
26 y/o | MBBS (Gold Medalist)(PMC'23)🏅 | Dip. Card (UK); Dip. Diab (UK)🇬🇧 | MRCP (UK)-II 🩺 | 16 Int'l Publications📝 | Int'l Teacher🎓 | B. Sc. 📚 | RMP
Joined January 2021
- Tweets 13,530
- Following 979
- Followers 1,780
- Likes 13,528
3,316 Photos and videos











Pinned Tweet
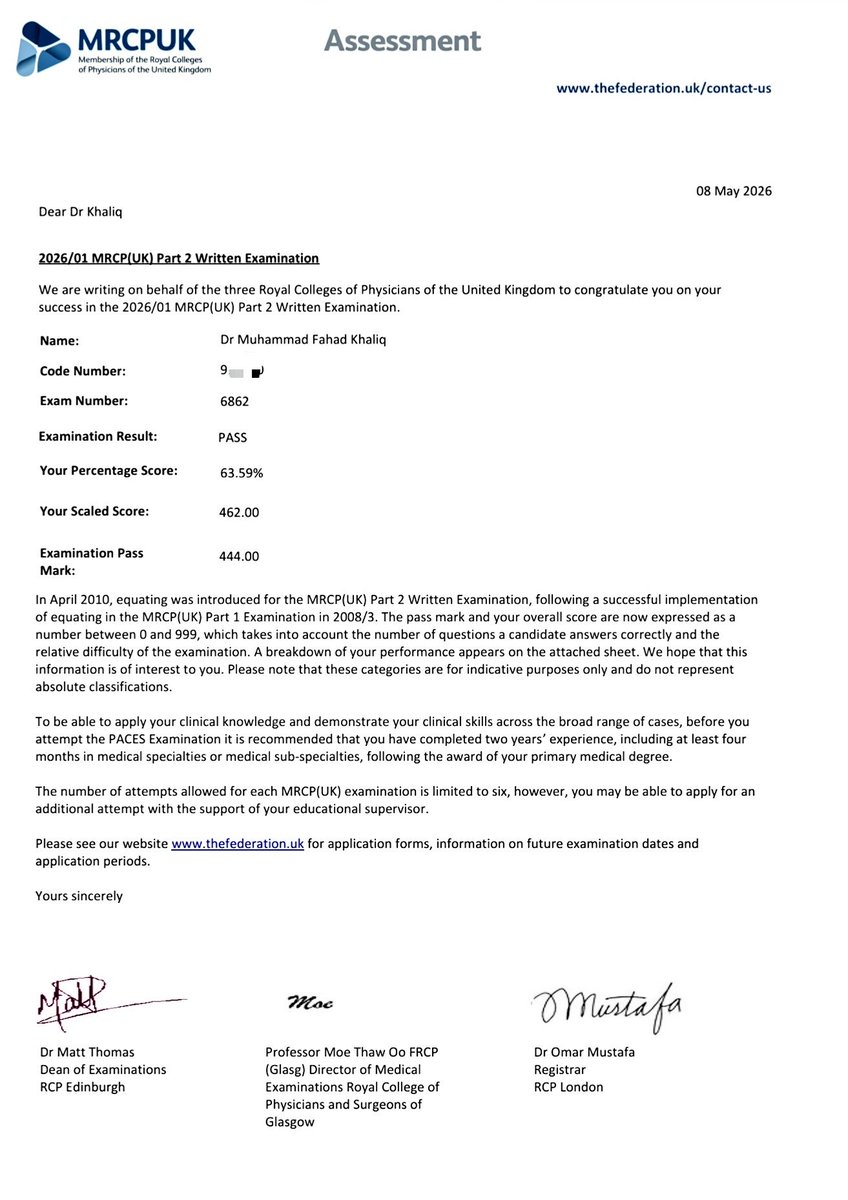
By the grace of Allah Almighty, here’s another step towards my dream and fav fav consultantship qualification:
𝗠𝗲𝗺𝗯𝗲𝗿𝘀𝗵𝗶𝗽 𝗼𝗳 𝘁𝗵𝗲 𝗥𝗼𝘆𝗮𝗹 𝗖𝗼𝗹𝗹𝗲𝗴𝗲 𝗼𝗳 𝗣𝗵𝘆𝘀𝗶𝗰𝗶𝗮𝗻𝘀 𝗼𝗳 𝘁𝗵𝗲 𝗨𝗻𝗶𝘁𝗲𝗱 𝗞𝗶𝗻𝗴𝗱𝗼𝗺 𝗣𝗮𝗿𝘁 𝗜𝗜 — 𝗣𝗔𝗦𝗦𝗘𝗗! 💫
Within just 1 year of completing the house job, and at the age of 26, I’ve achieved far far more than I ever imagined:
Certified Cardiologist (UK) ✅
Certified Diabetologist (UK) ✅
And "Almost" a Consultant Physician 🔥
Dr. Muhammad Fahad Khaliq
MBBS Gold Medalist (PMC)
MRCP (UK)—II, Dip. Card (UK)
Dip. Diab (UK), B. Sc. (Eng.), RMP
26
1
125
4,934

Jun 15
Attendant at 2: 00 AM after I spent hours stabilizing a crashing patient in ER: Wadday dactar sbb ne kaddoun aana?
My mind: ** Mera bhai aadhi raat ko teri farmaish pr toh wo anay nai wala. ER ki bajaye seedha uske ghar chala jata toh shyd mulaqaat hojati lakin filhal tujhy abhi sirf mere sth hi guzara krna prna hai **
Me: Kal subah ayen gay 🤗
1
6
332
Jun 10
Aortic Stenosis (AS) causes "pulsus parvus et tardus" which means a "Low-volume, slow-rising pulse"
However, this finding may NOT always be apparent in elderly patients because age-related arterial stiffening can mask the characteristic pulse changes.
Another important distinction should be made between aortic STENOSIS and aortic SCLEROSIS.
BOTH can produce an ejection systolic murmur, but the additional clinical features help differentiate them (which are present in STENOSIS and NOT in SCLEROSIS):
1) Slow-rising, low-volume pulse (pulsus parvus et tardus)
2) Narrow pulse pressure
3) Heaving apex beat (LVH)
4) Systolic thrill
5) Soft or absent A2
6) Ejection systolic murmur
Risk factors such as DM, smoking, HTN, and hyperlipidemia accelerate the progression of aortic SCLEROSIS and increase the likelihood of developing clinically significant aortic STENOSIS
P.S. Every LOW VOLUME PULSE is NOT always AS!
Keep other differentials like Shock, MS, Chronic constrictive pericarditis, Pulmonary HTN and Pericardial Effusion in the back of your mind as well
2
125
The Fallot Brothers:
Trilogy of Fallot: ASD with PS with right ventricular hypertrophy
Tetrology of Fallot: VSD with PS with right ventricular hypertrophy and overriding aorta
Pentalogy of Fallot: When TOF is associated with ASD
Acyanotic TOF (Pink Fallot): When TOF is associated with infundibular PS (The outflow obstruction is mild without obvious cyanosis)
TOF with pulmonary atresia = Severe form with duct-dependent pulmonary blood flow
4
230
May 31
Your side chick looking into your heart realizing she's the dragon warrior
Skadooossshhhhh! 💥
2
168
May 27
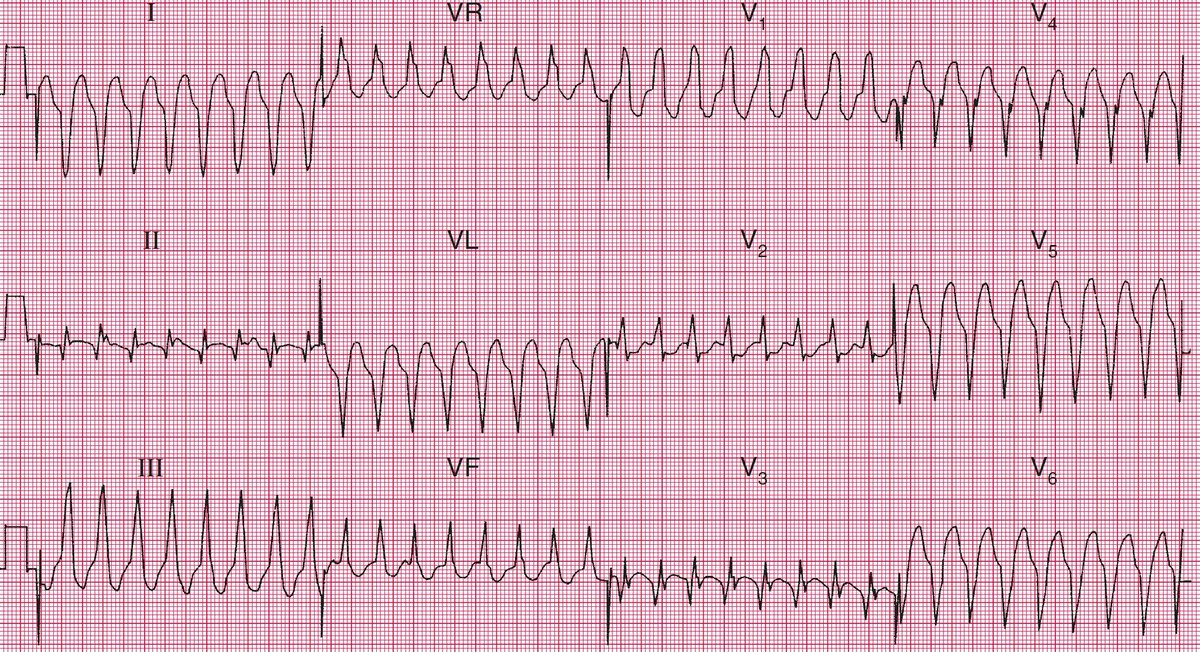
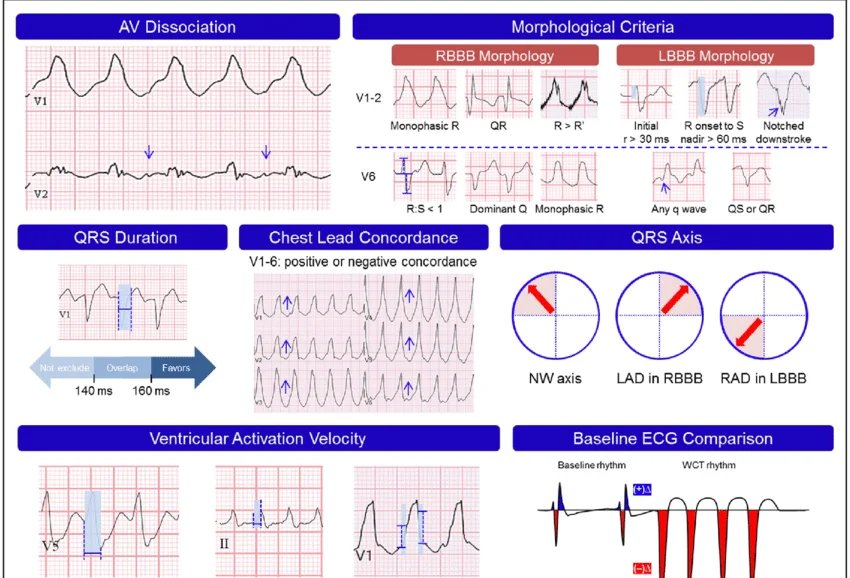
𝗔𝗻 𝗮𝗽𝗽𝗿𝗼𝗮𝗰𝗵 𝘁𝗼 𝗕𝗿𝗼𝗮𝗱 𝗰𝗼𝗺𝗽𝗹𝗲𝘅 𝘁𝗮𝗰𝗵𝘆𝗰𝗮𝗿𝗱𝗶𝗮 (BCT) 𝗼𝗳 𝘂𝗻𝗰𝗲𝗿𝘁𝗮𝗶𝗻 𝗼𝗿𝗶𝗴𝗶𝗻
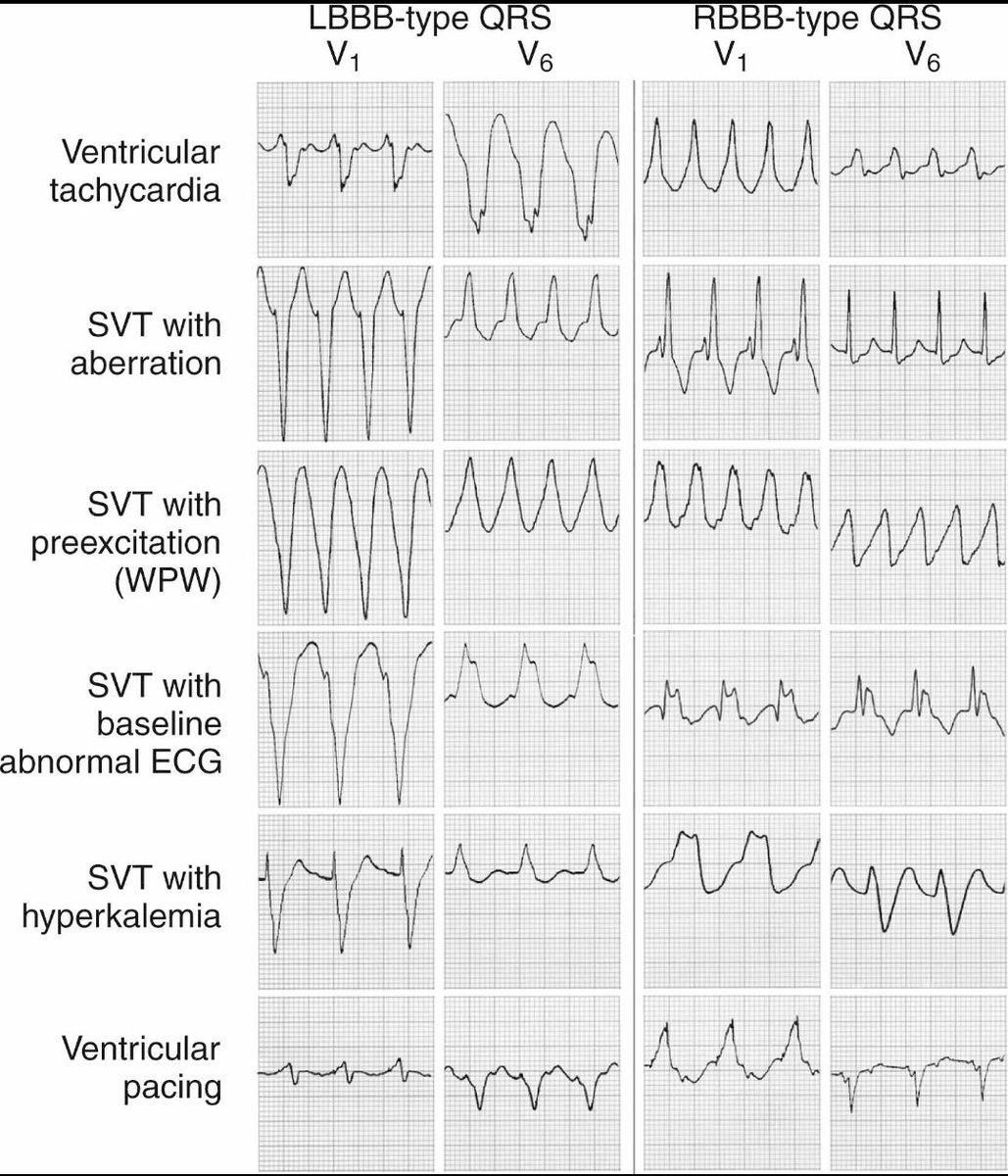
Main 𝐝𝐢𝐟𝐟𝐞𝐫𝐞𝐧𝐭𝐢𝐚𝐥𝐬 for BCT include:
• 𝐕𝐓 (most common) = Regular broad bizarre QRS
• 𝐒𝐕𝐓 𝐰𝐢𝐭𝐡 𝐚𝐛𝐞𝐫𝐫𝐚𝐧𝐜𝐲 (𝐑𝐁𝐁𝐁/𝐋𝐁𝐁𝐁) = Typical BBB morphology (classic RBBB/LBBB pattern)
• 𝐒𝐕𝐓 𝐰𝐢𝐭𝐡 𝐖𝐏𝐖 = Pre-excited bizarre, wide QRS, not necessarily BBB pattern
• 𝐀𝐅 𝐰𝐢𝐭𝐡 𝐖𝐏𝐖 = Irregularly irregular varying bizarre wide QRS
• 𝐏𝐨𝐥𝐲𝐦𝐨𝐫𝐩𝐡𝐢𝐜 𝐕𝐓/𝐭𝐨𝐫𝐬𝐚𝐝𝐞𝐬 = Polymorphic twisting QRS
Based on the pattern of attached ECG: AF with WPW, Torsades, and SVT with WPW are instantly ruled out. This leaves us to the 2 main strong differentials:
"𝗩𝗧" 𝘃𝘀 "𝗦𝗩𝗧 𝘄𝗶𝘁𝗵 𝗔𝗯𝗲𝗿𝗿𝗮𝗻𝗰𝘆"
Which one to pick?
Before jumping straight to diagnosis, recall that 𝘁𝗵𝗲 𝗳𝗮𝗰𝘁𝗼𝗿𝘀 𝘁𝗵𝗮𝘁 𝗳𝗮𝘃𝗼𝗿 𝗩𝗧 𝗼𝘃𝗲𝗿 𝗦𝗩𝗧 𝗮𝗿𝗲:
• QRS “broader than simply broad one” (>160ms)
• AV dissociation (P and QRS complexes occur independently)
• Absence of typical LBBB or RBBB
• Capture beats
• Fusion beats
• Josephson’s sign
• Brugada’s sign
• Bunny with LEFT ear taller than right one (i.e. RSR’ with R>R’)
• Positive (or negative) concordance throughout chest leads
• Extreme axis deviation
• PLUS points: Age 35 yr , Hx of IHD/SCD/DCM/CHF
The rule is: 𝗔 𝘀𝘁𝗮𝗯𝗹𝗲 𝗯𝗿𝗼𝗮𝗱-𝗰𝗼𝗺𝗽𝗹𝗲𝘅 𝘁𝗮𝗰𝗵𝘆𝗰𝗮𝗿𝗱𝗶𝗮 𝘄𝗶𝘁𝗵 𝗽𝗼𝘀𝘀𝗶𝗯𝗹𝗲 𝗶𝘀𝗰𝗵𝗲𝗺𝗶𝗮 𝗶𝘀 𝗺𝗮𝗻𝗮𝗴𝗲𝗱 𝘃𝗲𝗿𝘆 𝗰𝗮𝘂𝘁𝗶𝗼𝘂𝘀𝗹𝘆 𝗮𝘀 𝗩𝗧. 𝗔𝘀𝘀𝘂𝗺𝗲 𝗩𝗧 𝘂𝗻𝗹𝗲𝘀𝘀 𝗽𝗿𝗼𝘃𝗲𝗻 𝗼𝘁𝗵𝗲𝗿𝘄𝗶𝘀𝗲
In the attached ECG of Broad complex tachycardia (BCT) of uncertain origin, the factors that 𝐟𝐚𝐯𝐨𝐫 VT are:
• QRS “broader than simply broad one” (>160ms)
• Bunny with LEFT ear taller than right one (i.e. RSR’ with R>R’)
• PLUS points: Age 35 and Hx of IHD
The factors that 𝐠𝐨 𝐚𝐠𝐚𝐢𝐧𝐬𝐭 the VT are:
• Right axis deviation (extreme axis deviation NOT present)
• ABSENCE of Positive (or negative) concordance throughout chest leads
This leaves us to VT and the 𝐦𝐚𝐧𝐚𝐠𝐞𝐦𝐞𝐧𝐭 is quite simple:
• 𝐏𝐮𝐥𝐬𝐞𝐥𝐞𝐬𝐬 𝐕𝐓: Defibrillation ACLS
• 𝐔𝐧𝐬𝐭𝐚𝐛𝐥𝐞 𝐦𝐨𝐧𝐨𝐦𝐨𝐫𝐩𝐡𝐢𝐜 𝐕𝐓 𝐰𝐢𝐭𝐡 𝐩𝐮𝐥𝐬𝐞: Synchronized cardioversion
• 𝐔𝐧𝐬𝐭𝐚𝐛𝐥𝐞 𝐏𝐨𝐥𝐲𝐦𝐨𝐫𝐩𝐡𝐢𝐜 𝐕𝐓: Defibrillation (unsynchronized)
• 𝐒𝐭𝐚𝐛𝐥𝐞 𝐦𝐨𝐧𝐨𝐦𝐨𝐫𝐩𝐡𝐢𝐜 𝐕𝐓: Procainamide (often preferred), amiodarone 150 mg IV over 10 min then infusion, or lidocaine (especially ischemic/post-MI VT)
*𝐁𝐲 𝐮𝐧𝐬𝐭𝐚𝐛𝐥𝐞 𝐈 𝐦𝐞𝐚𝐧𝐭: Hypotension, shock, chest pain, pulmonary edema, heart failure, AMS—almost every messed up finding excluding pulse!
𝐀𝐧𝐨𝐭𝐡𝐞𝐫 𝐢𝐦𝐩 𝐩𝐨𝐢𝐧𝐭 𝐢𝐬: VT is NOT ALWAY RELATED TO DEFIBRILLATION. A VT may require either synchronized cardioversion or defibrillation depending on rhythm type and pulse status. Loser, go read previous paragraph again!
Follow for more
1
9
43
2,202
May 25
How to present a case?
"Local" vs "International" Rules ~ A thread (for comparison)
Local/Undergraduate:
"A Young man, who is healthy built and well nourished, lying comfortably in the bed, fully conscious, well oriented in person, space and time, fully cooperative throughout the examination, with attached cannula 22G at left arm and with the cardiac monitor placed beside the bed with the vitals..."...And that's Bullsh*t!
Your presentation should sound like a doctor discussing a patient, NOT a student reciting a list of irrelevant examination steps only
A better way (Internationally accepted) can be:
"Miss Roberts is a young lady with focal, left sided cerebellar signs as evidenced by hypotonia and past pointing in the left arm. I also noted..."
HERE'S THE BREAKDOWN:
· Opening sentence should immediately state diagnosis/differential/localization/syndrome
· Start with patient’s name/title, NOT “he/she/the patient.” If forgot, use “This lady/gentleman”
· Do not start with irrelevant appearance statements.
· First sentence must show interpretation, NOT just findings.
· Mention key positive findings first.
· Mention only diagnostically important negative findings.
· Group findings logically by syndrome/system.
· Support your diagnosis with 2–3 strongest signs.
· Use phrases like “consistent with,” “suggestive of,” “evidence of.”
· Avoid listing findings in examination order mechanically.
· Mention severity if identifiable clinically.
· Mention complications if present.
· Tailor differentials to patient demographics and findings.
· Give short prioritized differentials only.
· Continuously interpret findings while presenting.
· Sound concise, confident, and consultant-like.
· Avoid uncertainty fillers (“maybe,” “possibly,” “sort of”).
· Do not mention omissions or forgotten steps.
· Finish with further examination/investigations if appropriate.
· Aim to “interpret findings,” not “narrate examination.”
Follow for more 📚🖋️
Dr. M. Fahad Khaliq
MBBS (Gold Medalist)(PMC '23)
MRCP (UK)-II, Dip. Card (UK)
Dip. Diab (UK), B. Sc., RMP
2
1
34
1,681
May 24
I don’t know if I should share this, but it has been weighing heavily on my heart since my last duty
Today, I attended this CKD/ESRD patient (who was scheduled for the dialysis) at the ER for the almost 7th time in 3 months. No response to diuretics, No dialysis machines available, barely hanging on—and only God knows how every time I somehow manage to pull him through with whatever we had available.
A patient with lungs completely choked up with fluid—unconscious from severe breathlessness, gasping and starving for air, with skyrocketing blood pressure and a severely disturbed metabolic profile.
Today, for a moment, I looked at his children—who are around my age—and thought how fortunate they are to still have many chances to bring their father back home alive again and again. And just like the previous 6 times, today, he survived again! (MashAllah)
And then I thought about my own father— who was a patient of congestive cardiac failure.
I only got to bring him to the ER once, where the on-duty doctor attached normal saline to him. Despite my repeated insistence to stop the fluids, he confidently convinced me that the patient was simply dehydrated and there's absolutely nothing to worry about
The second time I brought my father to the ER… it was the next morning, and he was already dead
For a moment, it hit me deeply how blessed those children are.
Of course, life and death are only in Allah’s hands, but some moments leave wounds that stay deep in the heart. Today it was one of those "some moments"
It'll haunt me for the rest of my life and I'll never heal from that!
1
51
2,769
Dr. Fahad Khaliq retweeted

May 19
Asl struggle tu MBBS k baad start hoti ha.🙂
6
3
52
3,008
May 19
I'm both dumber and smarter than you think. Do NOT judge me 💀
7
304
Dr. Fahad Khaliq retweeted

May 18
It's a God forsaken country. No matter how sincere and hardworking you're. System will beat your down every time. It's a heaven for people who are filthy rich or corrupt or both. Rest are just following pathetic rules by will or by brutal force. Leave if you can.
1
24
100
2,077
May 17
Idher ma furosemide ki infusion chala raha hun, aur udhar se baba ji ne aik haath me TUC biscuit aur doosre hath mei liter paani ki botal pakri v hai
.
😭😭😭😭😭😭😭
OoOoOOOOooOo bhaiiii maro mujhyy
4
1
55
2,662
May 16
Louder! 📢📢
Sometimes these cruel attendants bring patients to the hospital not out of hope for recovery, but out of fear that society will blame and shame them if the patient dies at home. And when they teach the hospital, their concern literally shifts more towards the financial expenses than the patient's well being himself.
Some more cruel attendants even begin hoping that the patient's suffering ends quickly just to avoid further financial burden.
I denied this observation countless times, but repeated patterns eventually forced me to finally acknowledge it.
Honestly, that reality is deeply painful.
May 16

Hate to break it but many attendants hate their patients and even wish that they're better of dead. When they expect staff to take care of them entirely & don't do anything, even leave them alone. The want to dump their responsibilities on medical staff, and it's not uncommon!
1
2
43
2,190
May 15
Dullness on percussion? 🥁
Here are differentials!
• STONY dull OPPOSITE tracheal deviation = EFFUSION
• NORMAL trachea NORMAL breath sounds = PLEURAL THICKENING
• INCREASED vocal resonance ± Bronchial Breathing & Crepts = CONSOLIDATION
• ABSENT Breath sounds SAME side tracheal pulling REDUCED Lung volume = COLLAPSE
1
3
21
1,106


May 14
No pay for 2.5 months for intense donkey work at Emergency Department!
Time to shift treatment protocols from "UK (United Kingdom) International Guidelines" to "UK (Umer Kot) Local Guidelines" 💀
Like people, like treatment protocols!
P.S. Just in case you forgot, the name of the recruiting program was "Special Pay Package" 🫡
7
8
95
4,589
By the grace of Allah Almighty, here’s another step towards my dream and fav fav consultantship qualification:
𝗠𝗲𝗺𝗯𝗲𝗿𝘀𝗵𝗶𝗽 𝗼𝗳 𝘁𝗵𝗲 𝗥𝗼𝘆𝗮𝗹 𝗖𝗼𝗹𝗹𝗲𝗴𝗲 𝗼𝗳 𝗣𝗵𝘆𝘀𝗶𝗰𝗶𝗮𝗻𝘀 𝗼𝗳 𝘁𝗵𝗲 𝗨𝗻𝗶𝘁𝗲𝗱 𝗞𝗶𝗻𝗴𝗱𝗼𝗺 𝗣𝗮𝗿𝘁 𝗜𝗜 — 𝗣𝗔𝗦𝗦𝗘𝗗! 💫
Within just 1 year of completing the house job, and at the age of 26, I’ve achieved far far more than I ever imagined:
Certified Cardiologist (UK) ✅
Certified Diabetologist (UK) ✅
And "Almost" a Consultant Physician 🔥
Dr. Muhammad Fahad Khaliq
MBBS Gold Medalist (PMC)
MRCP (UK)—II, Dip. Card (UK)
Dip. Diab (UK), B. Sc. (Eng.), RMP
26
1
125
4,934
May 12
Thank you all so much for the beautiful wishes and kind comments. I’m truly grateful for every word and every prayer 💫
Apologies that I may not be able to reply to each comment personally due to time constraints, but please know that I have read them all and I truly appreciate your beautiful replies ⭐🫰🏻
May Allah bless you all with good health, happiness, prosperity, and endless success.
Thank you once again for all the love and support. Really means a lot to me ❤️🥳✨
1
168