
Myeloma and Amyloid Oncologist, Asst Professor of Medicine@hackensackUMC. Local guide NYC restaurants. Ravenclaw. Tweets are my own
Joined August 2009
- Tweets 1,364
- Following 305
- Followers 369
- Likes 3,270
23 Photos and videos










Jun 4
I propose a principle. Kaplan Meier reliability heuristic. The core rule: If majority of censoring occurs prior to 67% events, the data is immature and needs more followup before jumping to conclusions. Below this event fraction, sample size is too small to anchor the curves well
85
Jun 1
A rough bullsh*t detector when p values look amazing. For HRs look for CI. If upper 95th/lower 95th bound CI ratio is <2 = strong finding. 2-3=ok. 3-4=‘wobbly’ HR. >4 = useless
98
Harsh Parmar MD retweeted

21 Sep 2025
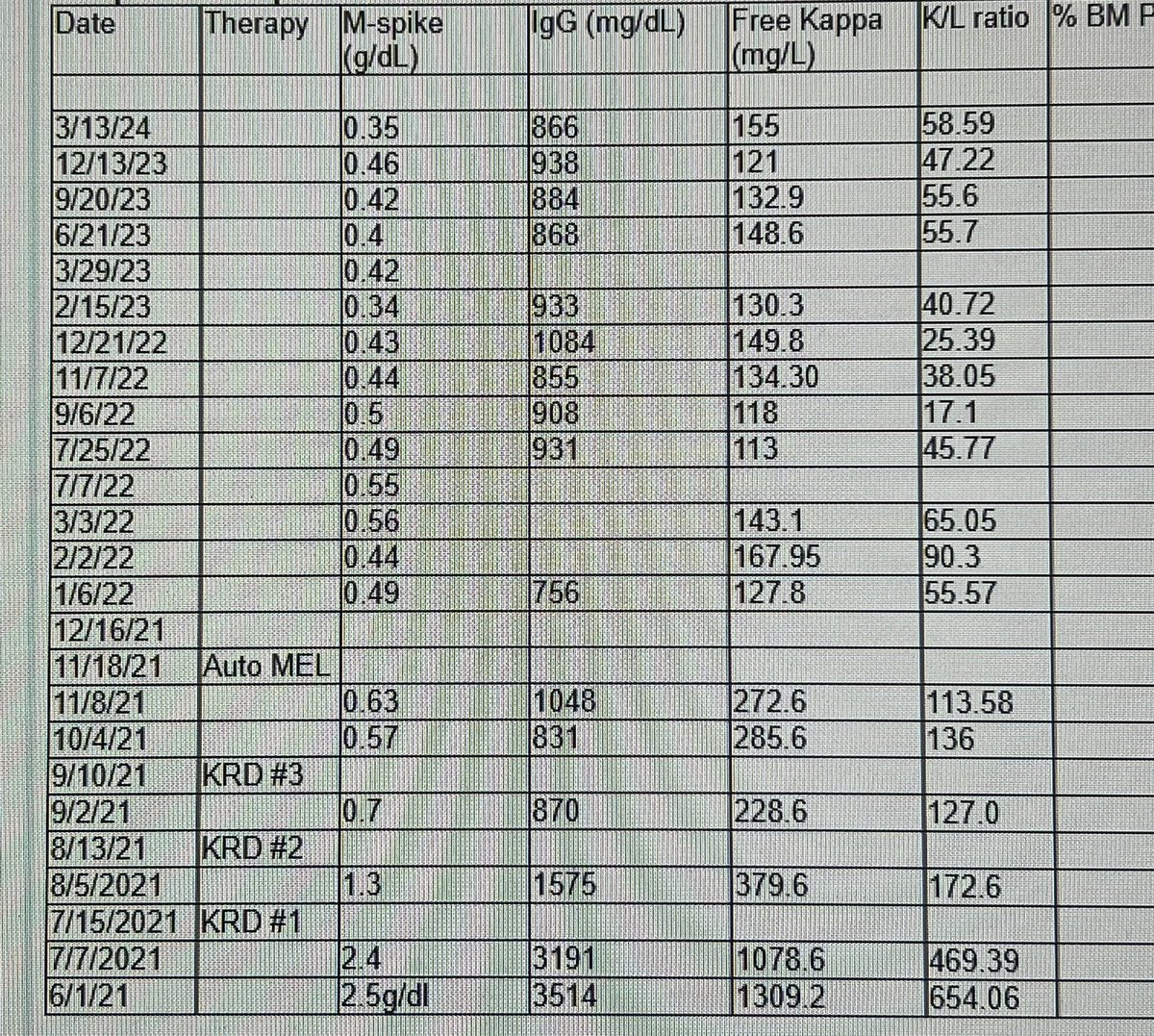
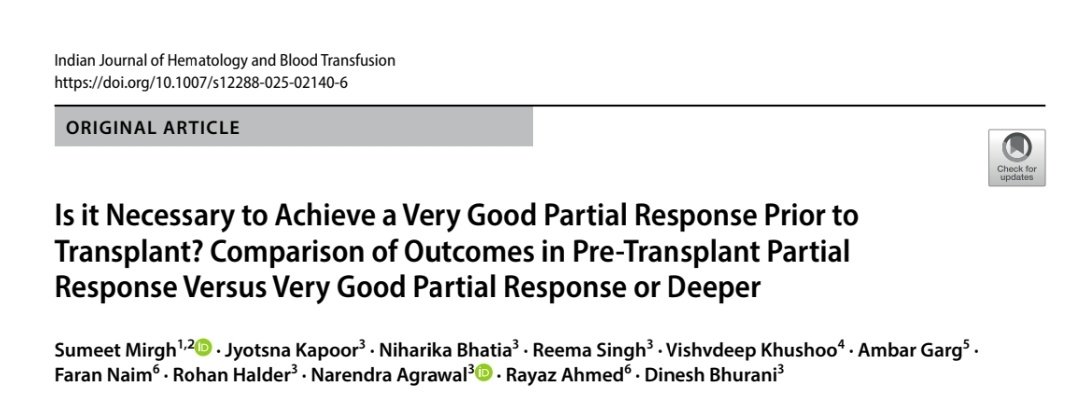
PR after induction - "Go on" to ASCT OR "Hold on" for VGPR and then do ASCT. A dilemma which many of us face in practice. Our analysis from my previous workplace which answers this important question @ishbtish @IndMyAcGp @DrPMPGI @UdayYanamandra @IsbmtU
1
13
46
11,324
Harsh Parmar MD retweeted

21 Aug 2025
I like this approach. Depositing light chains is toxic, and the treatment of AL should be considered a quasi-emergency! Almost like renal failure in MM.
#everydaymatters
1
1
9
952
Harsh Parmar MD retweeted

20 Aug 2025
Important clinical pearl from @Ron_Witteles! In cardiac AL, I check FLCs q-weekly in the first couple of months, and switch treatment if I sense plateau. “Every day matters” for the component of toxic cardiomyopathy from circulating FLCs.
20 Aug 2025

Congrats to the authors, but 2 critical points: 1) There’s no role for PYP scan in setting of monoclonal protein. 2) “Promptly diagnosing” does not mean 1-2 months from time of suspicion. When #AL #amyloidosis is in the differential, it’s a near-emergency — every day matters.
2
5
16
3,454
12 Aug 2025
Talquetamab dysguesia and xerostomia. Try this-
Pilocarpine 2.5mg BID (upto 4 times a day) - can help
1
14
691
Harsh Parmar MD retweeted

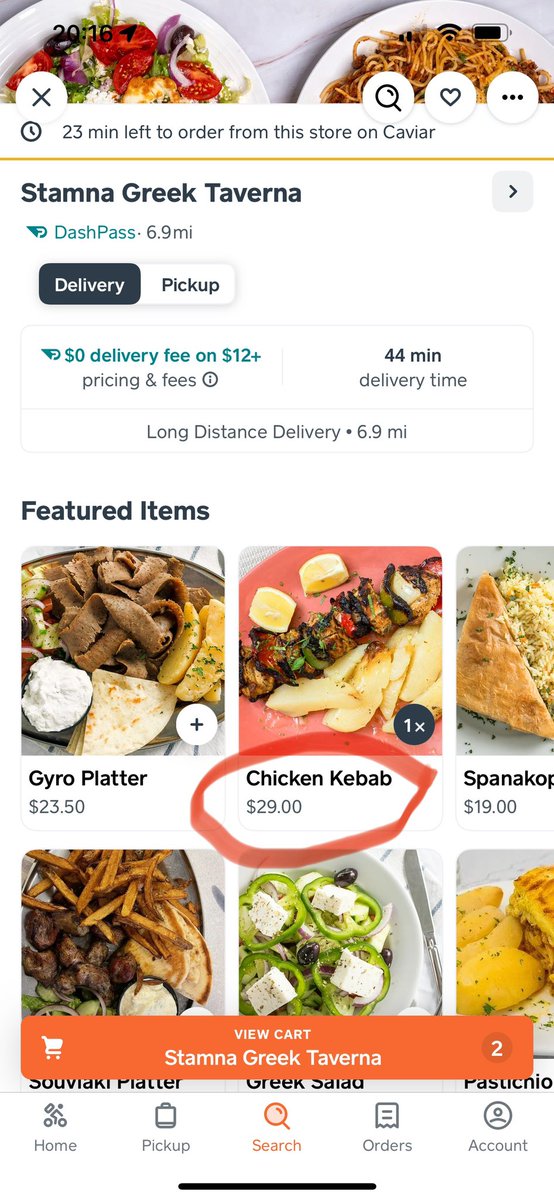
6 Jul 2025
Went to pick up a prescription at the pharmacy and with my prescription card it was $467…. Cash price $63.40. Our healthcare and insurance system, and the Pharmacy benefit managers have created the biggest fraud machine I’ve ever seen.
286
2,110
10,302
194,907
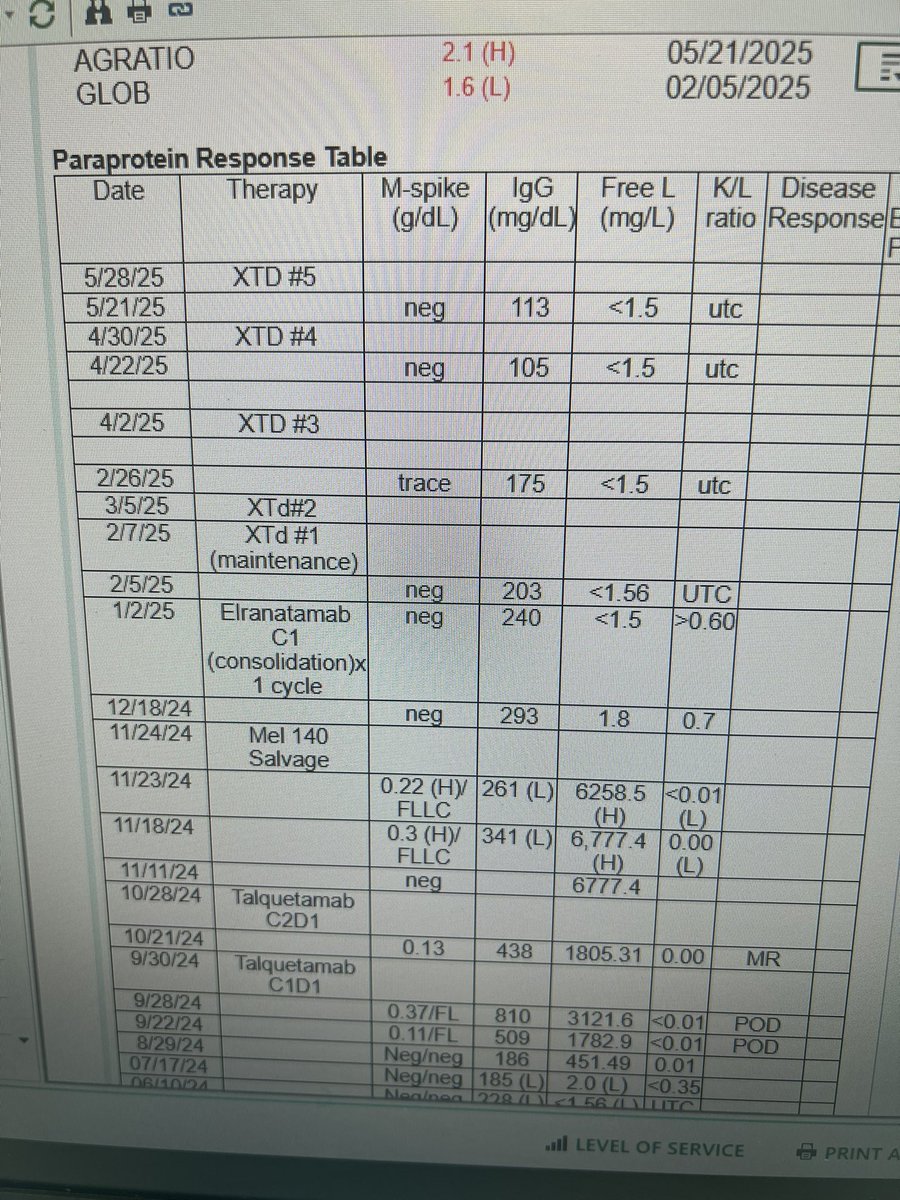
26 Jun 2025
6 prior LOTs. Anti-bcma cart failed (carvykti)-progressed x 2 months.Progressedx2 cycles of talq. Salvage Mel with a strong response, ‘consolidation’ elra x 1 and now on ‘maintenance’ selinexor (100mg weekly) thalidomide 400, in CR. No nausea, no fatigue. *Every* therapy matters
1
3
13
1,618
12 May 2025
MM in >=4 LOT misbehaves a lot. Multiple pts on TCE or post cart even if not meeting progression by dFLC but consistent iFLC trend increment with end organ damage (mostly skeletal events).Perhaps the LC or m-spike criteria need adjustment allowing change of Rx before these events
3
458
8 Apr 2025
70 F with RRMM 4 prior lines, triple ref. Bcma sensitive, diagnosed with stage IIb melanoma on adjuvant pembro since 7/2024 planned x 1 yr. Concerned about cart with LD w flu/cy or benda ld (interrupt w adjuvant therapy efficacy), data for TCEs w CPI(?)
452
27 Feb 2025
I have used anti-bcma therapy AFTER anti-gprc5d therapy more frequently these days; I see no issues with compromised responses even if done sequentially. (TCEs) for the most part. Any data presented for this?
1
1
657
13 Feb 2025
Waldenstrom/LPL defines disease progression biochemically as a 25% increment in IgM from best response but no minimum threshold considered in terms of an absolute value increase ? I know most of us go by clinical symptoms regardless
2
519
4 Feb 2025
AL question- post treatment initiation (eg.post asct) once uiFLC>iFLC,are we considering heme progression across the mathematical line to consider 50% increment to include negative difference and subsequent positive difference once iFLC>uiFLC? I think we should be
403
21 Jan 2025
Any experience with CAR-T in AL for pts with profound dysautonomia? Supine SBP 170s, drops to 80s while standing, already on midodrine, fludrocortisone for hypotension (trial of pyridostigmine??)
1
384
2 Jan 2025
About 30% of my pts achieve biochem CR with some of the bridging therapies (TCEs or HD mel) with the goal of CAR. (Most 4th LOT). Bridge administered post apheresis. I am opting to wait and monitor closely until progression (can preserve CARs upto 6 months). Any thoughts?
4
2
11
3,450
31 Dec 2024
Any data on post transplant outcomes of patients who have not been exposed to any novel therapies in the contemporary era ? I know no one does this any more but curious. (Eg. PACE based induction)
1
566
30 Dec 2024
IgGs over 10,000 have been known to be associated witth hyperviscosity although at levels 5000s or over, I have seen volume overload and pseudohypoNa. Any data on this? When I give car to this subset of pts- tolerance is poor. BNPs tend to run high
2
2
9
1,916

Google just announced a breakthrough in quantum computing.
It's called "Willow" - and it's making waves in the tech world.
But buried in their announcement was something fascinating:
A discovery that could reshape our understanding of computing itself...

22
233
1,356
501,699
Harsh Parmar MD retweeted

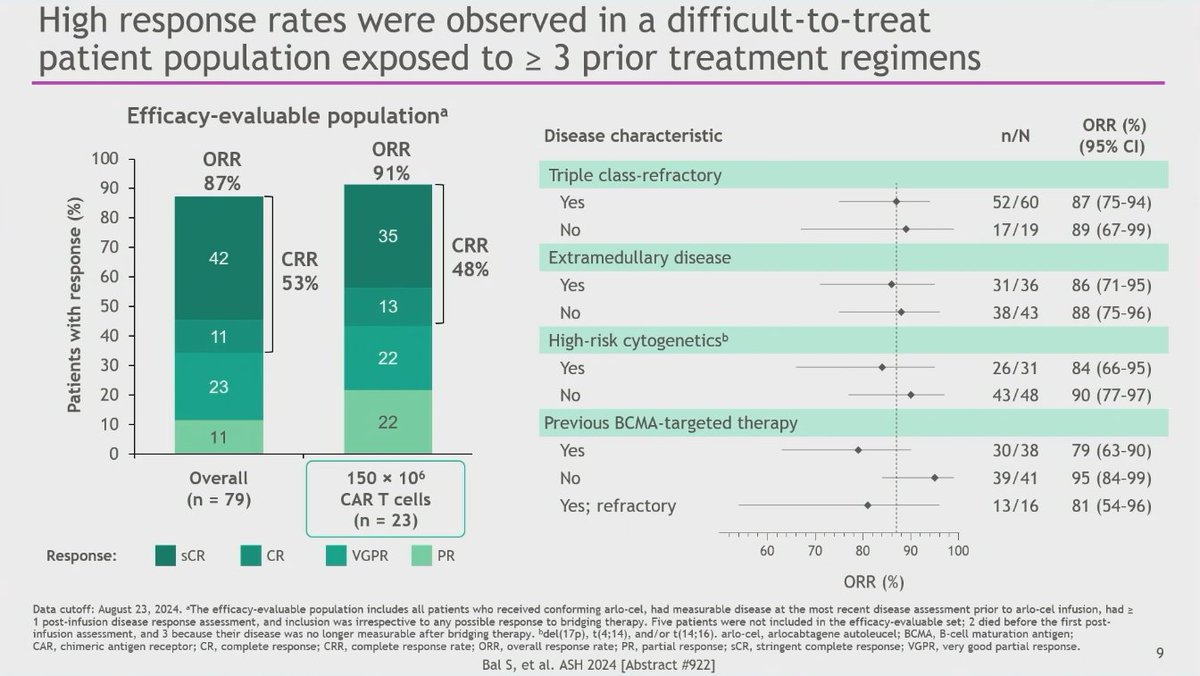
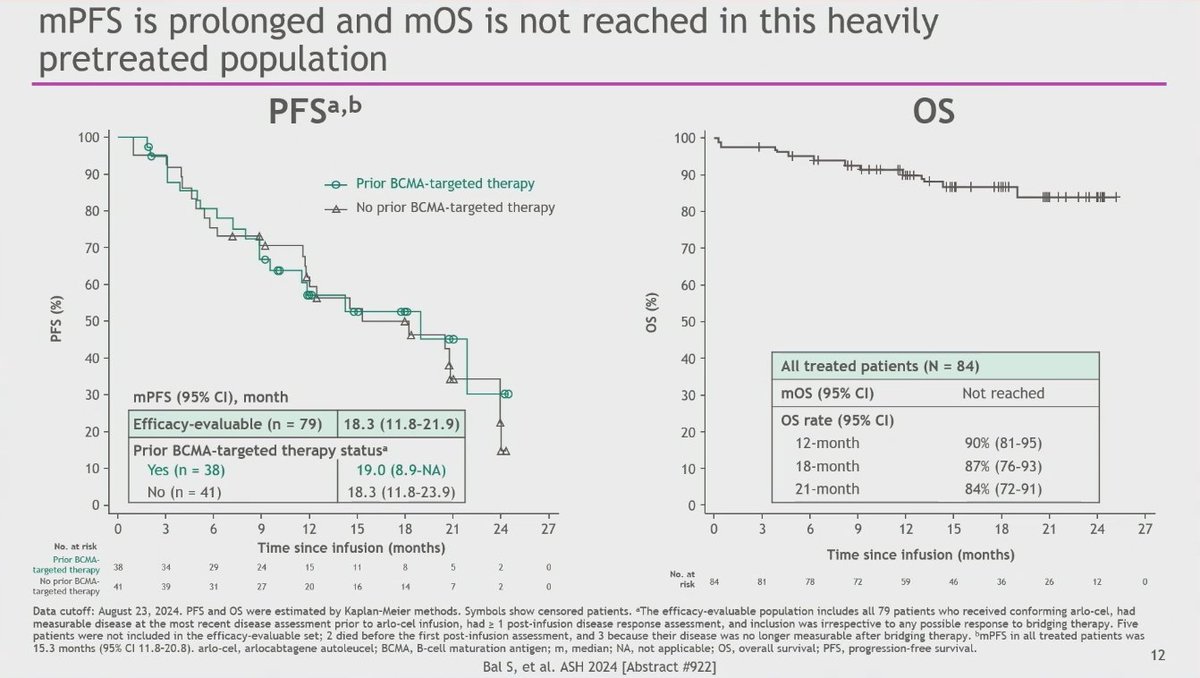
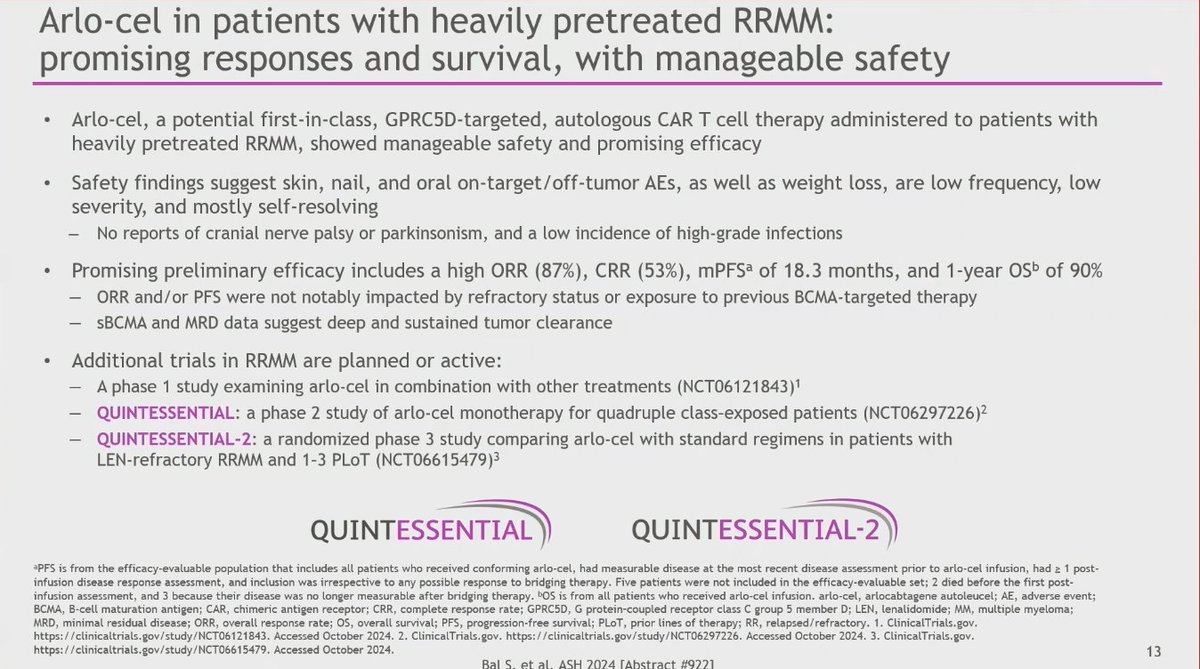
11 Dec 2024
CONGRESS | #ASH24 | Susan Bal @SusanBal9 @UABNews shares extended FU data from the Phase I study of arlo-cel (BMS-986393) in heavily pretreated RRMM. ORR 87%, CR 53%, 150x10^6 CAR T cells ORR 91%, median DoR 18-mo, median PFS 18.3-mo, 12-mo OS 90%.
Follow our live feed for more updates: loom.ly/o2oK2qI
#mmsm #myeloma #MedicalCongress

6
17
1,480
10 Dec 2024
PE interventions might be profitable to the company margins but that implies changes which destroy the morale of business ventures. Perhaps acceptable in most industries, in the healthcare sector it can be cataclasmic. Saddened by this
cnn.com/2024/12/10/business/…
179