
MD/MBA @PennMedicine @Wharton | Hospitalist | Creator @pointofcaremed | Follow for clinical threads and pearls
Joined December 2011
- Tweets 1,785
- Following 1,077
- Followers 5,138
- Likes 7,199
276 Photos and videos






Daily Pearl(s):
Light Chain Multiple Myeloma
In light chain myeloma, malignant plasma cells exclusively produce and secrete monoclonal free light chains (kappa or lambda) without the corresponding heavy chain.
Light chains are not detected on standard serum protein electrophoresis (SPEP) but are identified by the serum free light chain (SFLC) assay.
The classic presentation of light chain myeloma is captured by the CRAB criteria: hyperCalcemia, Renal insufficiency, Anemia, and Bone lesions.
However, the order of prevalence is more accurately reflected by the BARC mnemonic: Bone lesions, Anemia, Renal failure, hyperCalcemia.
Myeloma causes AKI through several mechanisms, most commonly cast nephropathy, where excessive filtered light chains precipitate in and obstruct the renal tubules.
While myeloma typically causes a normocytic anemia from marrow infiltration, co-existing pathology like severe iron deficiency from chronic blood loss can be present and must be treated as well.
Source: CPS - April 13, 2026 Mainstream Mondays VMR with Youssef & Seeme - fatigue and lightheadedness
1
4
12
640
Learn more clinical pearls from the Point of Care Medicine Substack!
rokeefemd.substack.com/
1
423

Jun 12
Daily Pearl(s):
Pancreatitis
Lipase, while more specific than amylase, is not perfectly specific for pancreatitis. It can be falsely elevated in DKA/HHS, renal failure, and mesenteric ischemia, creating significant diagnostic pitfalls.
The pathophysiology of severe pancreatitis involves two distinct processes: local autodigestion leading to necrosis and fluid collections, and a systemic vascular leak syndrome causing multi-organ failure like ARDS and shock.
Severe, palpable epigastric tenderness is a classic and crucial clue, suggesting local peritonitis from the inflamed pancreas. It can also help differentiate it from other, less tender causes of epigastric pain like PUD.
Source: CPS - April 11, 2026 Academy with Rabih - pancreatitis
1
7
30
1,740
Jun 12
Learn more clinical pearls from the Point of Care Medicine Substack!
rokeefemd.substack.com/
2
810
Jun 11
Daily Pearl(s):
Xanthogranulomatous Cholecystitis (XGC)
XGC is a rare destructive inflammatory disease of the gallbladder that is a variant of chronic cholecystitis.
It is characterized by a massive inflammatory reaction that often forms a tumor-like mass, making it a well-known mimic of gallbladder carcinoma.
A non-visualized gallbladder replaced by an inflammatory mass containing a large stone is commonly seen on imaging.
The pathophysiology is thought to involve chronic obstruction (typically by a large gallstone), leading to increased intraluminal pressure and rupture of the Rokitansky-Aschoff sinuses. This allows bile to extravasate into the gallbladder wall, inciting a significant inflammatory response dominated by lipid-laden macrophages (xanthoma cells), lymphocytes, and fibrosis, which can even invade adjacent structures like the liver, making it look like a malignancy.
Source: CPS - April 9, 2026 VMR with Rabih & Siva - chest pain and vomiting
2
5
13
1,061
Jun 11
Learn more clinical pearls from the Point of Care Medicine Substack!
rokeefemd.substack.com/
1
429
Jun 10
Daily Pearl(s):
APDS Syndrome - A Primary Immunodeficiency
The combination of recurrent sinopulmonary infections, lymphoproliferation (hepatosplenomegaly, lymphadenopathy), and autoimmunity strongly suggests a CVID-like primary immunodeficiency such as Activated PI3K Delta Syndrome (APDS).
APDS is a syndrome of immune dysregulation, not just deficiency, explaining the concurrent findings of infection susceptibility and hyper-inflammatory states like lymphoproliferation.
Recurrent or severe bacteremia with enteric organisms (E. coli, Salmonella) in an adult should prompt consideration of a primary immunodeficiency.
Source: CPS - April 8, 2026 VMR with Andrew & Kirtan - leukocytosis
1
3
11
958
Jun 10
Learn more clinical pearls from the Point of Care Medicine Substack!
rokeefemd.substack.com/
696
Ryan O'Keefe retweeted

Jun 9
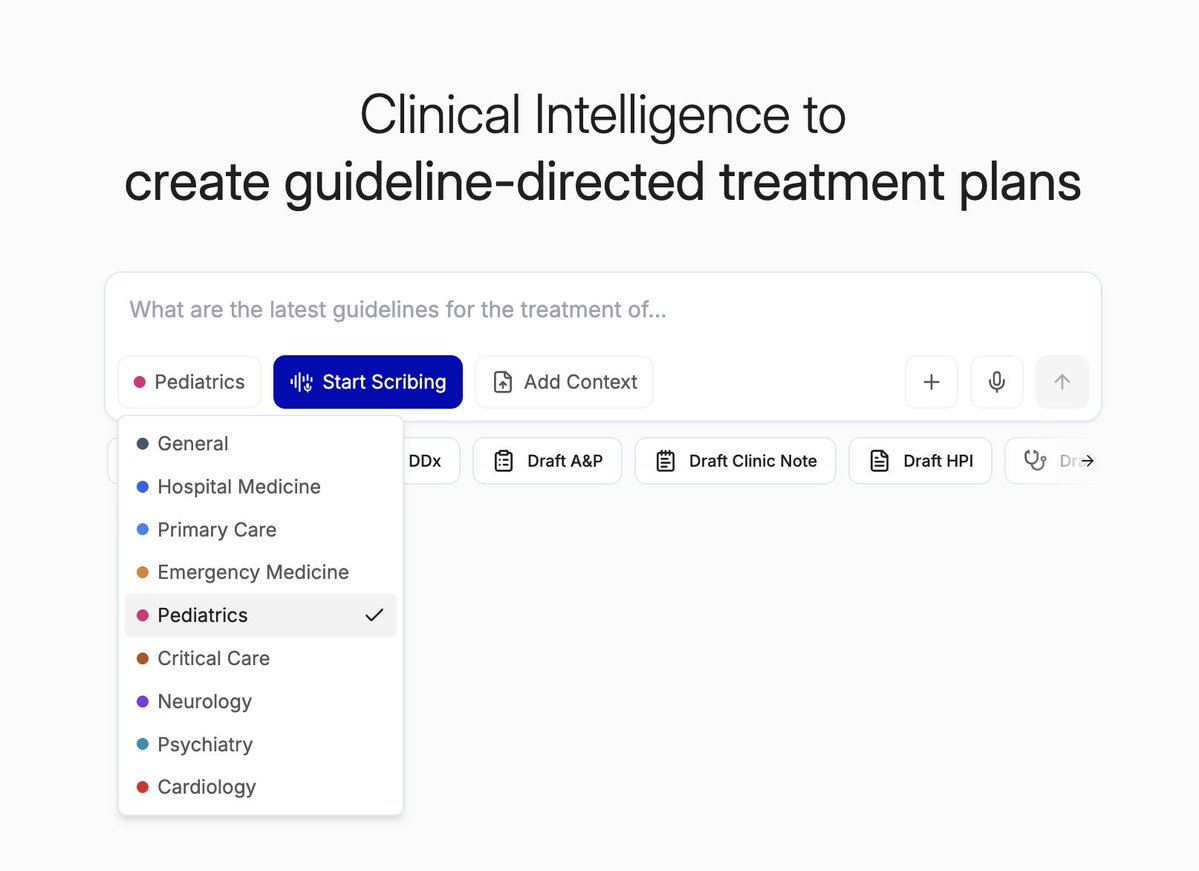
New specialty modes for colleagues in peds, cards, crit care, psych, and neuro are out today!

Glass has new specialty modes, designed to deliver AI deeply tailored to your clinical workflow. Choose your mode, and our AI's clinical reasoning, insights, and documentation will be tailored to the way you practice at glass.health
3
15
4,839
Jun 9
Daily Pearl(s):
"Unmasking" Sarcoid
The finding of significant interstitial fibrosis in a patient with a long-standing "asthma" diagnosis should prompt consideration of mimickers, including sarcoidosis which can cause airway hyperreactivity.
The withdrawal of a broad immunosuppressant like corticosteroids can unmask an underlying inflammatory disorder, such as sarcoidosis, that was previously being inadvertently treated.
A "silent" lung exam (clear to auscultation) in the presence of interstitial disease on imaging can be a clue for sarcoidosis, in contrast to IPF where bibasilar crackles are nearly universal.
PTH-independent hypercalcemia with an elevated 1,25 vitamin D level is a strong indicator of a granulomatous disease (like sarcoidosis, endemic mycoses, TB) or lymphoma.
Source: CPS - April 8, 2026 VMR with Steph & Zaven - worsening skin lesions
1
6
21
834
Jun 9
Learn more clinical pearls from the Point of Care Medicine Substack!
rokeefemd.substack.com/
3
328
Jun 8
Daily Pearl(s):
Streptococcal Toxic Shock Syndrome (STSS)
The syndrome is mediated by streptococcal pyrogenic exotoxins that act as superantigens, triggering a massive, non-specific T-cell activation and subsequent cytokine storm.
This leads to profound capillary leak, diffuse erythroderma (a "sunburn" rash), fever, and multi-organ failure.
Septic cardiomyopathy is a well-described but severe complication of STSS, contributing significantly to refractory shock.
Treatment is a combination of a beta-lactam (Penicillin G) to kill bacteria, and clindamycin to suppress toxin synthesis (via inhibition of ribosomal protein synthesis). IVIG is often used as an adjunct to neutralize circulating toxins. Surgical debridement is crucial for source control in cases of necrotizing soft tissue infection.
Source: CPS - April 7, 2026 VMR with Maddy & Andrew - fever, cough, and widespread body aches
1
6
16
1,733
Jun 8
Learn more clinical pearls from the Point of Care Medicine Substack!
rokeefemd.substack.com/
1,085
Jun 7
Daily Pearl(s):
Immune Thrombocytopenic Purpura (ITP)
Isolated and profound thrombocytopenia (platelets <20,000) in an otherwise healthy-appearing patient is highly suggestive of ITP.
Non-palpable purpura suggests a primary platelet disorder, whereas palpable purpura points toward an inflammatory process like vasculitis.
The presence of "wet purpura" (purpura or blood blisters in the mouth) is a red flag for a very low platelet count and a significantly increased risk of severe bleeding.
The peripheral smear is a critical and non-negotiable step in the workup of thrombocytopenia to rule out life-threatening mimics like TTP (schistocytes) and acute leukemia (blasts).
ITP is a diagnosis of exclusion; always consider and rule out secondary causes such as infections (HIV, hepatitis), drugs, and other systemic autoimmune or lymphoproliferative disorders.
Platelet transfusions are generally not indicated in ITP due to rapid destruction by autoantibodies and are reserved for patients with active, life-threatening hemorrhage.
Source: CPS - April 6, 2026 Mainstream Mondays VMR with Maddy & Lera - rash
1
5
22
1,109
Jun 7
Learn more clinical pearls from the Point of Care Medicine Substack!
rokeefemd.substack.com/
3
476
Jun 6
Daily Pearl(s):
Creutzfeld-Jakob Disease (CJD)
Brain MRI with DWI is the most critical initial imaging modality for suspected CJD, with cortical ribboning being a highly suggestive finding.
The modern gold-standard CSF test to diagnose CJD is the Real-Time Quaking-Induced Conversion (RT-QuIC) assay, which has high sensitivity and specificity for detecting the pathogenic prion protein. Older, less specific markers include elevated 14-3-3 and Tau proteins.
Definitive diagnosis is via brain biopsy or autopsy showing spongiform degeneration, neuronal loss, and gliosis.
The presence of a normal gait in a patient with significant dementia is a key localizing feature, pointing away from subcortical/limbic diseases (such as Lewy Body Dementia, Vascular Dementia, NPH) and more towards a primary cortical process like Alzheimer's or CJD.
True "reversibility" of a chronic dementia that has evolved over months is exceptionally rare and is primarily a feature of pressure-mediated processes such as NPH and subdural hematomas.
Source: CPS - April 2, 2026 VMR with Rabih & Fahed - forgetfulness & confusion
2
5
26
1,663
Jun 6
Learn more clinical pearls from the Point of Care Medicine Substack!
rokeefemd.substack.com/
437
Jun 5
Daily Pearl(s):
IDA Causing a Prothrombotic State
Severe iron deficiency anemia is an underrecognized prothrombotic state that can contribute to thrombosis through mechanisms like reactive thrombocytosis and endothelial dysfunction.
Source: CPS - April 1, 2026 VMR with Maddy & Zakariyya G - headache
1
4
22
1,173
Jun 5
Learn more clinical pearls from the Point of Care Medicine Substack!
rokeefemd.substack.com/
2
469
Jun 4
Daily Pearl(s):
Dural Venous Sinus Thrombosis
Dural Venous Sinus Thrombosis, also known as Cerebral Venous Sinus Thrombosis, is the occlusion of cerebral venous sinuses or cortical veins by a thrombus.
It is an uncommon cause of stroke that tends to affect younger women. Though clinical presentations vary, headache is the most common symptom. Headaches can be acute and severe ("thunderclap"), subacute, or chronic.
Other presentations include focal neurological deficits, seizures, and signs of increased ICP. A key feature is that a normal neurological exam can be present despite a severe headache, which may delay diagnosis.
Source: CPS - April 1, 2026 VMR with Maddy & Zakariyya G - headache
2
4
17
809
Jun 4
Learn more clinical pearls from the Point of Care Medicine Substack!
rokeefemd.substack.com/
436