
Cardiology PGY5/ University of Tennessee, Nashville. tweets and opinions are mine.
Joined June 2014
- Tweets 630
- Following 6,501
- Followers 1,846
- Likes 8,462
181 Photos and videos












Pinned Tweet

Mar 24
Feeling deeply humbled to receive the Ascension Saint Thomas Guardian Angel Award, a recognition that comes from the kindness of our patients. Grateful to care for them alongside incredible team, and especially thankful to my clinic mentor Dr. Keswani! @AmitKeswaniMD @timir_paul
12
4
60
5,363
Jun 9
The biggest challenge in medical AI is no longer building models; it’s ensuring they are unbiased, externally validated, and effective in real-world practice.
My latest article in @AmJCardio examines these challenges and outlines a path toward responsible AI implementation
7
5
29
2,686
Neel Patel, MD retweeted

Cheers, chills, and a standing ovation when RASolute 302 showed unprecedented survival on daraxonrasib for patients with progressive pancreatic cancer
Seldom do you sense you’re witnessing a historic moment in cancer care but this feels like ras targeting has arrived
#ASCO26
92
1,273
6,504
1,151,890
Neel Patel, MD retweeted

May 31
One of the most amazing things I’ve ever seen: a standing ovation for the full Daraxonrasib results
I feel inspired and energised, to put it mildly — we have a targeted therapy for pancreatic cancer now, and nothing is undruggable anymore
104
1,499
9,558
1,975,086
May 15
Ascension St Thomas Research Symposium 2026
@UTHSCNashCVD @timir_paul @RoshanBista85 @SwotantraGautam @Nikita20892512 @kerrigjl


1
3
21
2,384
Neel Patel, MD retweeted

Apr 10
This viral thread from @bschermd is a great read.
Veins and arteries see the exact same LDL/ApoB, yet plaque forms almost exclusively in arteries — and a pristine vein grafted into arterial flow rapidly develops atherosclerosis.
That points strongly to hemodynamic stress and endothelial injury as the primary trigger (Response to Injury) over a pure Response to Retention model.
Our Keto-CTA data in a metabolically healthy cohort with a wide spread of LDL/ApoB (going from under 100 to over 500) show no association with either the presentation or progression of plaque.
Which is why we've needed to do this exact research for so long.
This central illustration is from our match analysis in JACC Advances (Budoff et al., 2024), where we compared 80 metabolically healthy ketogenic hyper-responders (mean LDL-C 272 mg/dL, HDL-C 90, TG 64, after 4.7 years on keto) to 80 tightly matched controls from the Miami Heart cohort (mean LDL-C 123 mg/dL).
Despite the ~149 mg/dL difference in LDL-C, there was no significant difference in coronary plaque burden by CCTA total plaque score, CAC score, or other measures. And crucially, there was no correlation between LDL-C levels and plaque burden in either group.
(Full paper: jacc.org/doi/10.1016/j.jacad…)

Apr 9

Your veins and arteries carry the same blood. Same LDL. Same ApoB. Same everything. Yet veins almost never get plaque. Arteries constantly do.
Maybe you've seen the recent discussions about this. It's an interesting question that provides clues in cardiovascular science, and could challenge how we think about LDL and ApoB. 🧵
19
32
193
77,668
Apr 1

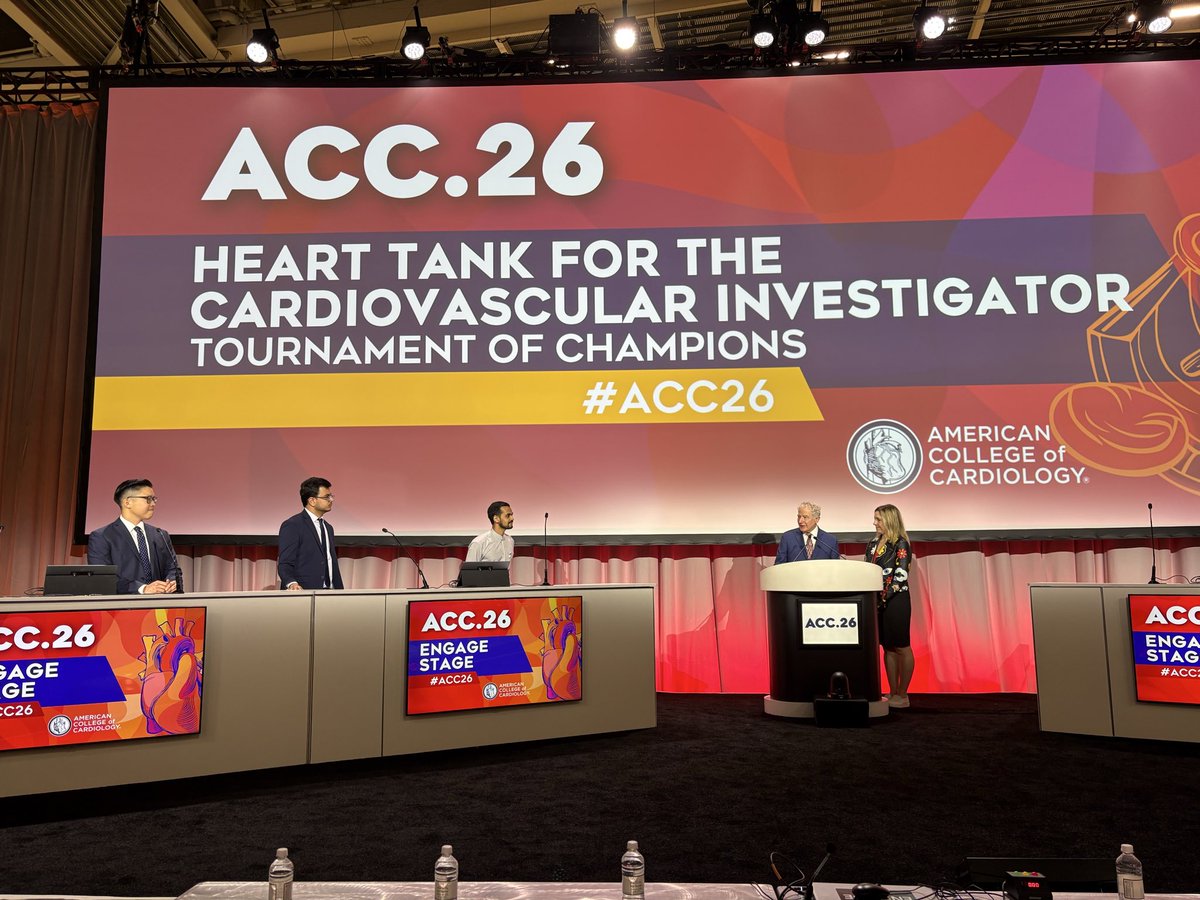
#ACC26 @JACCJournals @ACCinTouch @timir_paul @FITsOnTheGo @NPatelMD
Great presentation by Dr. Patel on ACC Heart Tank (Shark Tank)! Great to catch up with known colleagues.

2
16
1,692
Mar 31
Thank you so much, Dr Paul for the mentorship! @timir_paul @UTHSCNashCVD @kerrigjl @SasanRaissi @HadyLichaaM @evhaddad @RoshanBista85 @SwotantraGautam @zghouzi @Nikita20892512 @JastiManasa @MackennaDarling @ACCinTouch

So Proud of our fellow @NPatelMD at @UTHSCNashCVD who competed as top 3 at #ACC2026 HEART TANK competition


8
2
26
2,015
Mar 30
Grateful to contribute alongside such a talented group of social media ambassadors. #ACC26 was all about ideas, impact, and momentum 🔥❤️@ACCinTouch @JACCJournals @ACCmediacenter @Cardiology
Mar 30

Big shoutout to our amazing Social Media Ambassadors! 🎉
Your energy, expertise, and dedication helped make #ACC26 truly unforgettable. Thank you for sparking meaningful conversations, sharing your insights, and keeping the momentum alive 👏👏👏 @ACCinTouch


1
2
14
1,068
Mar 30


1
1
23
1,234
Mar 29


2
3
30
2,517

Mar 28
The faces behind the feed..
Grateful to be part of this incredible Social Media Ambassador team at ACC.26 in New Orleans. #ACC26 @ACCinTouch @ACCmediacenter
4
9
34
2,154
Neel Patel, MD retweeted

Mar 28
Eyes and ears of the ACC.26 👀👂
Great to connect with this amazing team dedicated to amplifying cardiovascular education worldwide. 🌍❤️
#SoMe team at #ACC26
@ACCinTouch @JACCJournals @Abdelcards @ZainAsadCardOnc @oliviacardio @MauroSotoMD @RThachilMD @Brian_RosePA @DPtheNP @Simona_Cochrane @lucreciamburgos @drcornejoa @ErrolMoras @AbenaKAgyekum @Kuseme_ @VictoriaTAraujo @CAESmedmd @markzroland @DrAnkitKPatel @Umair2017 @vicentejmzmd @AabuzaidDr @usman_aliakbar @MaximaMendez15 @Priyansh_Shah56 @amanpreet_wasir @BrunoLimaMDPhD @YJelwan @ErsozluSara @NPatelMD @christiankfuku @RonakBharucha @KAgarwalMD @palakpatel96 @drapurvapopat @SaadUrRahman55 @Zill_cardio @NjeriKuriaMD @IvanRafaelMD

4
10
21
1,503
Mar 28
Kicking off ACC.26 in New Orleans! Excited for the sessions, great conversations, competing in the Heart Tank and exploring NOLA over the weekend! #ACC26 @ACCinTouch @ACCmediacenter

1
18
785