
I’m here to learn. Current Interests (including, but not limited to): Vape hacking, terrariums, SARD/lupus tracking, UV exposure wearables, carnivorous plants
Joined August 2020
- Tweets 513
- Following 279
- Followers 164
- Likes 1,422
105 Photos and videos












Pinned Tweet

Jun 8
I posted this to Reddit, but I figure it deserves to be here too.
We don’t actually know how many people have lupus, and I am confident this is harming patients:
Since being diagnosed, lupus has become one of my special interests (I’m autistic, so when I say that, I mean it in the full-blown “I have read every paper I can find and have built many SARD specific tools” sense). And something keeps happening: the more I learn, the more lupus I find. In my own family: three generations of women on my father’s side, all in central Oklahoma, all with SLE. Among coworker’s family members or themselves. Among friends and friends of friends. Some of my clinicians. Everywhere I look, lupus, or some flavor of it (MCTD, DM, Incomplete lupus, cutaneous, UCTD.. you get the drift) seems to exist in one way or another.
For a while I wondered if this was just the Baader-Meinhof effect, you buy a red car and suddenly every car on the road is red. But then I started reading how SLE prevalence is actually measured in this country, and I realized: it might not be that I’m suddenly noticing lupus everywhere. It might be that lupus actually is everywhere, and we’ve just never properly counted.
I’m posting this because of the recent thread here about racial prevalence of lupus after that interview between those two people I’ve never heard of were posted saying incorrect things about lupus prevalence. There were some good points made in the thread, but I think the conversation was missing a critical piece: the numbers we’re all arguing about are far less solid than most people realize, and that uncertainty isn’t just academic; it’s shaping how our doctors and society views us, and ultimately shapes health outcomes down the line.
Here’s the situation:
SLE is not a nationally reportable disease. Unlike cancer, TB, or HIV, no one is required to report new lupus cases to any central database. There is no national lupus count. What we have instead are estimates, built from a small number of regional registries.
The number most commonly cited in research, about 204,000 Americans with SLE, comes from a 2021 meta-analysis (Izmirly et al., Arthritis & Rheumatology) that pooled data from five CDC-funded registries. Those registries covered portions of Georgia, Michigan, California, New York, and the Indian Health Service. The data was collected between 2002 and 2009, then extrapolated to the 2018 census. The authors themselves describe this as likely representing a lower bound.
The older “1.5 million” number the Lupus Foundation uses? That comes from a 1994 telephone marketing survey.
Neither of these is a count. They’re estimates built on estimates.
And when a different methodology is used, a nationally representative population survey (MEPS, 2016–2018), the number roughly doubles. That study found a prevalence of 195 per 100,000, which translates to around 490,000 adults with SLE.
Why does this gap exist? I propose several reasons:
The registries used ACR classification criteria to define cases. These criteria were designed for research classification, not clinical diagnosis. The Lupus Foundation itself has noted that at one major academic medical center, only half of patients actively receiving lupus treatment met those criteria at that time, or ever. So the registries were structurally designed to miss roughly half the population being treated.
The registries also excluded cutaneous lupus, incomplete lupus, and drug-induced lupus entirely. And they covered parts of five states, not the country.
Why this matters for you, personally:
When a doctor “knows” that lupus is rare and primarily affects young Black women, that shapes how they evaluate every patient who walks in. A white woman with fatigue and joint pain gets worked up differently than a Black woman with the same symptoms. An older patient gets told it’s “probably not lupus.” A man doesn’t even get considered.
1
142
Jun 8
I posted this to Reddit, but I figure it deserves to be here too.
We don’t actually know how many people have lupus, and I am confident this is harming patients:
Since being diagnosed, lupus has become one of my special interests (I’m autistic, so when I say that, I mean it in the full-blown “I have read every paper I can find and have built many SARD specific tools” sense). And something keeps happening: the more I learn, the more lupus I find. In my own family: three generations of women on my father’s side, all in central Oklahoma, all with SLE. Among coworker’s family members or themselves. Among friends and friends of friends. Some of my clinicians. Everywhere I look, lupus, or some flavor of it (MCTD, DM, Incomplete lupus, cutaneous, UCTD.. you get the drift) seems to exist in one way or another.
For a while I wondered if this was just the Baader-Meinhof effect, you buy a red car and suddenly every car on the road is red. But then I started reading how SLE prevalence is actually measured in this country, and I realized: it might not be that I’m suddenly noticing lupus everywhere. It might be that lupus actually is everywhere, and we’ve just never properly counted.
I’m posting this because of the recent thread here about racial prevalence of lupus after that interview between those two people I’ve never heard of were posted saying incorrect things about lupus prevalence. There were some good points made in the thread, but I think the conversation was missing a critical piece: the numbers we’re all arguing about are far less solid than most people realize, and that uncertainty isn’t just academic; it’s shaping how our doctors and society views us, and ultimately shapes health outcomes down the line.
Here’s the situation:
SLE is not a nationally reportable disease. Unlike cancer, TB, or HIV, no one is required to report new lupus cases to any central database. There is no national lupus count. What we have instead are estimates, built from a small number of regional registries.
The number most commonly cited in research, about 204,000 Americans with SLE, comes from a 2021 meta-analysis (Izmirly et al., Arthritis & Rheumatology) that pooled data from five CDC-funded registries. Those registries covered portions of Georgia, Michigan, California, New York, and the Indian Health Service. The data was collected between 2002 and 2009, then extrapolated to the 2018 census. The authors themselves describe this as likely representing a lower bound.
The older “1.5 million” number the Lupus Foundation uses? That comes from a 1994 telephone marketing survey.
Neither of these is a count. They’re estimates built on estimates.
And when a different methodology is used, a nationally representative population survey (MEPS, 2016–2018), the number roughly doubles. That study found a prevalence of 195 per 100,000, which translates to around 490,000 adults with SLE.
Why does this gap exist? I propose several reasons:
The registries used ACR classification criteria to define cases. These criteria were designed for research classification, not clinical diagnosis. The Lupus Foundation itself has noted that at one major academic medical center, only half of patients actively receiving lupus treatment met those criteria at that time, or ever. So the registries were structurally designed to miss roughly half the population being treated.
The registries also excluded cutaneous lupus, incomplete lupus, and drug-induced lupus entirely. And they covered parts of five states, not the country.
Why this matters for you, personally:
When a doctor “knows” that lupus is rare and primarily affects young Black women, that shapes how they evaluate every patient who walks in. A white woman with fatigue and joint pain gets worked up differently than a Black woman with the same symptoms. An older patient gets told it’s “probably not lupus.” A man doesn’t even get considered.
1
142
Jun 8
And then we can’t forget about the general issue with many, not all, clinicians not trusting the reporting of pain and vague symptoms from women of any race or economic background.
But we can’t actually say with confidence how lupus prevalence breaks down by race or geographic region, because the counting methodology itself has racial blind spots. The IHS registry in Oklahoma, covering Native American patients, validated fewer than 10% of potential cases, compared to 35-40% in other regions (Ferucci et al. 2014, Arthritis & Rheumatology). Was that because Native Americans in Oklahoma don’t get lupus? No. It was because IHS Oklahoma had limited rheumatology infrastructure at the time the data was collected. That wouldn’t exist until 2011. They conducted their census in 2009.
We observe disparities in every study that’s been done. Black women consistently show higher rates, and by all accounts that demographic appears to have more aggressive disease. But we cannot say how much of the observed disparity is biology versus access, detection, and counting methodology, because the counting itself is incomplete.
The perception that lupus is rare is not a fact. It’s an artifact of not conducting an accurate census. And that artifact has clinical consequences every time one of us sits in an exam room and gets told our symptoms are probably anxiety.
This may be contributing to the 6-7 year average for diagnostic delay. Which then in turn leaves more time for organ damage accrual and missed opportunities for earlier interventions, which are often less costly and allow patients to remain working and stay off disability for longer periods.
I am not saying this is a doctor problem or a bureaucratic problem or a patient problem or a race or sex problem.
This is a simple numbers problem.
We need to start reporting cases of SLE (and other lupus-associated diseases) to a national registry. This will improve health outcomes, research funding, and save lives of those who are caught far beyond just joint aches and rashes.
Sources:
•Izmirly et al. 2021, “Prevalence of SLE in the United States” — Arthritis & Rheumatology 73(6):991-996 stacks.cdc.gov/view/cdc/1068…
•Ferucci et al. 2014, “Prevalence and Incidence of SLE in a Population-Based Registry of AI/AN People, 2007-2009” — Arthritis & Rheumatology 66(9):2494-2502 acrjournals.onlinelibrary.wi…
•Engel-Nitz et al. 2022, “Real-world burden of SLE in the USA: MEPS 2016-2018” — Lupus Science & Medicine 9:e000699 pubmed.ncbi.nlm.nih.gov/3560…
•Engel-Nitz et al. 2021, “Prevalence of SLE in the United States: Updated Population Representative Estimates from MEPS 2016-2018” — ACR Meeting Abstracts acrabstracts.org/abstract/pr…
•Engel-Nitz et al. 2021, “Racial Disparities in US Adults with SLE: Prevalence, Quality of Life, Comorbidities and Healthcare Costs” — ACR Meeting Abstracts acrabstracts.org/abstract/ra…
•CDC, “Detailed Fact Sheet: Systemic Lupus Erythematosus” (confirms SLE is not a reportable disease and recent national estimates are not available) cdc.gov/lupus/media/pdfs/nat…
•Lupus Foundation of America, “Why It’s Difficult to Determine Exactly How Many People Are Living with Lupus in the U.S.” (documents ACR criteria missing ~50% of treated patients) lupus.org/resources/how-many…
•Gatto et al. 2023, “The Global Epidemiology of SLE: Narrowing the Knowledge Gaps” — Rheumatology 62(S1):i4-i16 academic.oup.com/rheumatolog…
•Duarte-García et al. 2022, “The Rising Incidence and Prevalence of SLE” — Annals of the Rheumatic Diseases (43-year Olmsted County data showing increasing incidence) stacks.cdc.gov/view/cdc/1328…
78
Jun 7
Um, making a case is hard. This is my futile attempt with acrylic and silicon, and because I don’t have normal super glue, nail glue. It’s the same but it comes in a pink bottle.
I might need to learn how to make a design to 3D print a case.
8
10
643
Jun 7
And yes, I have a husky, and it’s shedding season. Actually, that’s just all year, it’s *extra* shedding season
2
29
Jun 7
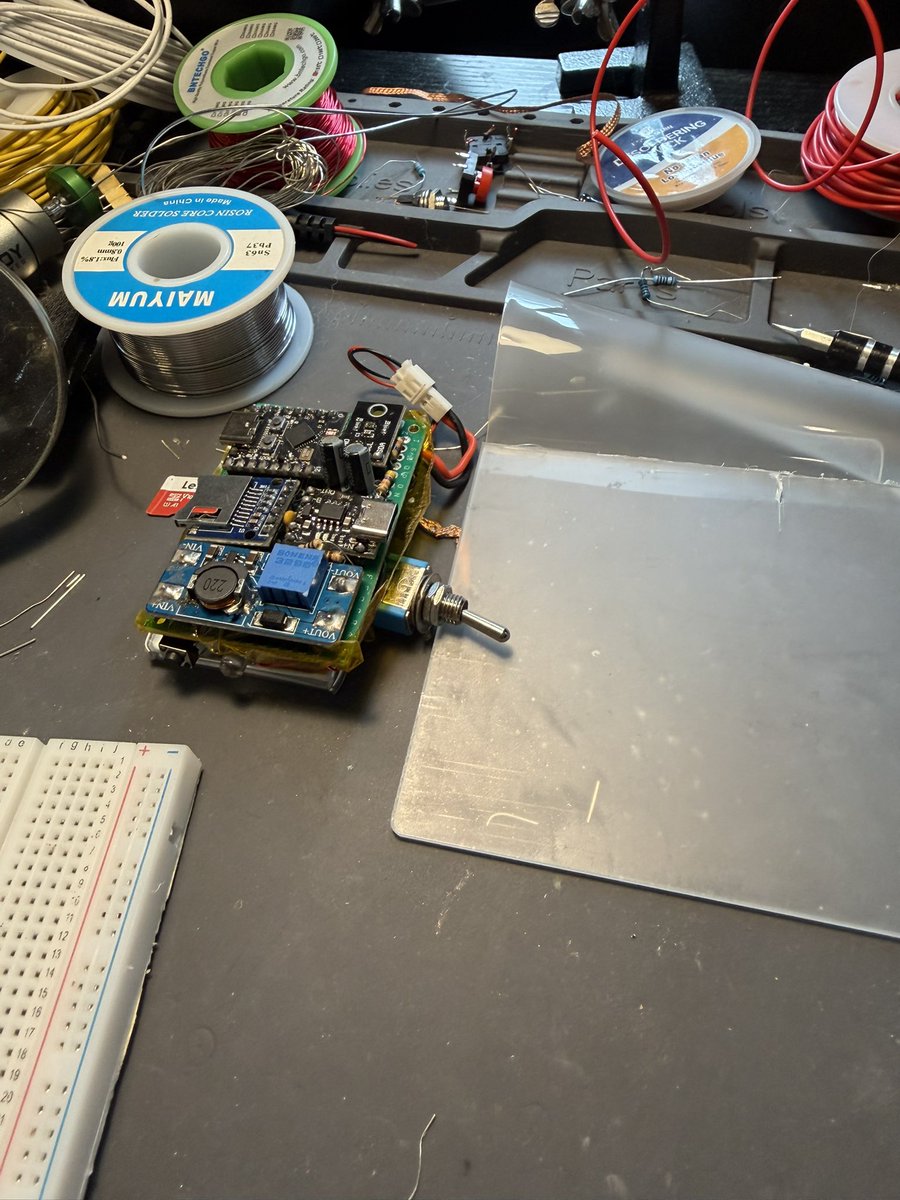
This is my pile of breakouts that has a slimmer profile than my earlier pile of breakouts, that does succeed at its designed purpose of sampling UVA/UVB light and syncing with over WiFi/BLE to drop it all in my pi4 flask server for my flare forecasting app.
1
2
41
Jun 7
The first “case”, its disguised as e-waste. It’s an aesthetic, trust me.
1
27
Jun 1
Just had a lovely evening talking about sardine tracker with a fellow luper. Building out the android companion app for her. I’m so curious how the model will perform for her, excited too!
1
31
May 30
I wish I could give other people chunks of my sleep-hours, like a timeshare. I’ll give you 14 hours of sleep and you can give me like 6 hours of productivity and awakeness. Deal?
2
4
288
May 25
I love how Temu says “buy our fast fashion” but then promotes what I guess would be good things for a mobile vet office?
Low key want the ultrasound just so I can I dunno, look at my dogs intestines or the wiring in the wall. Can you see wiring with an ultrasound? What other things can we see with it?

37
May 25
Fun fact: we can’t confidently say lupus is rare, we haven’t been actually reporting case numbers. All of the numbers we have are best guessed based of regional approximation. The last census attempt in Oklahoma was done in the Indian Health Services system and rendered 30 SLE patients in 2009, before IHS had a rheumatology leg to speak of. That wouldn’t happen until 2011.
Lupus isn’t rare, I simply can’t accept that.
Lupus is uncounted.
1
46
May 25
My own family has THREE generations of women with lupus, all along the patrilineal line, all born and raised in central Oklahoma.
And we know other lupus patients.
We aren’t an outlier, we simply aren’t being counted.
1
40
May 25
Here’s a relevant paper, but there are more I ought to synthesize to bolster my argument.
But it’s plain to see, we’re undercounted, not rare.
I’ll add that my family is mixed, with euro descended and native descended ancestry. Myself and my aunt being entirely euro, and my two cousins being more mixed.
But we are all Okies. There’s a thread here and we aren’t reporting the numbers. Because we aren’t counting.
acrjournals.onlinelibrary.wi…
25
May 25
If the one thing the comes out of my having become sick is that we can finally start simply counting who has lupus, I’ll be happy.
This is a hill worth dying on, because not knowing is likely one of the reasons SLE is in the top 20 causes of death for women in their childbearing years.
37
May 25
Had a get together with the Moore clan this Saturday, and my two cousins and aunt who all have lupus along with myself, agreed to look into enrolling in the Lupus Family Registry with me. Now, I guess it’s on me to figure out how to do that.
It was also really healing to get to talk about our experiences and we all learned that we have the same red chest rash, instead of the classic malar. Though we all have hyperpigmentation in the malar distribution.
It’s absolutely fascinating, and I’m so grateful that we can have these conversations and they don’t find my autistic drive to learn everything about our disease annoying.
For once, I had an audience of the exact people I want to help the most. My kin, and families like ours.
35
May 25
This here is Koda, he’s the best, he’s also a dust bunny factory. My life is fur right now. There is no escape.
74
May 20
What’s the name for this connector? Horizontal flex ribbon connector? Top down?

3
2
135
May 19
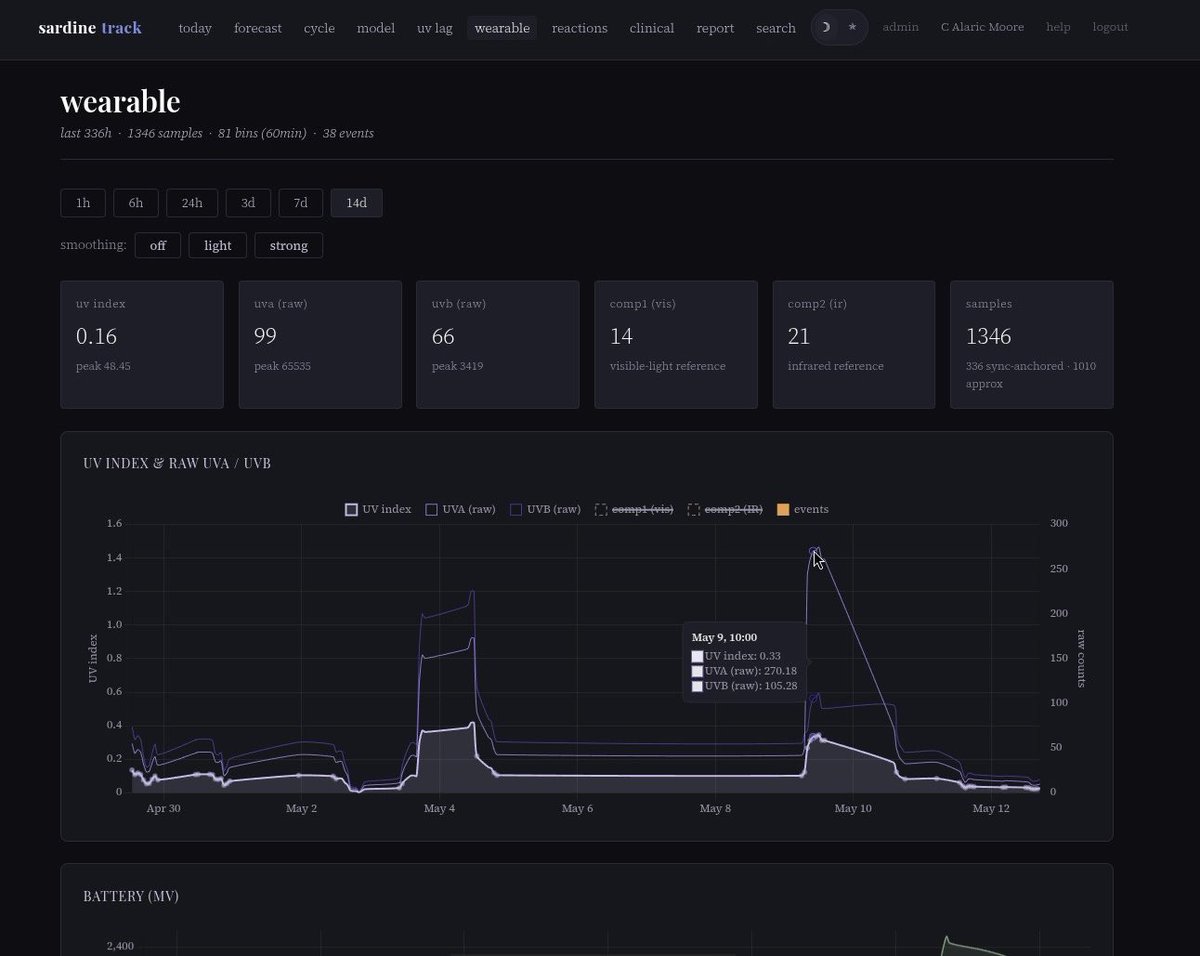
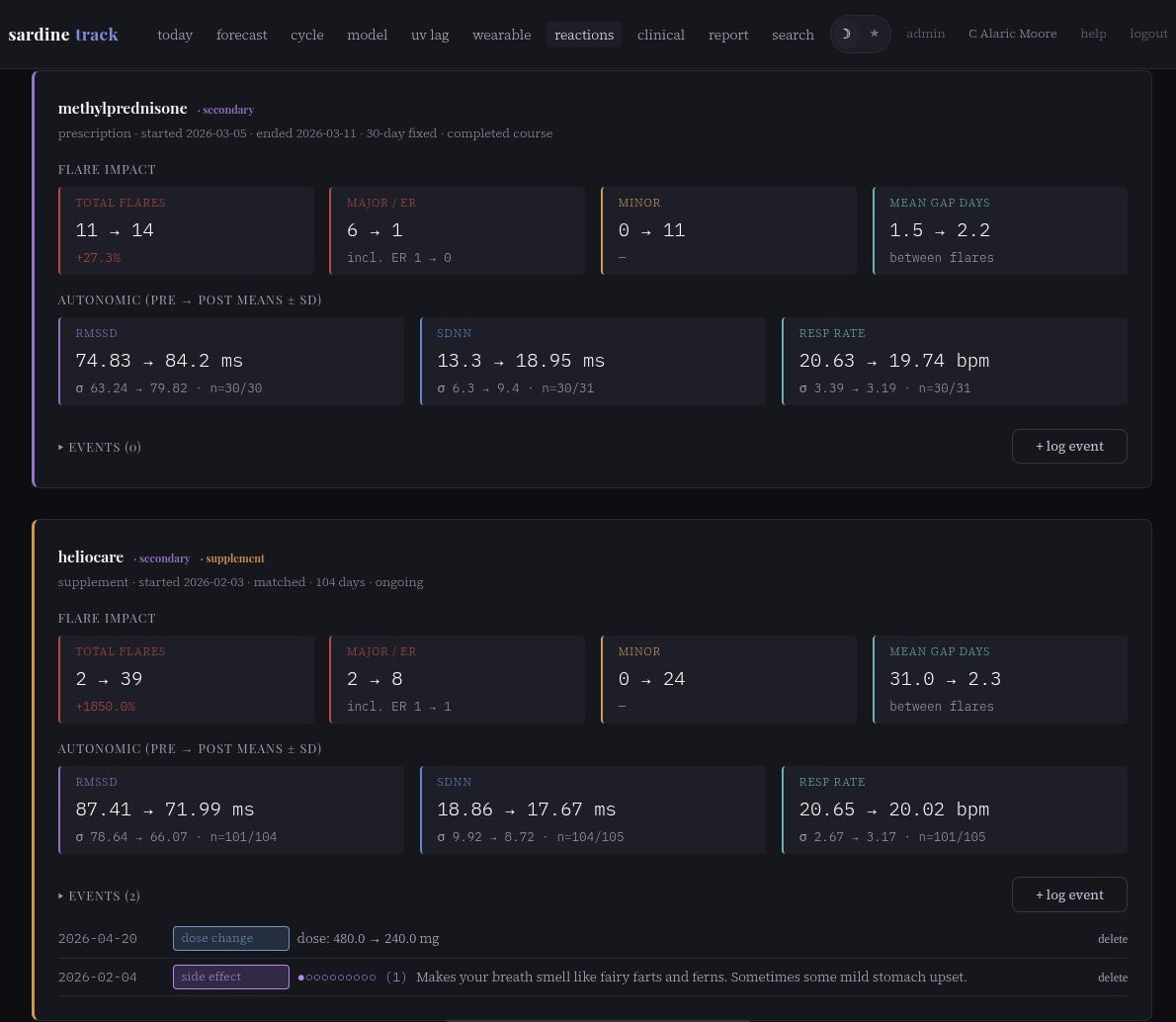
It doesn’t look like much at first glance, but this here is the “reactions” view of sardinetrack wherein I see what effect, whether positive or negative, various chemical interventions may have on my lupus.
Omitted here is of course my subjective experience with these medications, save for perceived side effects. Some meds may seem like they are not working quite yet by the numbers here, but at least two of these meds take a while to reach therapeutic doses. HCQ being famous for this.
Heliocare is a supplement derived from a fern, I still can’t tell if it helps. We’ll give it time.
Steroids are magical devil pills. Be wary of a quick fix. They also somehow taste like Molly but without the euphoria, just irritability.
1
43
May 18
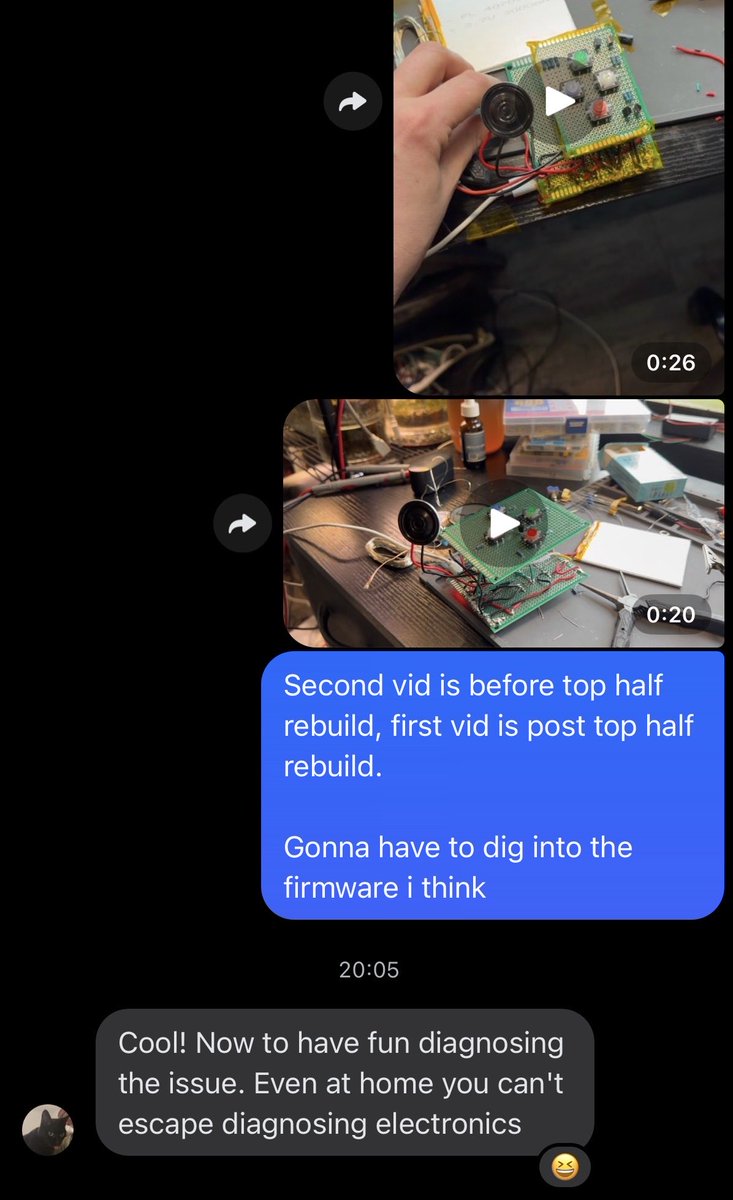
Shared the project of the week with a coworker, and got reminded that I compulsively desire the de-bug process.
Once Simon is finished I think we’re back to vape hack. It’s time.
2
57
May 18
My daddy came to mow my lawn today (my bubbas apparently couldn’t be bothered to wake up early enough), and we had a good breakfast and my lawn is now much nicer. Then I went out and noticed this, my father’s calling card, the ever present bungie cord.
He loves these things. Myself as a sailor, I hate them. But I forgive him, he’s family after all.
(But really, just tie a damn knot.)
1
1
86
May 18
The whole lawn thing has been a big deal. My photosensitivity because of the lupus is… stupidly extreme. The fluorescent lights at the USPS training center have been making me sick, with 100 SPF on!
My dad is a former green beret, HALO SCUBA, from the ‘70s. I got this disease from his side of the family, he has RA. It’s become apparent to me that he’s felt guilt about me becoming sick, but how do I help a man who’s used to being control come to terms with something that feels uncontrollable?
You give him instructions.
I asked my daddy to help me, and I gave him a specific task. Mow my lawn. I’ll make breakfast.
It was a really good time and it meant so much to me, and I think it helped my daddy feel more empowered about my having become sick.
And now I guess I have this bungie cord.
1
1
63