
Joined June 2019
- Tweets 85
- Following 90
- Followers 109
- Likes 146
13 Photos and videos













2 Apr 2021
💚⚾️ #SeaUsRise
2 Apr 2021

We wouldn’t be here tonight without the dedication and sacrifice from our frontline workers and healthcare heroes.
THANK YOU 💙

2
Ron Ron Cheng, MD retweeted

1 Feb 2021
@VMUrology is delighted to welcome Dr. Oriyomi Alimi from Yale University to our residency program! Yomi, we are thrilled to have you join the team! 👊👊👊@VirginiaMason

6
13
133
12 Dec 2020
Great time chatting with applicants yesterday for @VMUrology, both new and familiar faces! @amykupra @AbiRajasegaran @andrew_duchesne.
Fantastic day on the mountain 🎿🏔️
3
8
11 Sep 2020
Treating myself on call after two consecutive OR days without a proper lunch meal. 😁🌯💛
11
4 Sep 2020
Today I logged my 500th case since starting my R2 year @VMUrology last November. 🎉
Great time to reflect on a wonderful journey thus far and how blessed I was to be welcomed to the program by @KKseattle @Dr_UnaLee @Twillfull @Mrwailee @jkfrankel @awstamm @RPDonahue et al 😁✌️
1
1
29
30 Aug 2020
Love is my spouse instituting a study hour for both of us while I'm on home call. She is a paragon of a physician-to-physician partner 👩⚕️❤️
5
15 Aug 2020
Calling all future ballers 🏀🏀, shot callers 👩⚕️. Talk Monday or reach out on here anytime! ✌️
9 Aug 2020

@VMUrology residents are HAPPY🤗& they look forward to telling you why. Pls join them for HAPPY hour Mon 8/17 4pmPST to learn about our culture & the great training you will get in the amazing Pacific Northwest. TO REGISTER email Joytika.mala@virginiamason.org. @VirginiaMason
3
8 Aug 2020
Friday fun factoid: If I were a donor allograft in this pic, I would be one cool bean.
Unnamed moulin, Godwin glacier, outside Seward, AK
6
5 Aug 2020
Wednesday water wisdom:
Give a man a catheter, and his bladder will be empty for a day.
Teach a man to catheterize, and his bladder will be empty for the rest of his life.
What other adages/axioms are ripe for adaptation to urology?
3
2
25
Ron Ron Cheng, MD retweeted

5 Aug 2020
Impressive quick shot presentations for the 1st half of Round 2 #AWSResearchMadness! Thanks @WomenSurgeons for organizing & letting us share our work tonight. To those who registered for the event/vote, our project is in group 4! @jakaplan @ValSimianu @RonRonChengMD




1
3
9
2 Aug 2020
Sunday morning non-uromedical proclamation:
6/8 🎶 🎶 is the best time signature 🎼🎻 (disappointed that there are not bass clef and trombone emojis)
Change my mind 🤔
1
2
22 Jul 2020
Into my 7th year as some kind of resident taking primary call, and I've begun to appreciate the beauty in the overnight consult:
1. Educating/reassuring the patient during a stressful time.
2. Helping out another service with your expertise.
3. Doing the right thing.
1/
2
1
20
22 Jul 2020
I know it can feel overwhelming when you fall into a "me vs. universe" rut. The isolation can be very burdensome, at times too much to bear. Someone is always available; don't be too proud to reach out. We're all on the same team, and that team is a lot larger than you think!
3/
1
6
22 Jul 2020
Wrapping up:
Seek out the opportunity in the immediate challenge
Recruit patients/nurses/physicians/etc as allies in your quest to deliver excellent care
Ask for help. Vulnerability doesn't have to be a liability
And sleep when you can, but not at someone else's expense
4/4
8
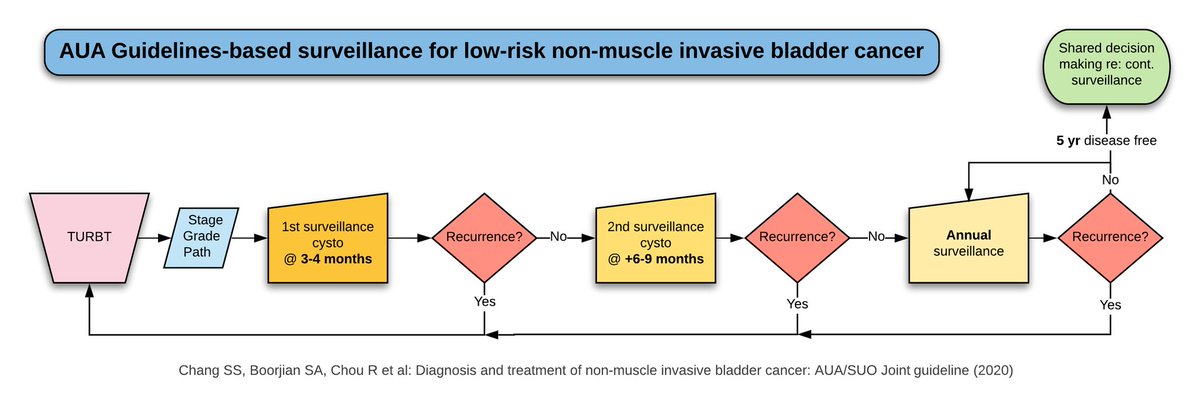
20 Jul 2020
While reading for academic day at Madigan, couldn't help but make this flowchart on surveillance recs for low risk NMIBC from AUA guidelines...because I am a huge nerd. Hope this helps someone/feel free to use for whatever! Feedback welcome 🧐 @jkfrankel @Ted_Wynne @VMUrology
3
2
19
20 Jul 2020
To close the loop, low risk includes a single low grade Ta lesion less than or equal to 3 cm in size, as well as papillary urothelial neoplasm of low malignant potential (say that 5 times fast?)
3
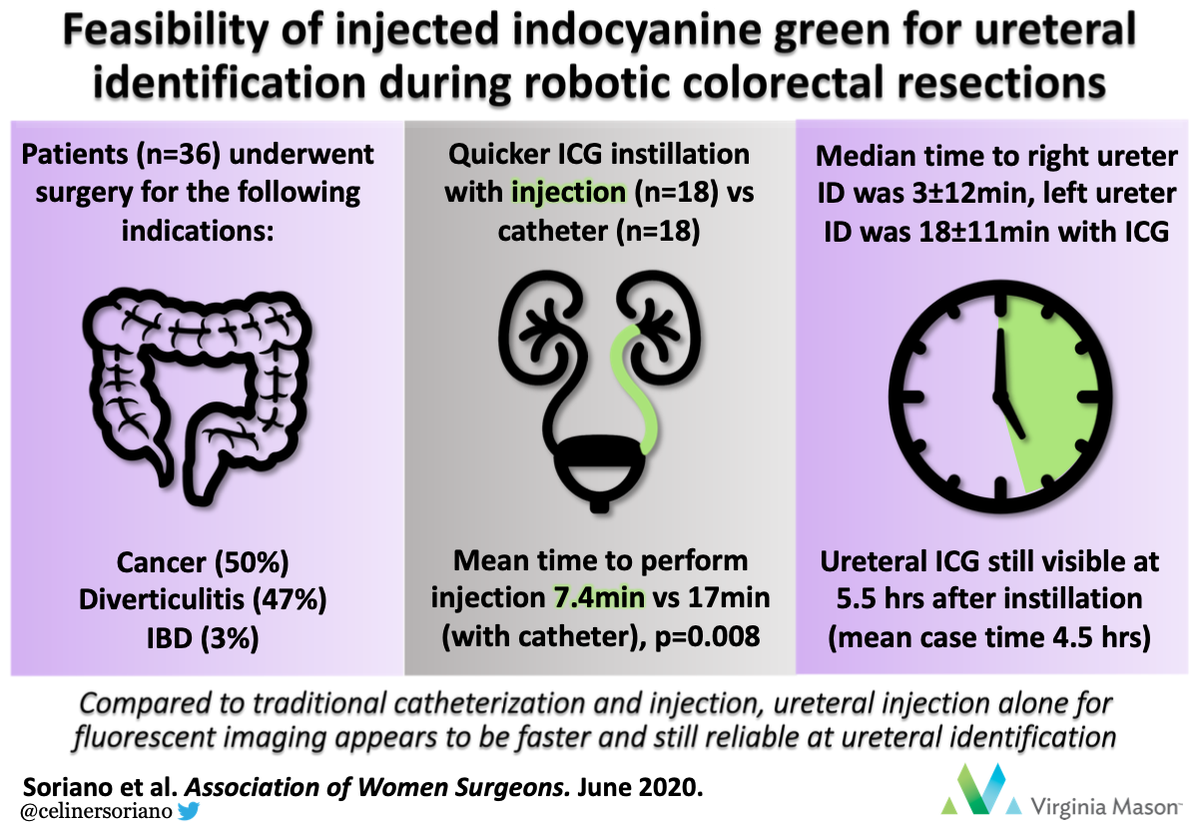
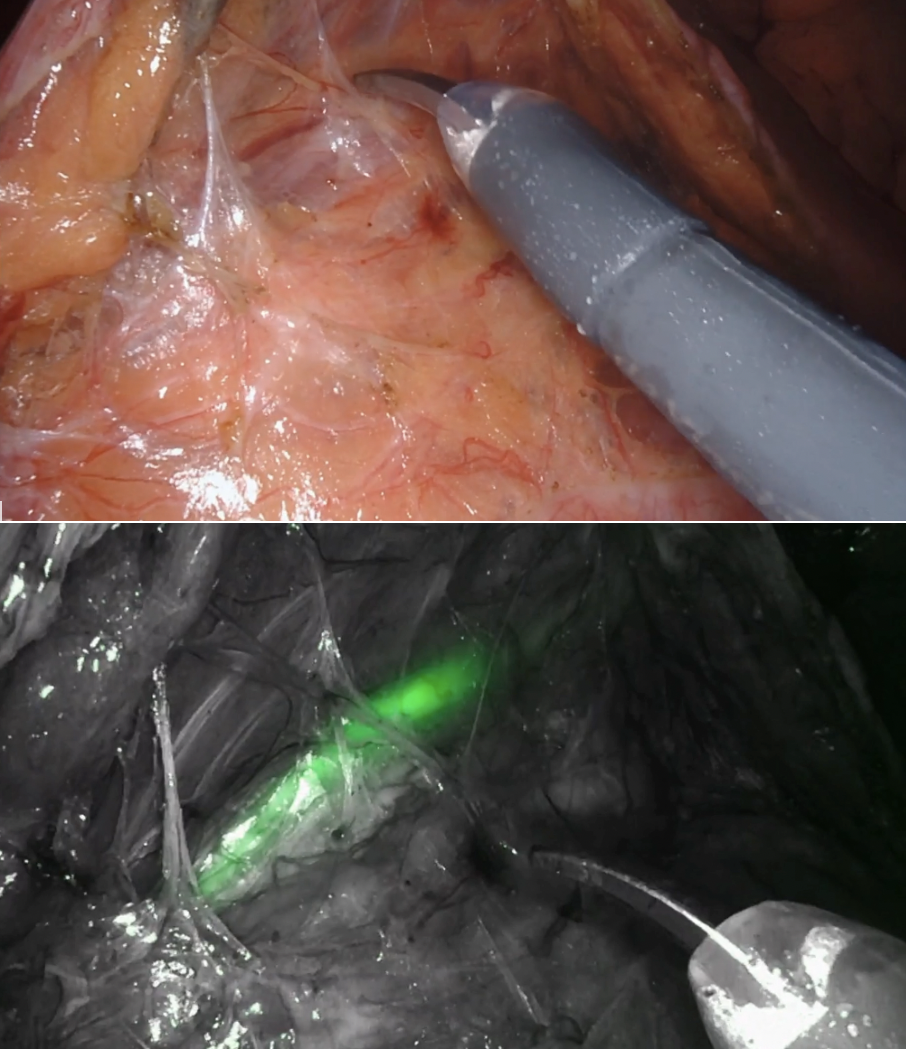
14 Jul 2020
Voted! Happy to be a part of this project; estimated particpation in 30 stent cases this past year, many using ICG. ICG w/o stents is super slick, and the abstract speaks for itself. Let's keep up the multi-disciplinary effort to push the envelope! @RPDonahue @awstamm @Twillfull
14 Jul 2020

Grateful to be among 73 amazing abstracts. Check out & vote for cohort 1, group 5, abstract #11 (my 1st visual abstract!) Our colorectal surgery dept collaborates w/ @VMUrology as we show our experience of ureteral ICG w/ and w/o stents. @jakaplan @ValSimianu @RonRonChengMD
1
6