
starting from ~120k my goal is to hit 1M by 2028 latest. until then I will invest aggressively and take considerable risk. plan is to ~2x my portfolio each year
Joined August 2025
- Tweets 974
- Following 161
- Followers 116
- Likes 1,289
57 Photos and videos











A good piece going around on the $ABVX cancer cases. I agree with where it lands. Just want to add how I think about this and where I think it misses the crucial point of safety assessments.
The strong reasons are not really about math. They’re about the full picture: no clear reason the drug should cause cancer, clean preclinical work, the cancers are in different organs (not clustered), no wider “immune system weakened” pattern, the investigators called them unlikely related, and UC patients already get more cancer at baseline. That’s what carries it.
The Rinvoq comparison is the clearest point. Rinvoq’s signal came from a huge 4,500-patient study that matched a known prior worry. Obe has a couple of scattered cases in a population that gets these cancers anyway. Different situation entirely.
Where I’d be careful: the “you’d need ~10 more cases” number. It leans heavily on an assumption the author picked (a very large background dataset). Change that one input and the number drops a lot. So it’s not really a hard line … it’s an estimate that moves with the assumptions.
Also, counting cases is the wrong test. A real drug signal shows up as a pattern: same organ, linked to dose or time on drug. 4 cancers all in one organ would worry me more than 14 spread around. A simple count misses that. So: I trust the conclusion, just not that exact number. (And I checked the logic, not the actual math behind it.)

Based on our conversations with the buy side and sell side, one thing is clear: the market is still struggling to define the actual safety bar for $ABVX.
Specifically: how many non-NMSC events would ABTECT Maintenance Part 2 need to show before FDA reviewers or sophisticated pharma BD teams should become concerned that obefazimod may have a true carcinogenic signal, rather than background malignancy events in a refractory UC population?
We provide our analysis and conclusions below. Said simply: under our assumptions, $ABVX would need to show a malignancy burden far beyond one or two incremental cancer cases before the bear case becomes statistically and biologically coherent.
When a drug trial reports a handful of cancer cases, the natural question is: is this a real signal, or just bad luck? A drug study with 150 patients over one year will almost certainly see some cancers — because UC patients get cancer at a background rate even without any drug. In fact, even otherwise healthy people get cancer at a background rate without any drug. The real question is whether the number of cancers seen on the drug is more than we would expect by chance from that background rate alone.
Enter statistics: the formal language of separating signal from bad luck. In this case: what is the event burden and pattern that is high enough, coherent enough, and biologically plausible enough to overcome a low causal prior to obefazimod being carcinogenic?
This is exactly the kind of question Bayesian inference is useful for answering.
Our Bayesian inference model asks a simple question:
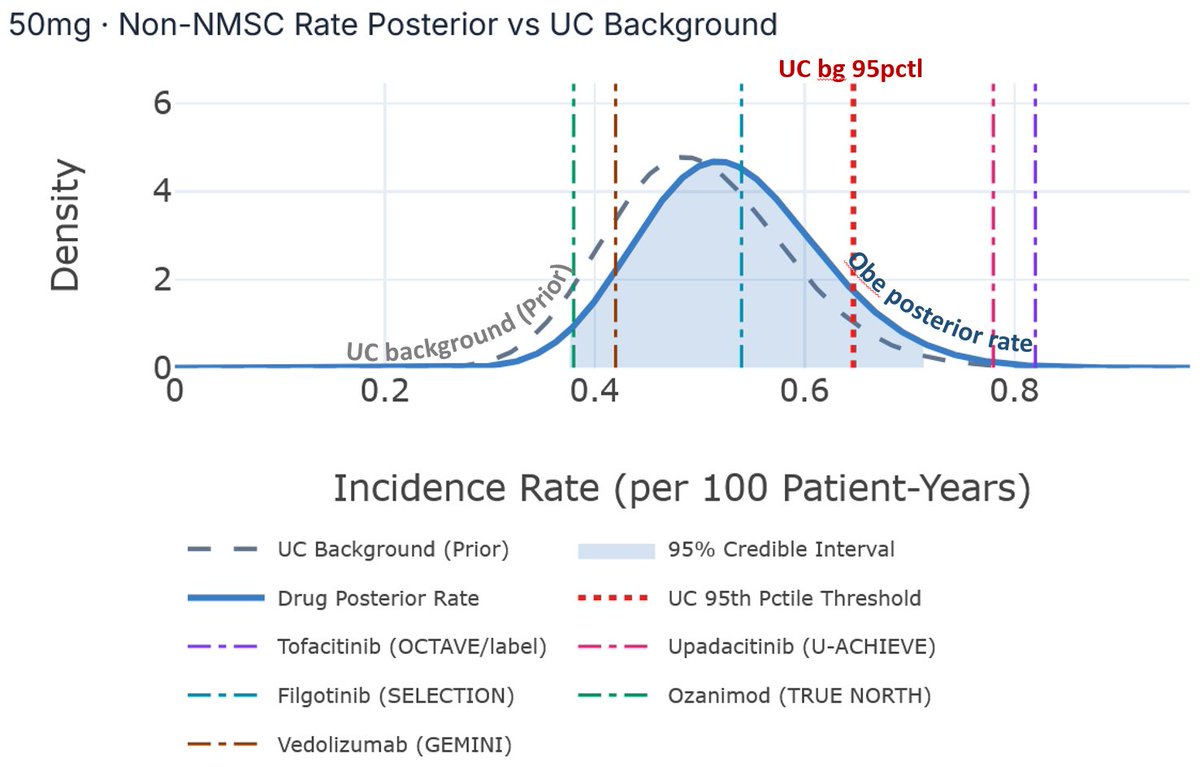
Given an estimated background non-NMSC incidence rate of ~0.5/100 PY, how many additional non-NMSC events would need to appear in the next ~450 PY of 50 mg exposure before the pooled 50 mg maintenance dataset begins to look meaningfully above UC background?
At ~0.5/100 PY, the expected background incidence over ~450 PY is roughly 2–3 non-NMSC events.
Our model suggests the upcoming 50 mg Part 2 update would need to show something closer to 10 additional events above background — roughly 14 total non-NMSC events in the pooled ~600 PY 50 mg maintenance dataset — before the posterior begins to suggest a >50% probability that the true obefazimod non-NMSC rate exceeds the upper bound of UC background.
We favor a Bayesian inference framework in these cases because it contemplates the data through a lens similar to that of what we believe an FDA reviewer and pharma regulatory teams would look through: exposure-adjusted rates, confidence intervals around those rates, event heterogeneity, organ clustering, baseline UC cancer risk, prior therapy risk, timing of exposure, investigator attribution, and whether the pattern resembles a broader immunosuppressive AE phenotype.
Most importantly, with this approach we do not need to assume obefazimod causes cancer. In fact, the causal prior should be low because there is no obvious a priori hypothesis for obefazimod causing cancer, including clean preclinical work, no clustering to a specific cancer type, no broader adverse event pattern associated with impaired immune surveillance, and investigator assessment that the disclosed prostate and breast cancer cases were unlikely related.
Thus, the analysis is not whether “observed cancers divided by patient-years is greater than zero.”; that is coarser than the data allows. The question is whether the observed event pattern is adequate to overcome a low causal prior.
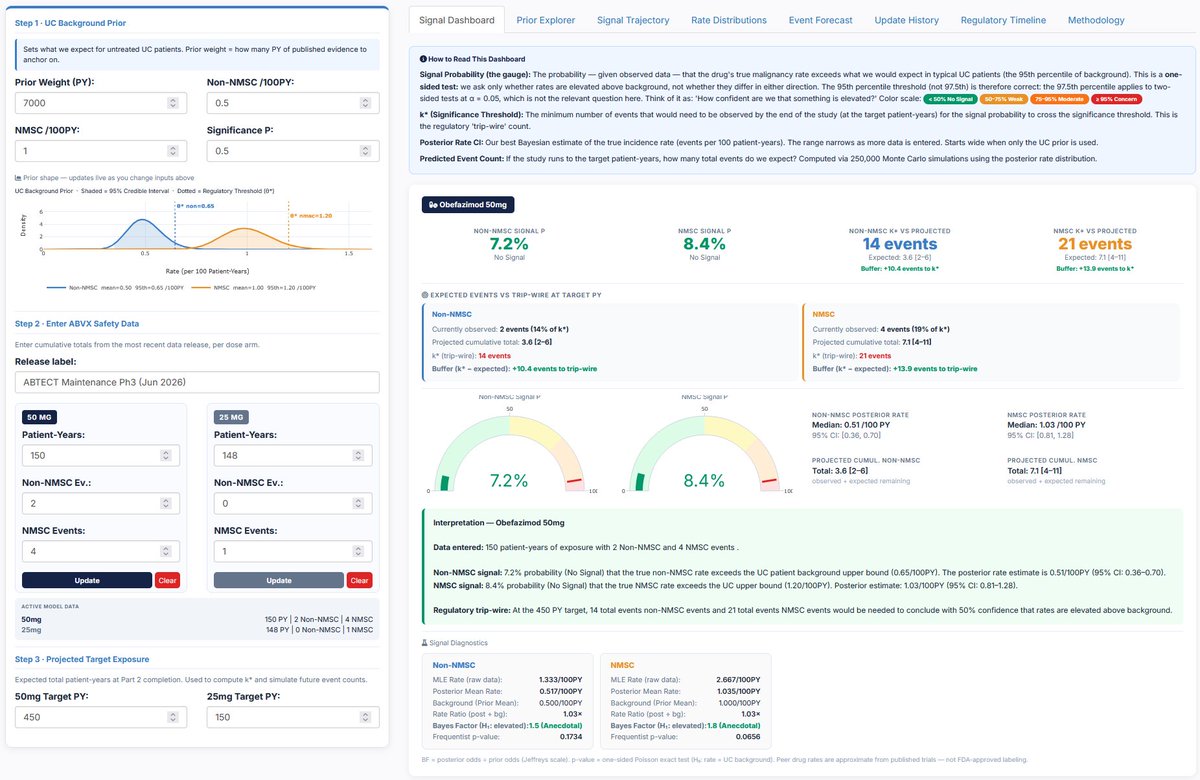
We estimated background malignancy IRs across an aggregate 7000 PY based on a synthesis of Colombel et al. (2017), Rubin et al. (2026), D’Haens et al. (2023), Swissmedic (2024), Sands et al. 2026, Abreu et al. (2022), and Sandborn et al. (2019), and arrived at an estimated non-NMSC IR of 0.5, which is the midpoint of the range provided by management in the Part 2 primer deck published earlier today (ir.abivax.com/static-files/7…). We use 0.5/100 PY as the non-NMSC IR as the background prior of our model. Our analysis allows us to use 7000 PY as the weight of that prior probability. Then, we ask how many non-NMSC events need to be observed in the ~450 PY from Part 2 for the aggregate obefazimod non-NMSC IR to indicate that the true obefazimod non-NMSC rate exceeds the UC patient background upper bound with at least 50% probability. We set the PY reported in ABTECT Maintenance Part 1 according to management feedback.
An estimated background non-NMSC IR prior of 0.5/100 PY is at the midpoint of the range provided by $ABVX management and implies an expected 2-3 non-NMSC events per 450 PY. Our model suggests that the ABTECT Maintenance Part 2 update for the 50 mg dose would need to show 10 additional events over and above those background events in 450 PY (i.e., total of 14 non-NMSC events) before the pooled 600 PY maintenance dataset (Part 1 Part 2) for the 50 mg dose to indicate a greater than 50% probability that the true obefazimod non-NMSC rate is greater than the upper bound of UC background rate, when the observed non-NMSC IR begins to possibly be considered elevated above background expectations.
Even when we cut the prior probability weight in half to 3500 PY, the conclusions remain unchanged: ABTECT Maintenance Part 2 update for the 50 mg dose would need to show 7 additional non-NMSC events over and above the number of events expected given the background IR before the pooled 600 PY maintenance dataset (Part 1 Part 2) for the 50 mg dose to indicate a greater than 50% probability that the true obefazimod non-NMSC rate is greater than the upper bound of UC background rate.
Said differently, the key risk is not that another cancer event occurs; the UC and IBD literature documents an expected incident rate for non-NMSC at their background rate (0.3-0.7/100 PY).
The key question is whether the next ~450 PY expected from the Part 2 50 mg arm is consistent with the drug-driven malignancy hypothesis: repeated non-NMSC events, organ clustering, biological patterning, exposure-duration logic, or a broader immune-surveillance signal.
That is what our model tests.
If the next cut instead shows low-count, disparate, background-plausible events, the current obefazimod-driven malignancy argument becomes increasingly difficult to sustain.
But what about Rinvoq? They didn’t see a big imbalance?
This is not a Rinvoq/Xeljanz-style RA safety signal, where a nearly 4,500-patient outcomes study produced a statistically significant malignancy and immunosuppressive AE cluster in line with an a priori safety hypothesis prior. So far, these few malignancy observations are easily explainable by the background rate of UC cancer in this population especially, and mechanistically, there is also no obvious reason to believe obefazimod should be carcinogenic. If anything, Qin et al. (miRNA-124 in Immune System and Immune Disorders - PMC) discuss miR-124 biology in anti-proliferative and anti-fibrotic contexts, though we would not underwrite an anti-cancer effect here.
Against the magnitude of efficacy demonstrated by obefazimod to date: ~50% clinical remission versus ~10% placebo, plus large effects on endoscopic remission, HEMI, steroid-free remission, and sustained remission that is life-altering; these non-NMSC events do not appear to alter the risk-benefit equation.
We do not think these disclosed data support a black box. A black box for what appears likely to be background artifact would risk causing net harm to patients by creating unnecessary friction around delivery of a novel and highly efficacious therapy.
A brief comment on NMSCs: Based on our diligence, including conversations with former FDA review leadership responsible for evaluating new IBD drug approvals, NMSCs are most commonly basal cell carcinoma and cutaneous squamous cell carcinoma. Importantly, these cancers are: 1) very common; 2) very slow growing; 3) very visible; and as a result, 4) very treatable and curable. These cancers are rarely metastatic, and very rarely fatal.
There is published evidence that IBD patients appear to be at elevated rates of NMSCs, hypothesized to result from either higher baseline persistent inflammatory processes and/or thiopurine use.
In fact, clinical guidelines published in April 2025 following an expert panel from the American Gastroenterological Association Clinical Practice Update provided specific guidance that all adult patients with IBD should follow skin cancer primary prevention practices by avoiding excessive UV exposure, that patients on immunomodulators, anti-TNF biologic agents, or small molecules should undergo yearly total-body skin exam, and that patients with any history of thiopurine use should continue yearly total-body skin exam even after thiopurine cessation.
In the cohort study, the incidence of NMSC was higher among patients with IBD compared to controls (IRR 1.64, 95% CI 1.51–1.78). Recent thiopurine use was associated with NMSC (adjusted OR 3.56, 95% CI 2.81–4.50), and persistent thiopurine use was associated with NMSC (adjusted OR 4.27, 95% CI 3.08–5.92).
While, prior to our analysis, we were not concerned that the FDA or pharma would view elevated NMSC rates as a major issue, we were concerned that investors might continue to misclassify them as a serious systemic malignancy signal. However, based on recent conversations with other buysiders, we sense the market is beginning to understand that NMSCs are not a meaningful issue here: they are generally detectable, manageable, and already incorporated into the standard-of-care dermatologic monitoring framework physicians use for UC patients.
For completeness, we repeat our Bayesian inference analysis as described above but for NMSC. Taking the NMSC background IR of 1/100 PY provided by management today, we expect 4.5 cases in a 450 PY dataset. Our model suggests that the ABTECT Maintenance Part 2 update for the 50 mg dose would need to show 12 to 13 additional events over and above those background events in 450 PY (i.e., total of 21 NMSC events) before the pooled 600 PY maintenance dataset (Part 1 Part 2) for the 50 mg dose to indicate a greater than 50% probability that the true obefazimod NMSC rate is greater than the upper bound of UC background rate, when the observed NMSC IR begins to possibly be considered elevated above background expectations.
In summary: The right conclusion is not that no cancer events occurred, or that no events will occur in the future. They will occur, not only because cancer risk is elevated in UC, but because cancer can occur in anyone, at any time, including otherwise healthy patients.
We think the right conclusion is that the events that did occur look explainable by baseline patient risk, common cancer epidemiology, UC biology, and routine screening detection, rather than acting as evidence of an obefazimod-specific oncogenic signal.
We think FDA reviewers and pharma regulatory teams are more likely to reach this conclusion than to view the disclosed cases as a coherent obefazimod-specific malignancy signal, making increasingly clear what we believe is a best-in-disease efficacy/risk profile in the lucrative maintenance setting for UC and substantially de-risking the company’s opportunity in Crohn’s.
Disclosure: I/we may be long ABVX and may buy, sell, hedge, or otherwise change exposure at any time without notice. Not investment advice or a recommendation. Analysis reflects current views and assumptions based on public disclosures, published literature, and non-confidential conversations, and may change as new data become available. No compensation from ABVX or any third party.
8
1,241
$ABVX malignancy “signal,” straight:
2 cancers, 2 different organs, 1 patient each, no clustering … and infections below placebo.
That’s the fingerprint of background ascertainment, not a drug effect.
Why JAK is the wrong comp:
JAK’s malignancy case was convergent … immune-surveillance MoA preclinical signal dose-response a head-to-head loss to anti-TNF, all pointing one way.
Obe has none of those pillars. It only rhymes on the headline.
Safety can kill a product pre-authorization, but it kills on a confirmed, serious, unmanageable risk, not a watched one. Marketing authorisation turns on efficacy and baseline safety; a manageable or merely-possible risk doesn’t block the gate …
it gets routed to post-licensing follow-up, where the data to actually adjudicate it accrues.
Two unclustered cancers in a confounder-heavy population is the textbook “watch it, don’t gate on it” case.
Likely path:
isolated events, watched question deferred to post-marketing pharmacovigilance / a PMR, monitoring language on the label … no box, no Rx deterrent.
Validated if:
the exposure-adjusted Part 1 50mg-vs-placebo malignancy rate lands in IBD background range, and the Type B pre-NDA doesn’t flag malignancy as a major review issue.
My opinion only, no investment advice.
13
1,449
TraderNick retweeted

Jun 12
4
40
4,930
TraderNick retweeted

Jun 11
Bin gespannt was für Häuser demnächst so auf den Markt kommen.
Die 10 und 15 jährigen Zinsfestschreibungen aus der Nullzinsphase laufen in den nächsten Jahren nach und nach aus.
Für ein Darlehen über 800.000€ hat man 2016 eine Rate von ungefähr 2100€ gehabt.
Die Restschuld beträgt heute (nach 10 Jahren) ca. 620.000€, wenn keine Sondertilgungen getätigt wurden.
Bei der Anschlussfinanzierung zu 4% steigt die Rate somit auf ca. 3300€ an.
Das ist nicht stemmbar für die meisten Familien in Deutschland.
#finanzen #immobilie #deutschland
155
61
880
146,281

Jun 11
$ABVX
ECG shows sudden sharp HR plunge from ~110 to critically low (cliff drop then slight recovery); suggests severe bradycardia, sinus pause, or conduction block (e.g. heart block).
concerning symptoms: dizziness, extreme fatigue.
Do immediately: If any symptoms → ER now.
12
2,568

Der feuchte Traum vieler Linken geht bald in Erfüllung, aber sie werden es hassen.
Bis zu 4.000 heutige und ehemalige SpaceX-Mitarbeiter könnten durch den Börsengang auf einen Schlag zu Millionären werden.
Nicht nur Manager, sondern auch Ingenieure, Techniker, Schweißer und viele andere Angestellte profitieren, weil sie über Jahre Unternehmensanteile erhalten haben.
Eigentlich müsste genau das der Traum vieler Linker sein: Arbeitnehmer werden am Unternehmenserfolg beteiligt und bauen Vermögen auf. Aber Vermögensaufbau und Millionen sind natürlich Toxisch für die Gesellschaft.
Ist dieser Schritt jetzt also gut oder böse? 🤔
118
137
2,630
86,406
Jun 9
No one is posting about the stocks, everyone will run their portfolio now through fable. Expect some extra volatility in the next hours until everyone executed his portfolio rebalancing.
64
Jun 9
The weird thing with $ABVX: normally the Ph3 readout is THE moment in a candidate’s entire lifecycle. It’s here. It’s de-risked. Efficacy is best in class…
And yet the main event is now the possible late-June update of safety in ph2 non-responders?!
6
1
36
7,131
Jun 8
Buyout announced why all corporate jets are in Ireland?
Seems like tracking jets isn’t very reliable…

$JNJ acquiring a pan-KRAS degrader via Firefly Bio for $1B
businesswire.com/news/home/2…
1
182

There is VERY likely to be multiple cancer cases in the $ABVX part 2 just based on pure statistics and the normal background rate. What matters is that they are explained by management this time, and compared to the normal rates seen in these patients and the rates the other drugs (with clean labels) also produce.
Management over-trusted the market to be able to interpret the original cases without any handholding.
5
2
48
13,236
Jun 7
Let’s not forget… there is another draft lingering in their CMS… $ABVX
ir.abivax.com/node/12346/htm…

3
20
6,197
TraderNick retweeted

Jun 6
Each circle has a different story

706
39,629
382,450
14,015,605
TraderNick retweeted

Jun 5
never waste a good crisis

1,086
3,185
66,556
3,215,160
Jun 3
How the obefazimod malignancy question will likely be handled under an EMA marketing authorisation for $ABVX (my area of experience lies there):
The scattered single-case malignancies almost certainly do not block approval.
1
2
24
3,037
Jun 3
Potential risk means: plausible enough to track, not proven enough to restrict labelling heavily.
That classification triggers routine pharmacovigilance plus, typically, long-term monitoring through post-authorisation safety studies (PASS) and registries.
1
1
276
Jun 3
In plain terms: the drug gets approved, and malignancy incidence is followed in the post-marketing setting and ongoing studies. This is exactly how the EMA handles immunomodulators with theoretical malignancy questions. It is a manageable, well-trodden path, not an approval risk.
3
247
Jun 2
Why the $ABVX obefazimod Ph3 maintenance malignancies are very likely not a drug-related signal (my view on reasons that count/ don’t count):
• Long-term Ph2 data is the strongest evidence. No malignancy concerns across Ph2b open-label extensions,
1
15
2,204
Jun 2
• Management seemed unprepared for the concern. Weak on its own, but you don’t walk in unprepared if something had been flagged internally.
What does NOT count:
• “44 weeks is too short for carcinogenesis” is wrong. The feared mechanism is impaired immunosurveillance allowing
1
4
247
Jun 2
existing malignant cells to progress, which can manifest faster.
• “25mg showed no cancers, so use the low dose” does not hold. A regulator won’t accept low-dose cleanliness as reassurance.They would assume the same risk could arise at 25mg with more patients and longer exposure
3
228