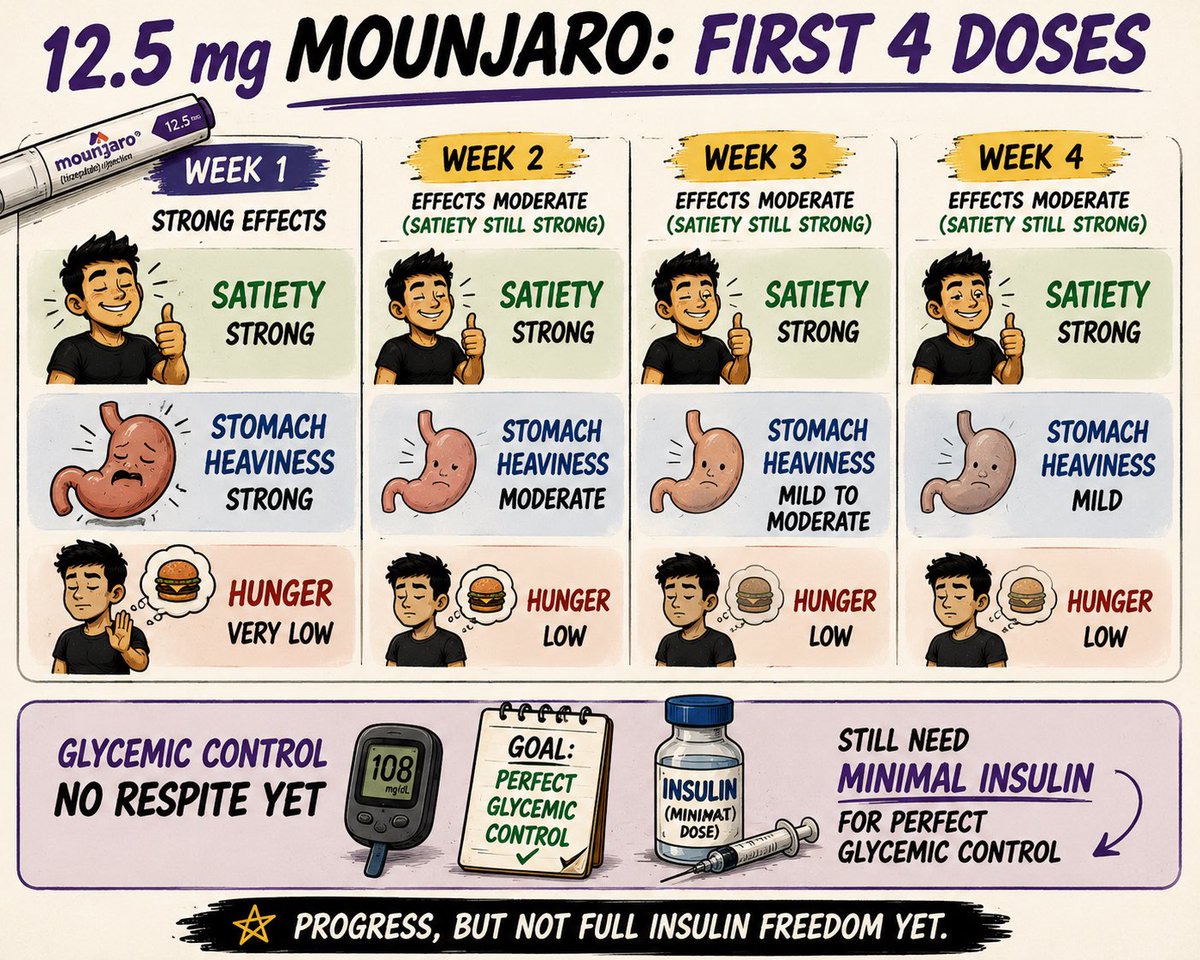
Four doses into 12.5 mg Mounjaro:
Week 1 hit hard — strong satiety, stomach heaviness, reduced hunger.
From week 2 onward, satiety remains, but the other effects have softened.
I still need small doses of insulin for perfect glycemic control. No insulin independence yet.
1
1
364
May 13
Survodutide looks promising, but not revolutionary on weight loss alone.
16.6% mean weight loss at 76 weeks is strong, but the real intrigue is the GLP1 glucagon biology and what it may do for fatty liver / MASH.
Potential niche drug. Not yet a Zepbound killer.
healthline.com/health-news/n…
1
187
May 12
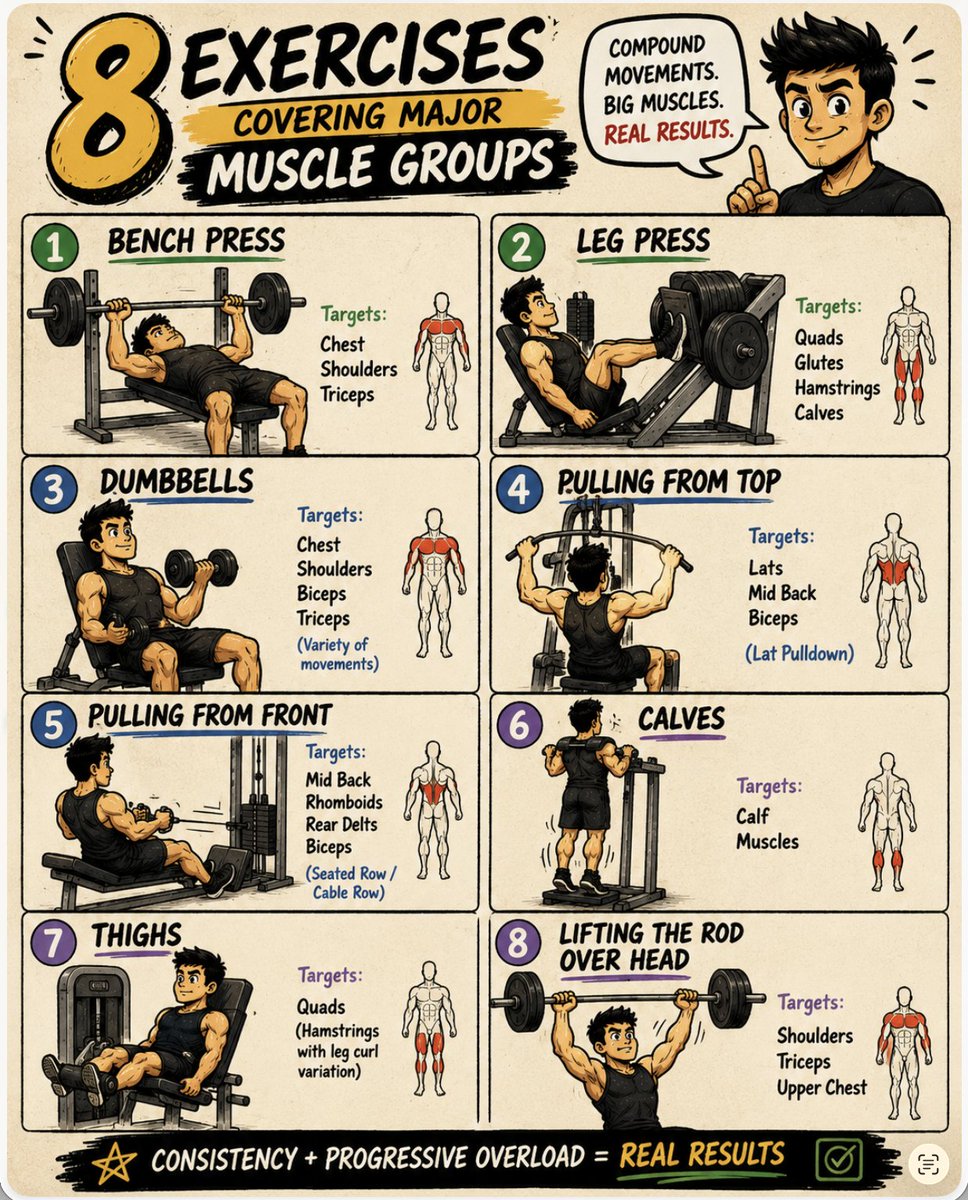
The 8 exercises I am using to cover the major muscle groups:
Bench press
Leg press
Dumbbell work
Lat pulldown (pulling from top)
Seated row / cable row (pulling from front)
Calf raises
Leg extension / leg curl for thighs
Overhead press
Simple. Basic. Effective.
1
1
158