
Joined May 2008
- Tweets 1,484
- Following 216
- Followers 4,031
- Likes 1,898
18 Photos and videos




Pinned Tweet

17 Nov 2021
Calling all little neurologists - we launched a children’s book called “Neurology in a Nutshell” explaining neurology to kids in a playful and educational way. Now available on Amazon: amzn.to/2ZBqqR2
#NeuroTwitter #MedTwitter
3
6
29
NEUROLOGY retweeted

15 Sep 2024
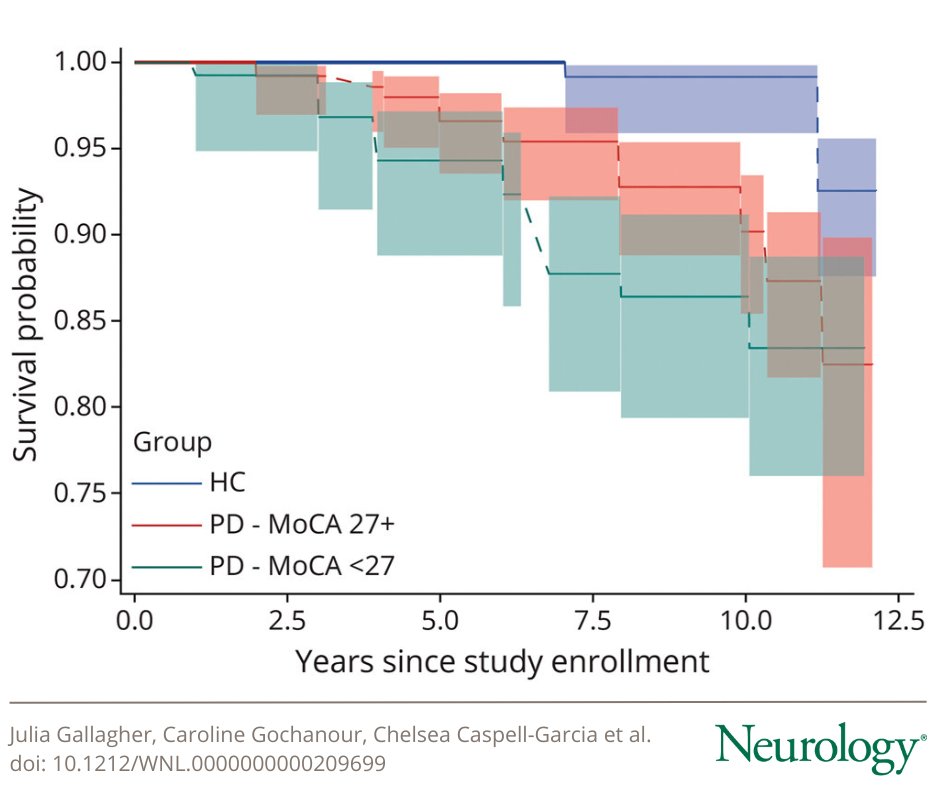
Results from two large, prospective studies suggest that dementia in Parkinson disease occurs less frequently, or later in the disease course, than previous research studies have reported: bit.ly/4dYBzg5
#NeuroTwitter
1
17
53
6,839
NEUROLOGY retweeted

14 Sep 2024
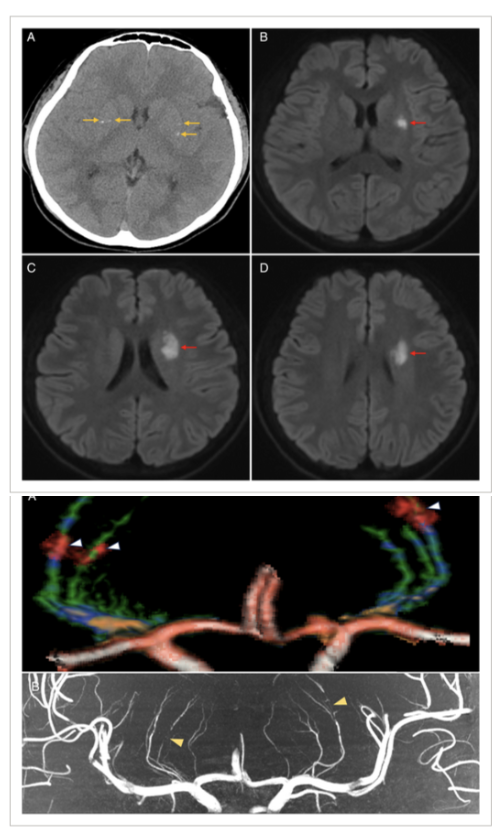
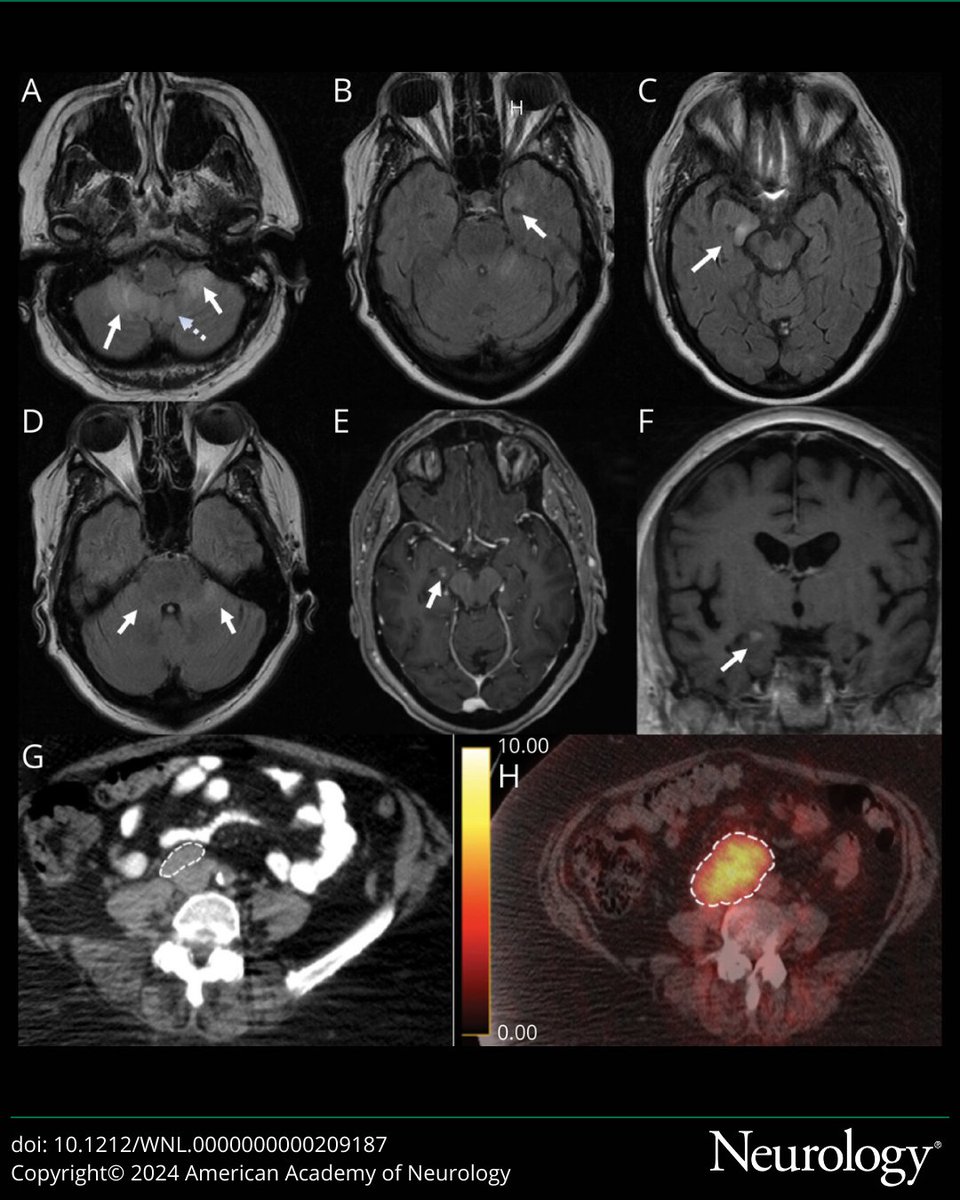
Have you seen this syndrome? Mineralizing lenticulostriate vasculopathy and traumatic infarction? Basal ganglia involvement and NO movement disorder. Great case in Annals of Neurology @TheNewANA1 by Li and colleagues.
Key Points:
- A 14 you had loss of consciousness.
- Then a transient generalized epileptic seizure followed.
- Bilateral basal ganglia punctate calcifications.
- 5 days later MRI acute infarction left putamen and anterior corona radiata.
- CT angiography 7 Tesla MRI showed 'calcifications next to bilateral lateral lenticulostriate arteries.'
- Bilateral lenticulostriate 'arteries stenoses.'
My take: This is a tricky diagnosis and the authors were able to show the 'mineralizing lenticulostriate vasculopathy based on the multimodality image findings and most important, the clinical presentation.' For clinicians, remember the CT is very useful to reveal and verify calcifications. I always marvel at scans with a lot of basal ganglia involvement w/o movement disorders.#basalganglia #neurology #neuroradiology #stroke
5
30
116
12,166
NEUROLOGY retweeted

14 Sep 2024
In this study, fecal microbiota transplantation (FMT) was safe, but did not improve Parkinson disease (PD) symptoms more than placebo. Improvements and microbiome changes after placebo warrant further research on FMT and bowel cleansing in PD. ja.ma/4d0DcJ7
6
7
3,203
NEUROLOGY retweeted

14 Sep 2024
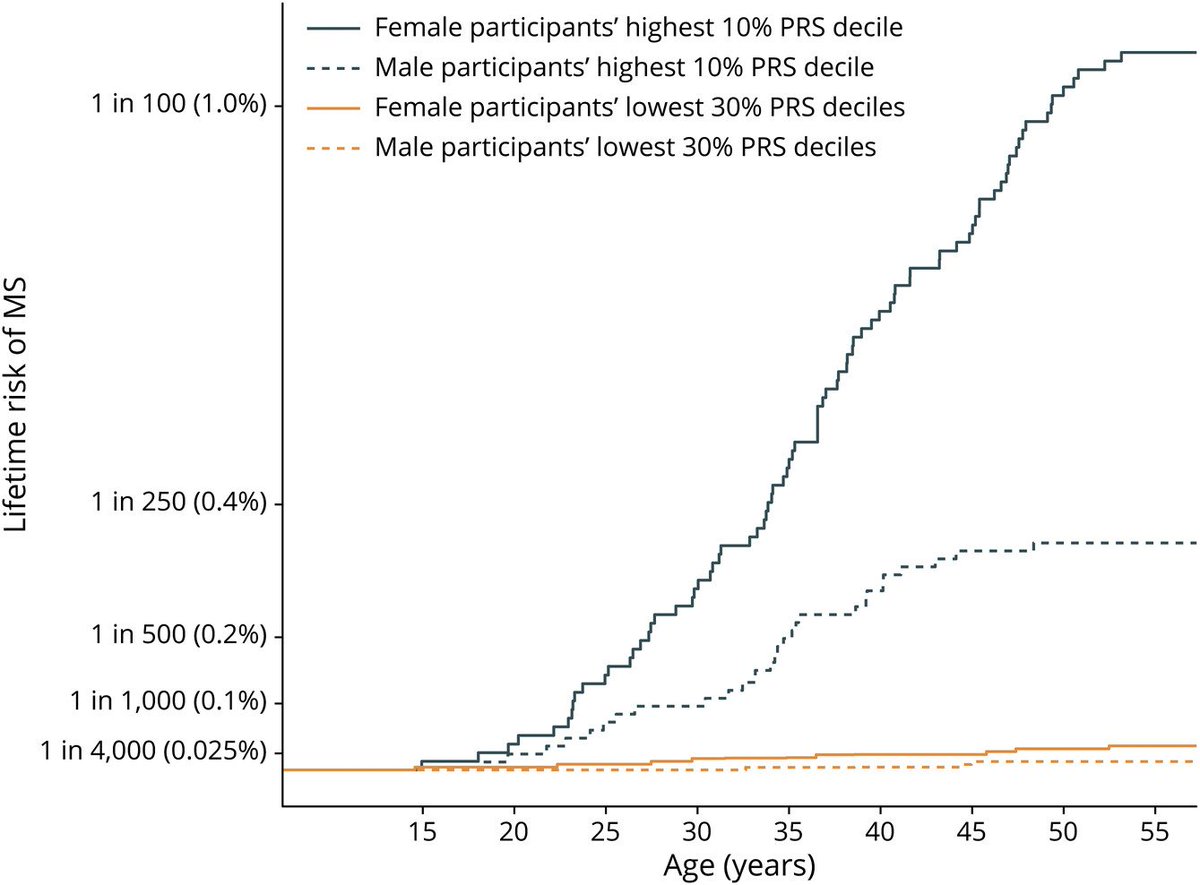
Anyone can get multiple sclerosis. This study found that for women in the Netherlands with the "lowest 30% genetic risk," they still had a 1 in 2,739 risk of MS (vs. 1 in 92 for women with the top 10% genetic risk). pubmed.ncbi.nlm.nih.gov/3927…
3
25
3,071
NEUROLOGY retweeted

25 May 2024
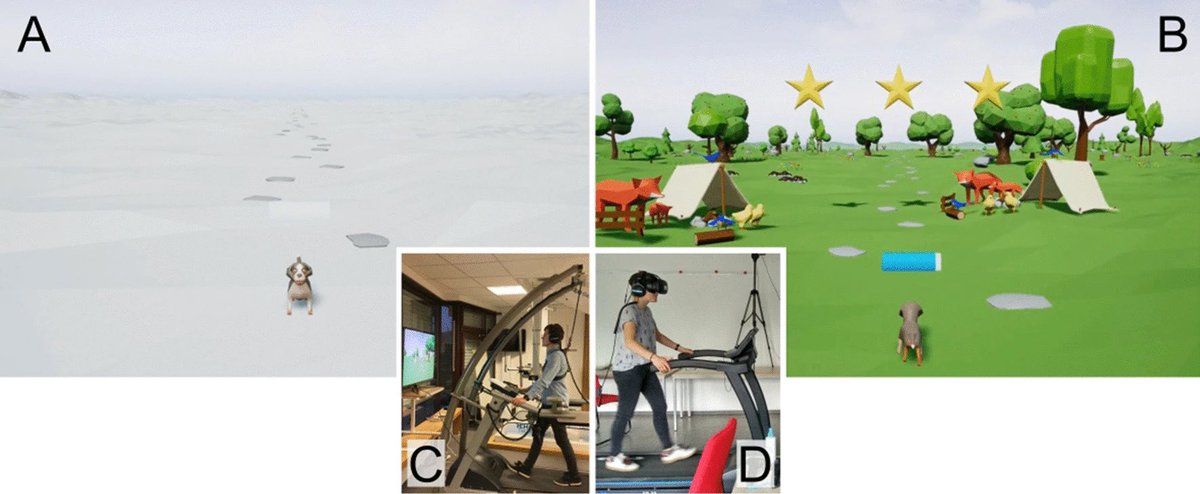
This is one of the largest meta-analyses on the effects of exercise on cognitive performance.
Here are my top 4 evidence-based protocols from it to leverage exercise to maximize cognitive performance.
1/13
20
795
3,712
851,458
NEUROLOGY retweeted

26 May 2024
Wish you had a sixth sense to localize that sixth cranial nerve palsy?
Feeling six feet under when you see a sixth nerve deficit?
Here’s a cheat sheet to help you locate the lesion in a sixth cranial nerve palsy!
Just remember the Six Syndromes of the Sixth Cranial Nerve!
There are six syndromes of CN6—one for each of its five stops along the way to its destination in the orbit—and one that is idiopathic
1. Brainstem
🔸CN6 nucleus is at the facial colliculus—looks like a baby’s butt of the brainstem
🔸Many important structures here
🔸Rarely get an isolated palsy & uniquely can get associated MOTOR deficits
2. Subarachnoid space
🔸CN6 exits under the dad bod belly of the pons & enters Dorello canal
🔸Susceptible to changes in intracranial pressure—can get stretched!
🔸ICP changes can cause BILATERAL palsies here
3. Petrous apex
🔸Exits Dorello canal & travels under the petroclinoid ligament, like under a seat belt
🔸Many other nerves here
🔸Rarely get an isolated palsy & uniquely can get associated HEARING deficit
4. Cavernous sinus
🔸Many nerves in close proximity!
🔸Rare to get an isolated palsy
🔸Many pathologies can affect the cavernous sinus—so many differentials & many deficits!
5. Orbit
🔸Short orbital course—quick lateral turn after the superior orbital fissure to innervate the lateral rectus
🔸Rare to have isolated palsy
🔸Get a SOF syndrome or orbital apex syndrome
6. Idiopathic
🔸No other identifiable etiology
🔸Like transverse myelitis—likely microvascular or post-inflammatory
🔸1/4th of CN6 palsies are idiopathic
But you must exclude the other five first!
Now you know the Six Syndromes of the Sixth Cranial Nerve.
Hopefully now when you see a CN6 palsy, there will never be six degrees of separation between you & the etiology!
19
162
562
43,546
NEUROLOGY retweeted
25 May 2024
Most viewed in the last 7 days from @JAMANeuro:
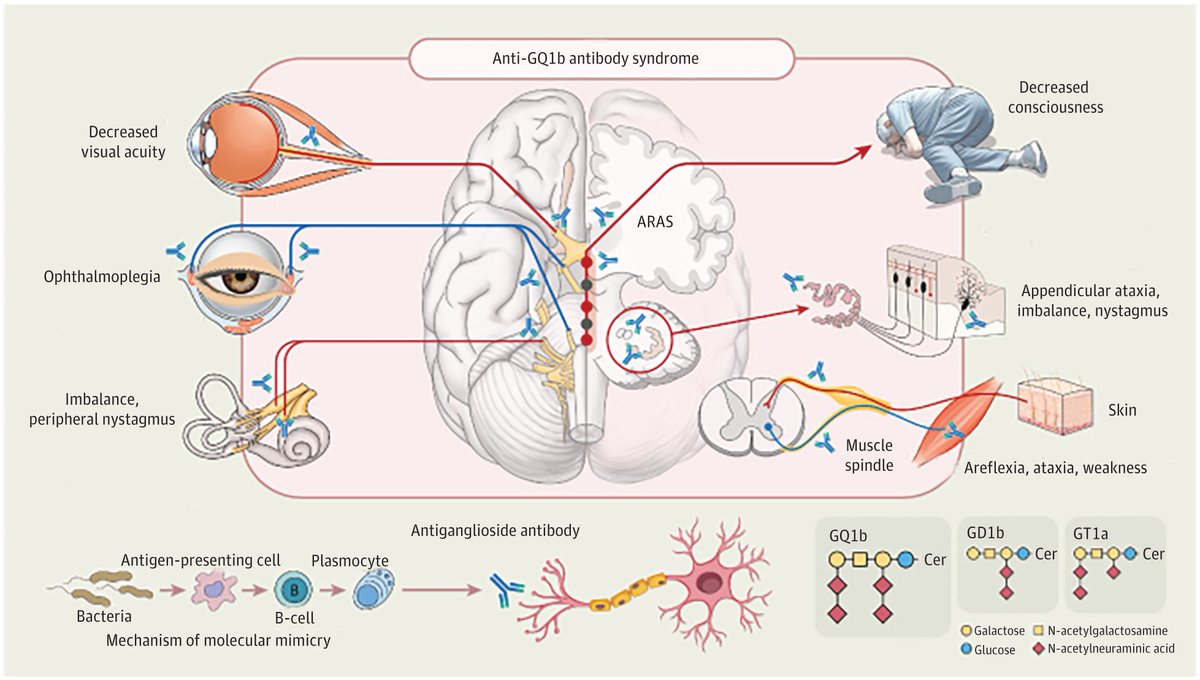
This narrative review describes the phenotypes of anti-GQ1b antibody syndrome to aid in its diagnosis in light of its various clinical presentations.
ja.ma/44W5u4Y
45
146
20,799
NEUROLOGY retweeted
16 Apr 2024
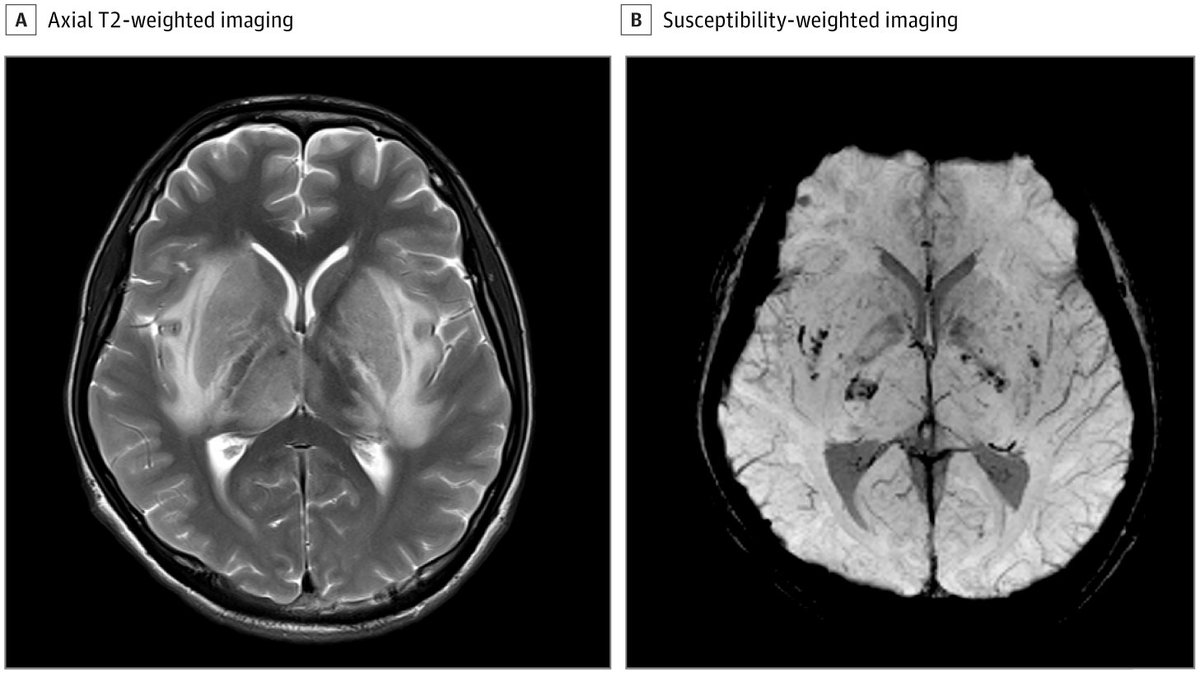
Case report: a 17-year-old boy with reduced consciousness and T2-weighted hyperintensity, focal diffusion restriction, and microhemorrhages within the deep gray nuclei and surrounding white matter.
ja.ma/49wJfDm
3
18
67
18,142
NEUROLOGY retweeted

6 Apr 2024
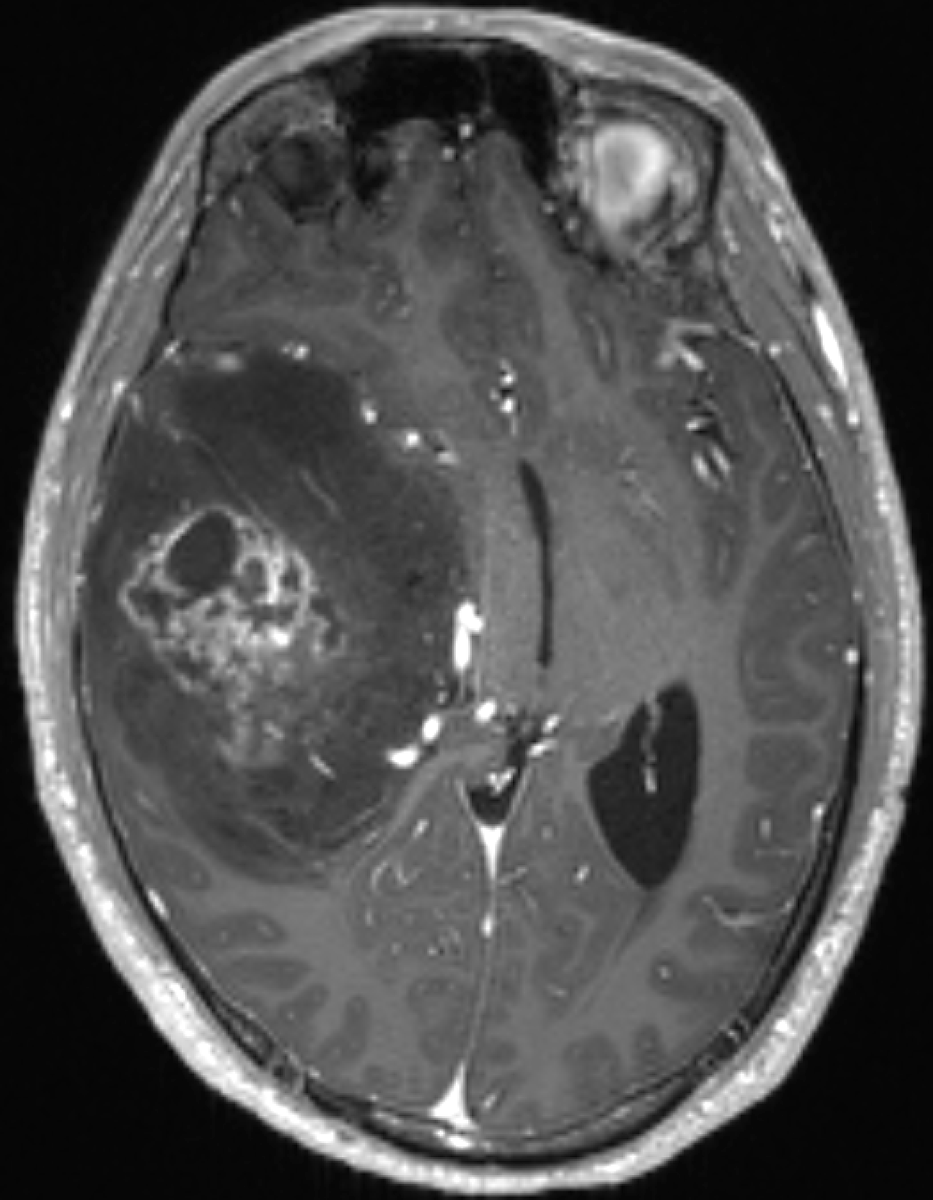
33 year old male presents with seizure. MRI reveals a brain tumor as shown. Can you make the WHO CNS 2021 diagnosis on this single image?
29
40
331
90,056
NEUROLOGY retweeted
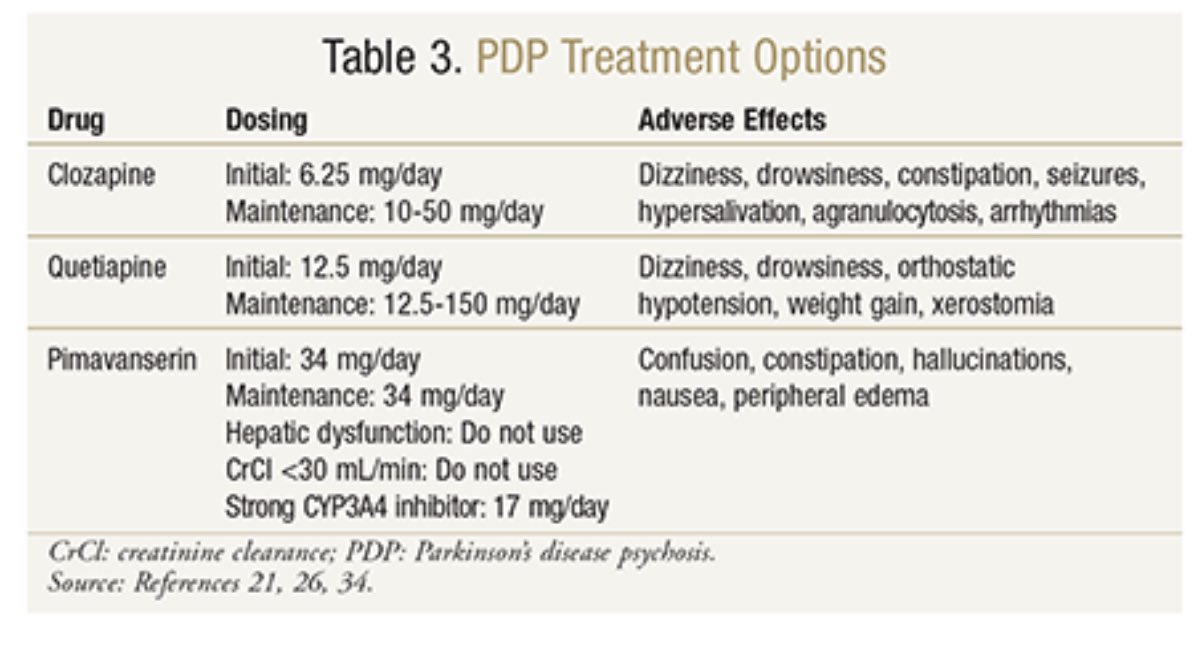
7 Apr 2024
If you have hallucinations, psychosis or paranoia with Parkinson and your clinician has tried all options short of medication, this is the key table you will need with the big 3 choices you should limit your team to using. We are seeing too many folks turn to atypical and typical antipsychotics which will make Parkinson worse. Nice article and chart. Note doses are much lower than in other conditions like schizophrenia. uspharmacist.com/article/tre… #parkinson also check out @ParkinsonDotOrg free medication book.
44
125
11,146
NEUROLOGY retweeted
30 Mar 2024
This case expands on the current knowledge of KLHL11-related autoimmune encephalitis including the paraneoplastic presentation, associated tumor types, and management of this syndrome in women: bit.ly/4ak2lNU
#NeurologyRF #NeuroTwitter
1
33
94
13,009
NEUROLOGY retweeted
31 Mar 2024
In pediatric-onset multiple sclerosis, initiating highly-effective rather than moderately-effective therapies may better control early disease activity and expose patient to less discontinuation due to inefficacy and intolerance. ja.ma/48Jw2GU
2
16
29
6,338
NEUROLOGY retweeted

28 Mar 2024
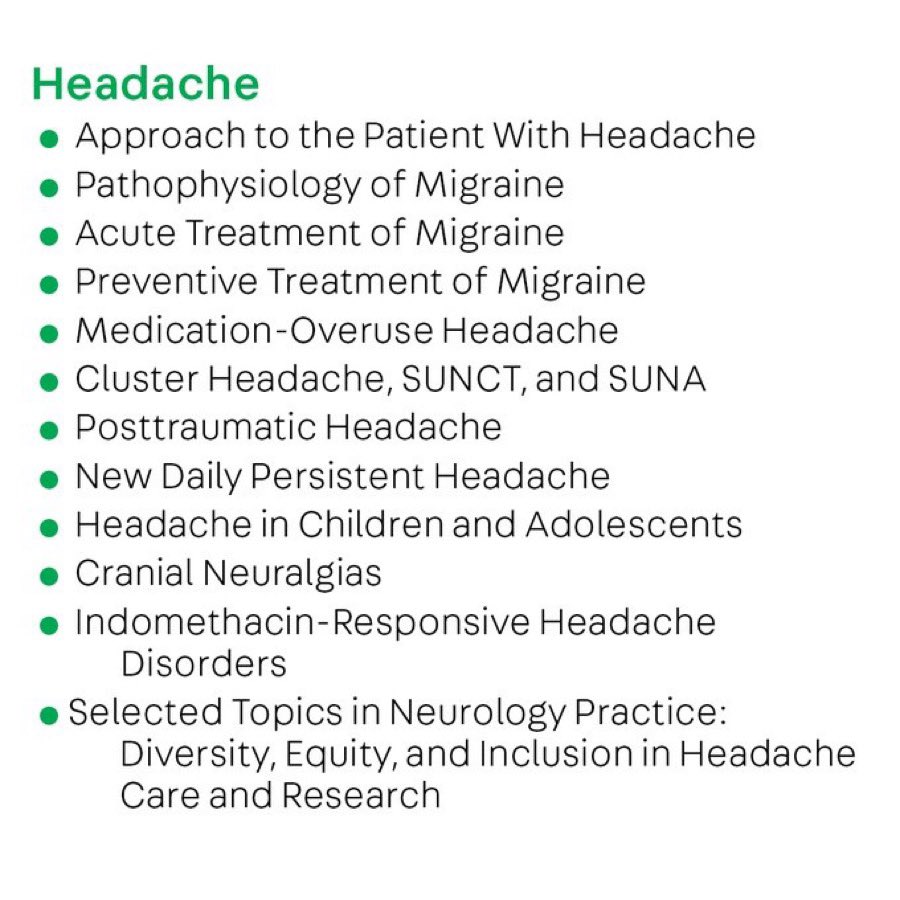
Our first Continuum issue on headache since 2021 publishes… next week!
Very excited for this issue. The amazing Dr. Amy Gelfand has put together an awesome list of topics and authors ⬇️
Much has changed in the world of headache, you won’t want to miss this one
2
38
169
16,083
NEUROLOGY retweeted
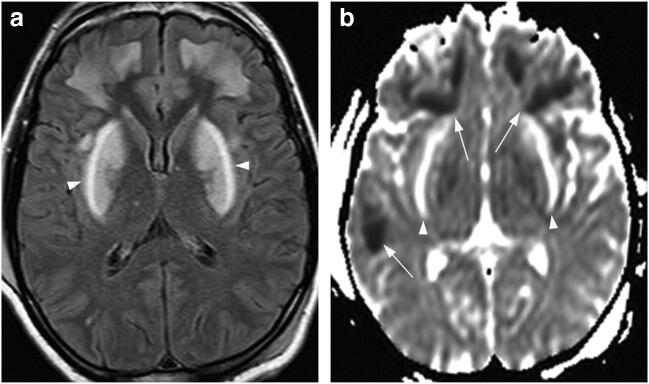
18 Mar 2024
31 year-old man with confusion and slowed movements a few days after ingesting home-made liquor. MRI showed these strange lesions (left side is ADC). Diagnosis?
8
16
87
12,799
NEUROLOGY retweeted
14 Mar 2024
Case report: the evaluation of a 44-year-old man with a history of headache, dizziness, and imbalance and imaging that showed lacunar infarctions and bilateral white matter hyperintensities. ja.ma/49L8P8J
1
16
53
10,460
NEUROLOGY retweeted

13 Mar 2024
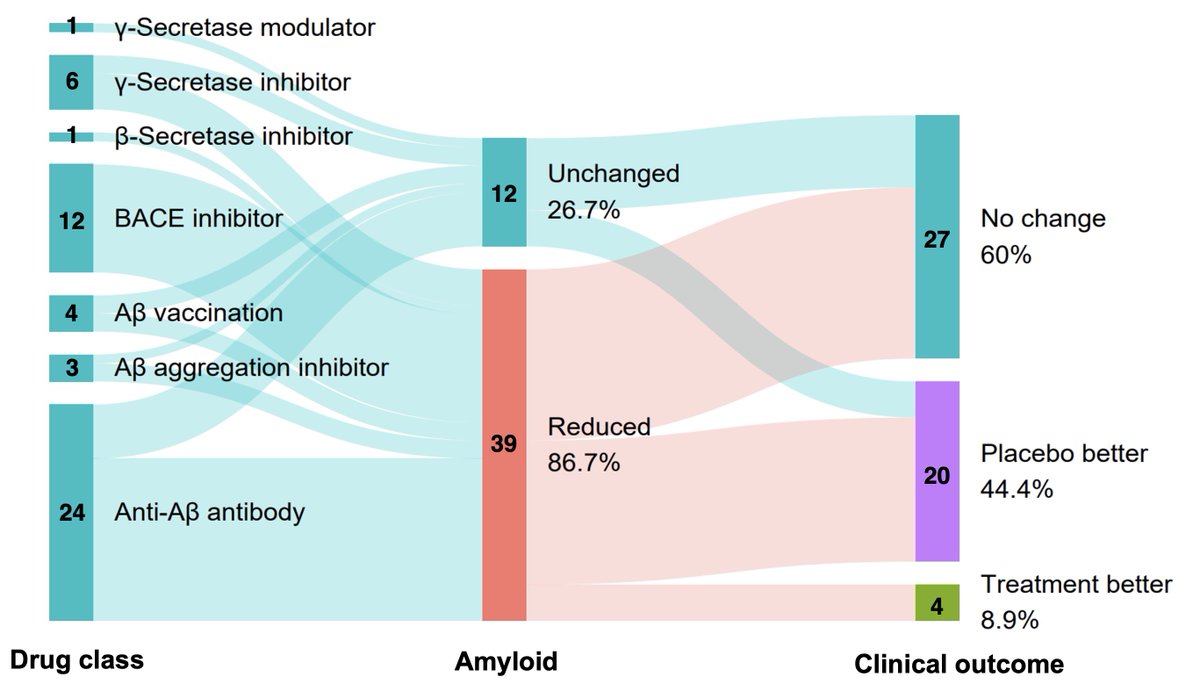
In two decades of anti-amyloid trials in #Alzheimers (2002-2023), placebo emerges as the historic winner.
Do No Harm: #Lecanemab is an accident, not a victory.
Presented today at #ASENT, Bethesda, @ASENT_Org.
4
33
132
12,478
NEUROLOGY retweeted
13 Mar 2024
1/Time to rupture all your misconceptions about aneurysms!
When you see an aneurysm on imaging, do you know it’s risk of rupture?
Do you know which features make one aneurysm more likely to rupture?
Here’s a short thread to teach you which aneurysms are bursting with risk!
21
145
454
40,970
NEUROLOGY retweeted
13 Mar 2024
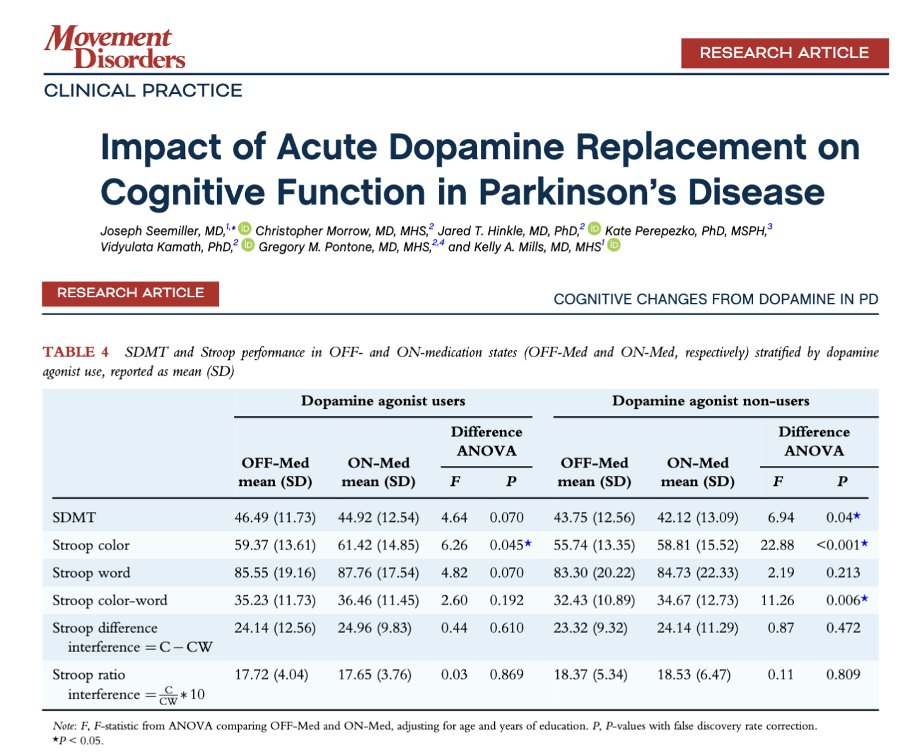
Does dopamine replacement affect cognitive (thinking) function in Parkinson's? Is it all about the motor? Guess what folks, Semiller, Pontone and Mills teach us about the aspects of cognition that 'change' on and off dopamine replacement therapy.
Key Points:
- The authors point out that there is 'striatal dopaminergic denervation in a posterior/dorsal to anterior/ventralgradient, leaving motor and associative cortico-striato-pallido-thalamic loops differentially susceptible to hyperdopaminergic effects with treatment.'
- The authors point out that we usually guide our dopamine replacement primarily by motor symptoms.
- They tested folks on and off dopamine replacement and guess what? 'Symptomatic medication differentially affected performance on two cognitive tests in Parkinson's.
- 'Core Stroop measures improved, Stroop interference was unchanged, and SDMT performance worsened, likely reflecting complex changes in processing speed and executive function related to acute treatment.'
My take: Dopamine replacement therapy can affect thinking and cognition. Thank you to these authors for reminding us to look more deeply and think beyond motor function.
movementdisorders.onlinelibr… #Parkinsons
4
30
101
8,574
NEUROLOGY retweeted

11 Mar 2024
This just published online in the Headache journal. Overwhelming evidence and clinical experience supporting the use of these transformative therapies as first-line approaches.
37
72
5,758
NEUROLOGY retweeted

29 Feb 2024
Most popular read this week: Findings from a large dataset paint a vivid picture of posterior cortical atrophy—including when it begins, the primary symptoms, and the pathological proteins involved: bit.ly/3SZXV90
#NeuroTwitter @AANMember
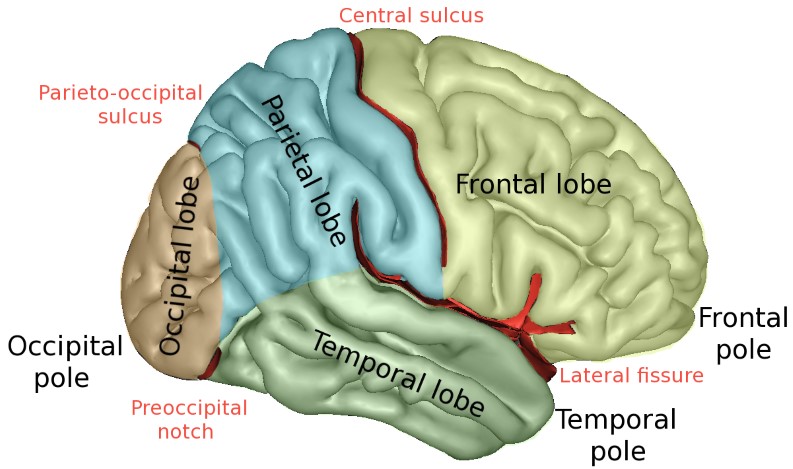
ALT A map of the human brain.
13
35
3,214