
Emeritus Professor USC. 50 Years of Experience in Endodontics Education and Practice.
Joined August 2015
- Tweets 418
- Following 262
- Followers 3,415
- Likes 42
174 Photos and videos




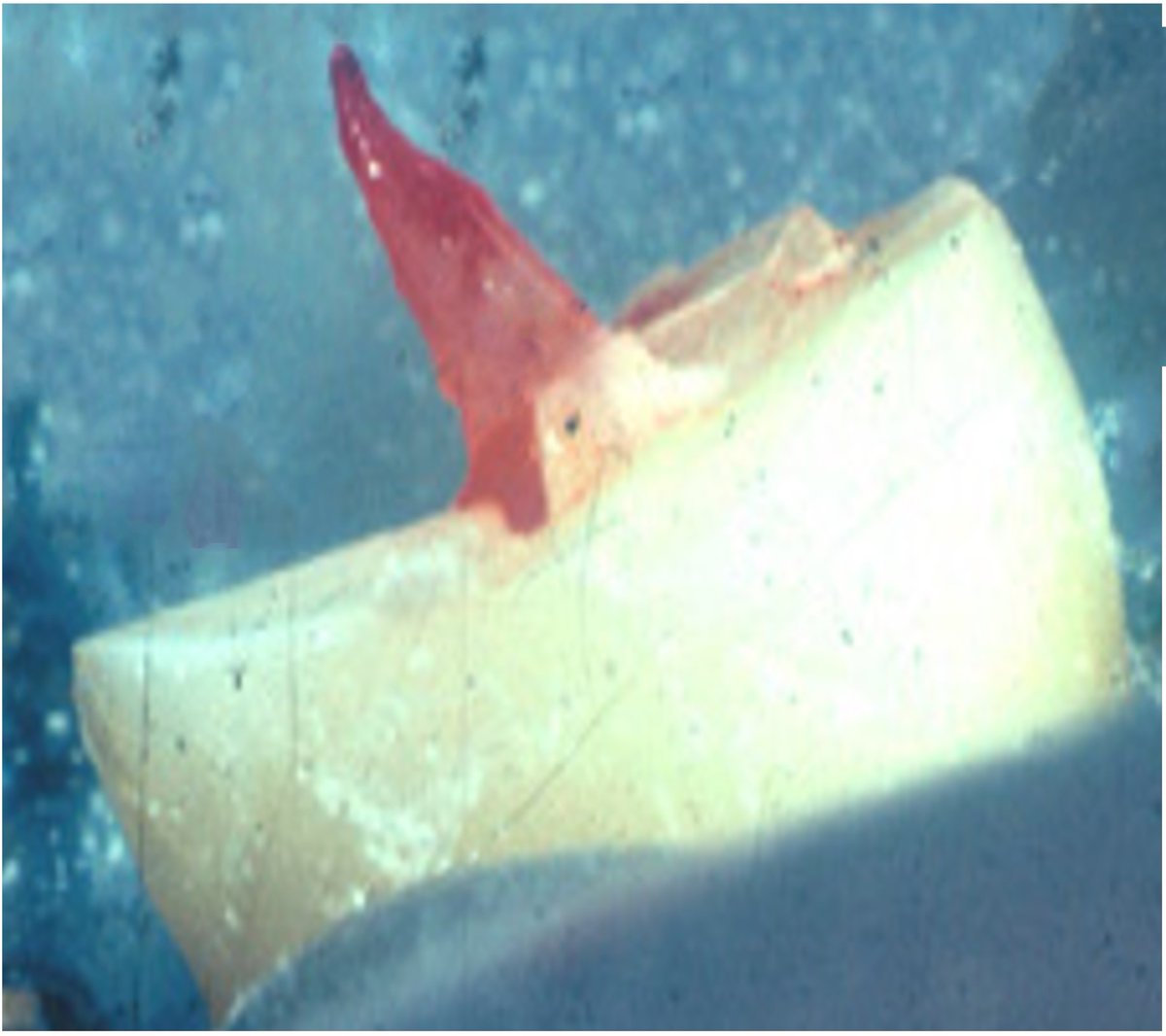












Tooth Structure Cracks: From Confusion to Clarity
Sixty Years After Cameron's Warning
Tooth structure cracks are now considered the third leading cause of tooth loss in dentistry.
More than 60 years ago, Cameron 1964 warned the dental profession about what he called Cracked Tooth Syndrome. Today, the problem has evolved into what many consider a silent epidemic.
Studies have reported cracks in 66.1% of molars, and more recent data suggest rates approaching 81%. Even more surprisingly, cracks are found in 40–60% of intact, unrestored posterior teeth.
Yet despite their prevalence, our attention is often directed toward the final stages of tooth crack failure:
• Root fractures
• Split teeth
• Cusp fractures
What if these conditions are not the beginning of the problem—but the end?
In this Master Class, I present a different perspective:
Most catastrophic tooth fractures begin as small, undetected line cracks that remain unnoticed until structural collapse.
The challenge is not simply finding cracks. The challenge is understanding:
• What is the crack?
• Why did it occur?
• How should it be diagnosed?
• What does it mean clinically?
To answer these questions, this Master Class introduces a structured diagnostic philosophy built around:
• The 3×3 Crack Classification
• The EROIC Etiologic Framework
• The 4ROD Diagnostic Protocol
• The ROTC Clinical Interpretation Method
• The MADA Concept for intact cracked teeth
The goal is simple:
Move beyond accidental discovery, symptom-based management, and reactive treatment.
Move from confusion to clarity.
Because before we can treat a crack, we must first understand it.
👉 Join now at abourass.com
1
3
212
Beyond Pulp Necrosis - The Many Faces of Pulp Degeneration - Bacterial Pulp Necrosis
For decades, pulp necrosis has been taught as a simple endpoint of bacterial infection.
But is the story really that simple?
In this new Master Class, we revisit the classic research of Sundqvist—the pioneering scientist whose work transformed our understanding of pulpal disease. His studies revealed that a necrotic pulp is not infected by a single microorganism, but by complex communities of anaerobic bacteria, with as many as 4–6 different species occupying a single root canal.
More importantly, Sundqvist helped establish the infection chain linking pulp exposure to apical periodontitis, laying the biological foundation for modern endodontics.
In this presentation, we explore:
• The bacterial pathway from pulp exposure to apical disease.
• The twelve recognized routes through which bacteria gain access to the pulp.
• The twelve causes of bacterial pulp death.
• The four major culprits responsible for most cases of bacterial pulp necrosis:
• Caries
• Periodontal disease
• Failed vital pulp therapy
• Tooth structure cracks
We also demonstrate how the 4R Operational Diagnosis Protocol can be applied to diagnose symptomatic and flared-up bacterial pulp necrosis in everyday clinical practice.
This Master Class is part of the larger series:
Beyond Pulp Necrosis: The Many Faces of Pulpal Degeneration
Because the future of endodontic diagnosis is not simply determining whether a pulp is vital or non-vital.
It is understanding why the pulp is dying, how it died, and what that means for treatment and prognosis.
👉 Join now at abourass.com
2
181
Beyond Pulp Necrosis – The Many Faces of Pulp Degeneration
For decades, we have taught dental students and practitioners that pulp necrosis follows a simple pathway:
Caries → Pulpitis → Pulp Necrosis → Apical Periodontitis.
But what if that story is incomplete?
What if pulp degeneration has many faces?
Throughout my clinical and academic career, I have observed that pulpal death is not always the result of bacterial infection. The pulp may undergo degeneration due to ischemia, calcification, atrophy, trauma, aging, and systemic influences that compromise its blood supply and vitality.
Not all pulps die the same way.
Not all necrosis follows the same biological pathway.
And not all roads to apical periodontitis begin with bacteria.
Understanding these differences is more than an academic exercise. It can profoundly influence diagnosis, treatment decisions, prognosis, and—most importantly—the prevention of apical periodontitis.
In the AbouRass Endodontics Academy Master Class:
Beyond Pulp Necrosis – The Many Faces of Pulp Degeneration
We explore the full biological journey of the dental pulp—from vitality to degeneration, from health to disease, and from traditional concepts to a broader clinical reality.
Sometimes the most important discoveries in dentistry begin by asking a simple question:
Have we been telling the whole story?
👉 Join now at abourass.com
4
567
THE STORY OF ENDODONTICS:
The Life, Memory, and Legacy of the Dental Pulp
For more than fifty years, I have never viewed the dental pulp as merely a collection of nerves, blood vessels, and connective tissue located inside a tooth.
The pulp is the protagonist of the endodontic story.
The pulp is the tooth’s memory organ.
A remarkable living organ.
An organ that nourishes.
An organ that protects.
An organ that senses danger.
An organ that repairs.
An organ that adapts.
And perhaps most importantly, an organ that remembers.
The dental pulp is the memory organ of the tooth.
Every restoration leaves a trace.
Every crack leaves a mark.
Every traumatic injury leaves evidence.
Every bacterial challenge leaves a scar.
The pulp never forgets.
Throughout life, it records its experiences through calcification, fibrosis, reparative dentin formation, inflammation, and countless other biological responses.
For years, sometimes decades, it quietly carries the burden of protecting the tooth.
It tolerates abuse.
It adapts to change.
It compensates for injury.
It struggles to survive.
Often, it does so silently.
This is why I introduced the concept of the Stressed Pulp Condition more than forty years ago.
The stressed pulp is not a diseased pulp.
It is a pulp attempting to survive.
It is a living organ responding to accumulated challenges that exceed its ability to adapt completely.
Eventually, however, there may come a point when the burden becomes greater than the pulp's capacity to cope.
The pulp begins to fail.
The pulp loses its ability to recover.
The pulp dies.
Yet death is not the end of the story.
In many ways, it is the beginning of the most important chapter.
A necrotic pulp demands respect.
When the cause of pulp death is ignored, and the root canal remains infected, the consequences extend far beyond the tooth itself.
Apical periodontitis develops.
In severe cases, the infection spreads, abscesses form, and affect the entire neighborhood around the tooth.
To understand endodontics, we must first understand the life, memory, and legacy of the dental pulp.
For more in-depth content on Endodontic diagnostics, visit the Abou-Rass Endodontics Academy: abourass.com
200
Over 40 Years of the Stressed Pulp: Why 1982 Still Dictates Modern Endodontic Reality.
In 1982, I published a diagnostic concept in The Journal of Prosthetic Dentistry that challenged the traditional, binary view of pulpal vitality: The Stressed Pulp Condition.
Every experienced general practitioner and veteran endodontist knows that a tooth is a living ledger. It stores the cumulative, silent trauma of deep restorations, crown preparations, micro-leakage, and functional stress over a patient's lifetime. A pulp that tests "vital" on a routine cold test today is not guaranteed to be a healthy organ tomorrow; often, it is a deeply compromised entity, silently marching toward a catastrophic breaking point.
Quality dentistry cannot be summarized in short snippets or modern social media feeds. It requires deep clinical observation, historical perspective, and a commitment to comprehensive diagnostic standards. Forty-four years later, this concept remains as vital to predictable treatment planning as the day it was written.
Are we treating the tooth we see today, or the lifelong history written inside it?
Reference:
Abou-Rass M. The stressed pulp condition: An endodontic-restorative diagnostic concept. J Prosthet Dent. 1982 Sep;48(3):264-271.
For more in-depth content on Endodontic diagnostics, visit the Abou-Rass Endodontics Academy: abourass.com
179
How Apical Periodontitis Diagnosis Ended the Histologic Terminology Chaos
For decades, dentists have been taught to describe periapical radiolucencies using histologic terms such as granuloma, a true cyst, a pocket cyst, apical lesion, apical radiolucency, and abscess.
But have you ever asked yourself:
Can you truly diagnose a cyst or granuloma from a radiograph alone?
More importantly—
Does calling a lesion a cyst instead of a granuloma change the treatment plan?
In most cases, the answer is no.
A tooth with inadequate endodontic treatment and an 8-15 mm periapical radiolucency remains an endodontic disease requiring appropriate management, regardless of the histologic label attached to it.
Over the past 60 years, pioneering research by Kakehashi, Bergenholtz, Orstavik, Sundqvist, Segura-Egea, Brynolf, Nair, Estrela, and others has demonstrated that radiographic findings—not speculative histologic terminology—provide the foundation for clinical diagnosis, classification, treatment planning, and outcome assessment.
Yet many textbooks, schools, examination boards, and organizations continue to rely on terminology that often creates confusion rather than clinical clarity.
In this presentation, I discuss:
• How apical periodontitis diagnosis evolved from histologic speculation to radiographic evidence
• Why radiographic classification brought order to decades of terminology confusion
• The historical research that changed our understanding of periapical disease
• The need for clinically relevant, evidence-based classifications that improve diagnosis and treatment decisions
Understanding this evolution is essential for every dental student, general practitioner, and endodontist who wants to diagnose apical periodontitis with greater confidence and precision.
👉 Join now at abourass.com
3
338
The Untold Story Behind Apical Periodontitis – Endodontics’ Most Common Pathology
Today, when a dentist sees a radiolucency around the root of a tooth with pulp necrosis or inadequate endodontic treatment, the diagnosis is usually straightforward:
Apical Periodontitis (AP).
But did you know it took nearly 50 years of controversy, confusion, research, and scientific debate for dentistry to reach this conclusion?
The story behind AP—the most common pathology in endodontics—is rarely taught in dental schools.
For decades, endodontic periapical radiolucencies were misunderstood, misclassified, and described by a variety of histological terms that often created more confusion than clarity. The profession moved through multiple historical eras before finally recognizing these lesions as manifestations of a single disease process: Apical Periodontitis.
In this presentation, I review the six historical eras that shaped our current understanding of AP:
• Pools of Sepsis Era
• Stagnation Lesions Era
• Sterile Granuloma Era
• Microbial AP Era
• Molecular AP Era
• AP Awareness Era
Understanding this history is important because it explains why terminology, diagnosis, treatment philosophies, and educational approaches have been so inconsistent over the years.
Today, AP has become the universal diagnostic term encompassing the major periapical pathologies of endodontic origin, including granulomas, cysts, abscesses, and condensing osteitis.
To understand where endodontics is going, we must first understand how we arrived here.
👉 Join now at abourass.com
2
310
Modern Dentistry Is No Longer Practiced By One Doctor In One Room.
Today, dentistry is delivered through large clinics, DSOs, hospital departments, and multi-doctor practices where clinicians come from different educational systems, philosophies, and clinical backgrounds.
The result?
Inconsistency in diagnosis.
Variations in treatment planning.
Missed findings.
And, ultimately, compromised patient care.
That reality is one of the reasons I developed the AbouRass 4R Operational Diagnosis Protocol (4ROD).
This protocol was not created overnight.
It evolved through more than four decades of teaching, clinical practice, observation, research, and continuous refinement in Pittsburgh, Los Angeles, Saudi Arabia, and beyond.
The philosophy is simple:
Dentistry should move from speculation to operational verification.
Instead of merely looking and assuming…
we investigate, verify, explore, document, and confirm.
The 4ROD framework provides clinicians with a structured, evidence-based diagnostic language that can be used consistently across individual practices, teaching institutions, hospitals, and large group clinics.
The protocol includes:
• R1 — Rapport & Reports
Understanding the patient beyond the chief complaint using the Patient Pain Profile (PPP).
• R2 — Radiographic Findings
The 10 Areas of Diagnostic Interest (10 ADI) for systematic radiographic interpretation.
• R3 — Pulp & Periodontal Testing
Structured operational testing using biologically meaningful clinical methods.
• R4 — Restoration & Tooth Integrity Evaluation
Applying restorative and structural assessment standards to determine restorability and prognosis.
The 4ROD is not simply a checklist.
It is not merely a philosophy.
It is an operational diagnostic framework designed to improve clarity, communication, consistency, and patient safety in modern dental practice.
👉 Join now at abourass.com
1
167
Apical Periodontitis: 52% Global Prevalence and Rising
For over five decades—first at the and later at—I witnessed the same troubling clinical reality:
Patients living for years with large, established apical periodontitis lesions…
Undiagnosed.
Untreated.
Misunderstood.
Even more disturbing was hearing:
“My dentist is watching it.”
Today, apical periodontitis (AP) has reached an alarming global prevalence of nearly 52%—making it one of dentistry’s most neglected and silent epidemics.
Why has this happened?
Because AP has not been taught with the clinical depth, biological understanding, and diagnostic precision it truly deserves.
That is why I created:
“Apical Periodontitis – The Neglected Endodontic Epidemic.”
This comprehensive educational journey includes 3 detailed presentations exploring:
• What AP really is
• Why patients should worry about it
• The true causes of AP
• How AP behaves clinically as a disease
• Why current classifications need enhancement
• ARSAP: My Radiolucency Size–Based AP Classification for diagnosis and treatment planning
This Master Class is designed for every general practitioner and specialist who wants a deeper, biologically driven understanding of the most important endodontic disease impacting patients today.
The goal is simple:
To elevate patient care through better endodontic diagnosis, timely intervention, and prevention of apical periodontitis.
👉 Join now at abourass.com
1
213
4ROD Final Introduction: Developmental Dental Anomalies, Early Diagnosis & the Power of Structured Endodontic Thinking
The final introduction in the 4ROD Masterclass Series has now been released.
This presentation concludes the R4 stage of the 4R Operational Diagnosis Protocol, focusing on three clinically important developmental dental anomalies:
• Palatogingival Groove (PGG)
• Dens Invaginatus (DI)
• Dens Evaginatus (DE)
Although uncommon, these anomalies are highly significant in endodontic and periodontic practice because they frequently affect teeth in the esthetic zone and may remain silent for years before presenting as advanced, complex disease.
When symptoms finally appear, clinicians are often facing:
• Advanced pulpal and periapical pathology
• Localized periodontal destruction
• Difficult treatment decisions
• Multidisciplinary management
• Unpredictable prognosis
In this presentation, these anomalies are profiled through the complete 4ROD framework:
• Patient report and history
• Radiographic interpretation
• Pulp and periodontal testing
• Tooth structure and restorative findings
The session includes:
• The Gu classification of PGG
• The classic Oehlers classification of DI
• Clinical implications and classifications of DE
• Periapical radiographs and CBCT interpretation
• Published benchmark cases from around the world
• Personal clinical experiences and rare combined anomaly cases
One remarkable case involved both DI and DE occurring in the same tooth—demonstrating the true complexity of diagnosis and treatment planning in advanced endodontics.
Most importantly, this presentation reinforces the central message of the entire 4ROD philosophy:
Early recognition prevents advanced disease.
By applying a structured diagnostic framework such as 4ROD, clinicians can identify hidden pathology earlier, improve decision-making, reduce complications, and provide more predictable biologic and restorative outcomes for patients.
This concludes the 4ROD introduction series—but it also marks the beginning of a deeper diagnostic journey beyond traditional endodontics.
👉 Join now at abourass.com
1
396
From Abfraction to NCCL: Endodontic Implications and Clinical Management
What was once called “abfraction” is no longer viewed as a simple stress-induced cervical defect.
Today, these lesions are understood as NCCLs — Non-Carious Cervical Lesions — a complex, multifactorial condition involving biomechanical stress, flexure, occlusal forces, dentin biology, and breakdown of tooth structure at the cemento-enamel junction.
In this new presentation from the AbouRass Endodontics Academy, we explore the modern understanding of NCCLs from both restorative and endodontic perspectives.
This presentation discusses:
• The evolution from the old “abfraction” concept to the broader NCCL classification
• The clinical stages and patterns of NCCLs
• Compression, tensile stress, flexure, and multifactorial pathodynamic theories
• Anatomical variations at the enamel-cementum junction
• Dentin permeability and hypersensitivity
• The relationship between NCCLs, pulpal health, cracks, and long-term tooth survival
From an endodontic perspective, NCCLs are highly significant.
When these teeth require root canal treatment, traditional aggressive approaches may further weaken the cervical zone and increase the risk of fracture.
For this reason, I utilize the BioSeal Stress-Free Root Canal Treatment Protocol, designed to preserve cervical dentin and minimize biomechanical stress through:
• Conservative access preparation
• Stress-modulated canal shaping
• Stress-free obturation techniques
• Fiber-reinforced composite reinforcement
The goal is not only to treat the tooth…
but to preserve its long-term structural and biologic integrity.
NCCLs are not simply cervical defects.
They are biological and biomechanical warning signs that demand precise diagnosis and thoughtful clinical management.
👉 Join now at abourass.com
2
326
على مدى السنوات قرأت و سمعت الكثير من الرسائل عن الصمود، وخيبات الأمل، والاعتماد على النفس، والإيمان. لكن عندما استمعت إلى ما عبّر عنه الأستاذ عبدالسلام الحبابي بهذه الصورة الجميلة والبليغة في هذا المقطع باللغة العربية، شعرت فعلًا بقشعريرة تسري في جسدي.
الرسالة قوية، عميقة المشاعر، وتزداد تأثيرًا وروعة عندما تُقال بلغتنا العربية الجميلة.
وفي جوانب كثيرة، شعرت وكأنها تحكي قصة رحلتي الشخصية في التعليم، والحياة، والصراع المهني — أن تتعلم، أحيانًا بالطريقة الصعبة، كيف تبتعد عن البيئات التي لا تُقدّرك أو لا تدعمك، وأن تضع ثقتك في نفسك، وفي رسالتك، وفي الله سبحانه وتعالى.
هذه الرسالة تتجاوز كثيرًا حدود طب الأسنان أو علاج الجذور. لذلك أحببت أن أشاركها مع المتابعين، والزملاء، والطلاب، والأصدقاء، لأنني أؤمن أن الكثيرين سيرون جزءًا من قصتهم الشخصية فيها أيضًا.
أرجو أن تمنحوها دقائق من وقتكم للاستماع.
tiktok.com/@sau.911/video/76…
232
Throughout the years, I have heard many messages about resilience, disappointment, self-reliance, and faith. But when I listened to what Mr. Abdulsalam Al Habaibi so beautifully and eloquently expressed in this Arabic TikTok presentation, it truly made me shiver.
The message is powerful, deeply emotional, and even more moving in our beautiful Arabic language.
In many ways, it feels like the story of my own journey in education, life, and professional struggle — learning, often the hard way, to walk away from environments that do not value or support you, and to place your trust in yourself, your mission, and in Allah.
This message goes far beyond endodontics. I wanted to share it with my followers, colleagues, students, and friends because I believe many people will see part of their own story in it as well.
Please take a moment to listen.
Thank you, Abdulsalam, for a beautiful material. You are the best I have heard.
tiktok.com/@sau.911/video/76…
114
Attritive Tooth Wear – Endodontic Perspective & Clinical Management
Today, we are releasing the introduction to our presentation on attritive tooth wear — a common yet often underestimated condition with major biological, functional, occlusal, and endodontic implications.
Attrition is not simply “normal wear.”
It is a biomechanical process driven by occlusal stress, parafunction, grinding, clenching, and abnormal tooth contact. Over time, this mechanical destruction can compromise tooth structure, pulpal health, occlusal stability, and ultimately the patient’s quality of life.
This presentation explores:
• The difference between attrition, erosion, and abrasion
• Clinical and radiographic signs of attritive wear
• The relationship between bruxism, occlusal overload, and pulpal stress
• Pulpal responses, including dentinal bacterial invasion, pulpal atrophy, and pulpal necrosis
• Occlusal collapse, posterior super-eruption, and loss of vertical dimension
• The connection between severe attrition and temporomandibular disorders (TMDs)
• Why are severely worn dentitions highly susceptible to fractures and apical periodontitis (AP)
The presentation also reviews the evolution of treatment philosophy:
From the traditional full-mouth rehabilitation approach of the 1980s and 1990s to today’s modern conservative additive prosthodontic concepts, inspired by the work of Dr. Vailati.
This presentation further integrates attrition into the 4ROD diagnostic philosophy, emphasizing the importance of recognizing wear patterns as biological and functional warning signs—not merely cosmetic or mechanical changes.
Attrition is a silent, destructive process.
Early diagnosis and conservative intervention are essential to preserving pulp vitality, maintaining occlusal stability, and improving long-term prognosis.
👉 Join us at abourass.com
1
150
Tooth Wear Is Not Just Cosmetic — It Is Biological, Functional, and Endodontic
Erosive Tooth Wear has become a growing global problem affecting both developing and developed countries. Far beyond aesthetics, it is now recognized as a serious biological and functional disease process with major restorative, occlusal, and endodontic implications.
This presentation explores erosive wear from an endodontic and interdisciplinary clinical perspective, emphasizing its relationship to oral pain, dentinal exposure, tooth fractures, occlusal instability, TMJ dysfunction, pulpal degeneration, and diminished Oral Health-Related Quality of Life (OHRQoL).
Erosive tooth wear is strongly associated with modern lifestyle and systemic health factors, including:
• Acidic diets and unhealthy lifestyle habits
• Reduced salivary flow and dehydration
• Gastroesophageal Reflux Disease (GERD)
• Chronic vomiting and eating disorders
• Alcoholism and systemic health disturbances
The prevalence continues to rise dramatically worldwide, particularly among adolescents and young adults.
From an endodontic standpoint, erosive wear may lead to:
• Loss of enamel and secondary dentin
• Dentinal exposure and sensitivity
• Tertiary dentin formation
• Pulp chamber calcification and atrophy
• Stressed pulp conditions
• Pulpitis and non-bacterial pulp necrosis
This presentation also introduces the Vailati & Belser (2007) classification and discusses modern management concepts, particularly additive prosthodontics as a conservative, biologically driven alternative to aggressive full-mouth rehabilitation.
Key Topics Include:
• Erosive Tooth Wear and Oral-Systemic Health
• Lifestyle and Medical Risk Factors
• Endodontic Implications of Tooth Wear
• Pulpal and Dentinal Changes
• Occlusal and Functional Consequences
• Vailati & Belser Classification
• Additive Prosthodontics and Conservative Management
This presentation is part of the AbouRass Endodontics Academy educational series focused on biologically driven diagnosis and interdisciplinary clinical decision-making.
📷 Join the Academy at AbouRass.com
3
377
From Diagnosis to Mastery: The 4ROD Protocol Meets the Cracked Tooth Epidemic
Today marks an important milestone.
We are releasing the introduction to the Comprehensive Presentation on Tooth Structure Cracks as a part of R4 of the 4ROD Operational Diagnosis Protocol—a structured, clinically driven system designed to move endodontic and related disciplines diagnostics from uncertainty to definitive diagnosis.
But this is not a theory. This system is already in action.
Recently, we launched the Master Class in Tooth Structure Cracks—a comprehensive 17-presentation series that addresses one of the most misunderstood and misdiagnosed problems in clinical dentistry.
Cracked teeth are the third leading cause of tooth loss—yet they remain a diagnostic challenge.
Why?
Because most clinicians are still relying on fragmented thinking, isolated tests, and incomplete evaluation methods.
This is exactly where 4ROD becomes essential.
Through:
• R1 – Patient encounter and behavioral insight
• R2 – Radiographic interpretation (10 ADI)
• R3 – Evidence-based response testing
• R4 – Restorative and tooth structure analysis
…we create a complete diagnostic architecture.
The Tooth Cracks Masterclass is not just a course—it is a clinical demonstration of how this system works in real life.
From line cracks… to fissures… to fractures…
From confusion… to clarity. It is seeing clearly, systematically, and predictably.
This is not content.
This is a new way of thinking.
👉 Join now at abourass.com
1
436
Beyond Aesthetics: The Endodontic Meaning of Tooth Discoloration
Today, I am releasing Part 2 of R4 – Tooth Structure Assessment within the 4ROD Protocol.
We have already addressed restorations. Now, we move deeper into the tooth itself.
This presentation redefines tooth discoloration. It is not a cosmetic issue. It is a diagnostic message.
Every color change—yellowing, darkening, gray shadows, pink hues, or loss of translucency—represents a biological event occurring within the tooth. Tooth discoloration provides a non-invasive window into:
• Pulp health and degeneration
• Internal breakdown and necrosis
• Trauma and vascular changes
• Coronal leakage and restorative failure
These changes are often the earliest and sometimes the only clinical signs of underlying disease.
This presentation connects discoloration to its true causes, including:
• Caries and restorative leakage
• Advanced periodontitis
• Internal and external resorption
• Pulpal calcification and failed vital pulp therapy
• Luxation injuries and orthodontic forces
• Aggressive crown preparation and structural compromise
Most importantly, it teaches clinicians to think differently:
Every discoloration is a biological clue
Every color change deserves diagnostic attention
Even when the tooth is asymptomatic…
Even when radiographs are inconclusive…
This is R4 thinking—where structure, biology, and restoration come together in one unified diagnosis.
Key Learning Points:
• Color as a reflection of pulp biology
• Discoloration as an early warning sign
• Structural and restorative sources
• Radiographic correlation with color patterns
• Role of discoloration in patient communication and treatment acceptance
This is not about aesthetics.
This is about seeing disease before it becomes pain.
👉 Join the Academy: abourass.com
6
625
Beyond Beauty: The Biologic Diagnostic Power of Aesthetic Criteria in Modern Restorative Dentistry
The 2023 FDI Restoration Criteria: Aesthetic Component - goes far beyond appearance.
This presentation challenges the traditional view of aesthetics as “cosmetic” and reframes it as a powerful biologic diagnostic tool within the R4 (Restorative & Tooth Structure) step of the 4ROD protocol.
What appears as a simple aesthetic defect, discoloration, loss of translucency, marginal shadowing, staining, or contour distortion, is often the first visible sign of deeper biological and structural breakdown.
These changes may reflect:
• Microleakage and bacterial penetration
• Recurrent caries and marginal failure
• Material aging and degradation
• Occlusal stress pathways
• Early crack formation and structural fatigue
In this presentation, aesthetic evaluation becomes a clinical language, one that reveals hidden pathology before symptoms arise.
You will learn:
• How aesthetic criteria serve as early biological warning signs
• The key 2023 FDI aesthetic parameters and how to interpret them clinically
• The diagnostic meaning behind color mismatch, staining, and translucency changes
• The significance of surface texture, contour, and marginal shadow lines
• How aesthetic changes correlate with radiographic findings
• Why aesthetic evaluation is essential in predicting endodontic risk
This is not about beauty.
This is about seeing disease before it declares itself.
Aesthetic criteria, when properly understood, complete the triad of Functional, Biological, and Aesthetic evaluation, transforming R4 into a true diagnostic powerhouse.
👉 Join now: abourass.com
2
256
FDI Biological Criteria: The Hidden Threat Behind “Acceptable” Restorations
Not all restorations fail visibly. Some fail biologically, quietly and progressively.
The 2023 FDI Biological Criteria shift our focus from what looks acceptable to what is biologically happening beneath the surface.
In this 4-minute introduction, I present one of the most important yet overlooked components of R4 – Restorative and Tooth Structure Assessment in the 4ROD protocol. Because restorations are not just mechanical structures, they are biologically connected. A restoration can either protect the pulp or slowly destroy it.
These universal, internationally accepted criteria help clinicians detect early biological warning signs that are often missed:
• Microleakage beneath intact margins
• Plaque retention and gingival inflammation
• Recurrent caries hidden under restorations
• Material toxicity and tissue irritation
• Postoperative hypersensitivity
• Early pulpal stress before radiographic changes
This is not just a restorative evaluation. This is an endodontic risk assessment at its earliest stage. When properly applied, the FDI Biological Criteria become a predictive diagnostic tool
allowing clinicians to identify future pulp disease and apical periodontitis before they occur.
In this presentation, we cover:
• Why is a biological evaluation essential for endodontic diagnosis
• The core biological criteria of the FDI system
• The link between restorations and pulp degeneration
• Radiographic recognition of biological defects
• Integrating biological thinking into R4 clinical decision-making
• Communicating risk and treatment with patients
👉 Join the full masterclass: abourass.com
1
437