
GOD, Family and Country are my priorities and in that Order. Inactive U.S Marine, Semper Fi
Joined April 2022
- Tweets 3,701
- Following 1,910
- Followers 1,426
- Likes 7,444
1,136 Photos and videos



Pinned Tweet

19 Nov 2025
@BearGrylls @MiracleSeries Faith of a 9 year old to be healed from cancer and healing it was, incredible. Jesus still heals today as he did in Biblical days, Faith is real, prayer is real. This story is just one of many you see on the new Miracles series on the Angel Network. As Natalie Grant was singing live with her social media platform during COVID she responded to a comment made with a song she would sing called "Miracles", she asked all who watching too pray, the boy being prayed for got a huge pray chain and was healed during the song and instantly. You literally see what looks like a Angel ORB in the video. This was LIVE for all to see. Also, recommend a great read by Lee Storbel, numerous documented miracles there. Here is a link to watch this episod Free on Facebook. #JesusHeals #Miracles fb.watch/DtImORI3pf/
2
15
2,389
Jun 12
$NWBO @MHRAgovuk @NBTStweets @AlMusella @braintumourrsch
MHRA, you need to do better based on your standard timelines you shoot for. You have exceeded your own set timelines by a factor of 4. GBM patients such as shown here has to raise funds to extend or sometimes even cure the Brain Cancer.
Jun 12

1
17
73
2,501
Jun 12
Tale of the tape today. Up 7.1% almost 3 Million Shares, 600K traded last 15 minutes. Low of .1850 and High almost right at close of .2004 Chart below is a Weekly Chart, last time we sat above $1 was 9/24/2023.
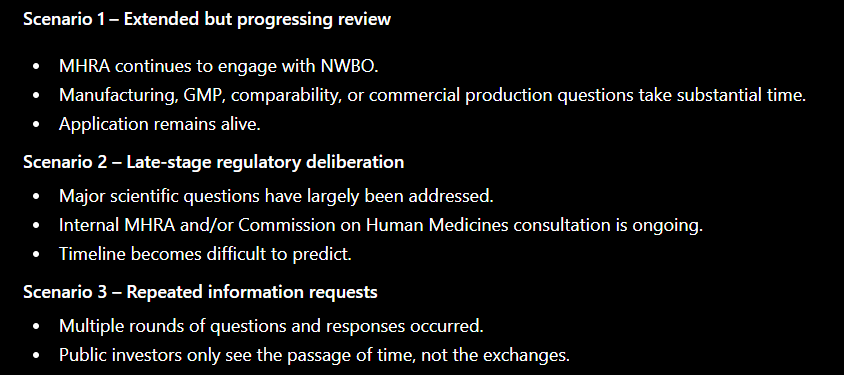
My take going into the weekend after question and answer sessions with MHRA: For sure there will be no more of my time wasted on potential timelines and apologize for any timelines I tried to come up with. Guidance from MHRA on 150, 210 days it does not matter, MHRA is on their own timelines, there is no oversight. Guidance is just that, they are made up standards they hope to follow but rarely do. They pause,stop, start, extend as needed. That is exactly what they told me today which makes perfect sense being at 870 Post Validation days. Decision on approval will come when they are good and ready after they run out of questions for NWBO to answer. Case in point is the 2.3 years it took to approve a drug already approved in other countries I noted from research from the CHM minutes. Blame it on backlogs, Covid or what ever, does not matter, timelines IMO are a farce.
Trying to make a educated guess on timelines is futile.
6
4
43
1,758
Jun 12
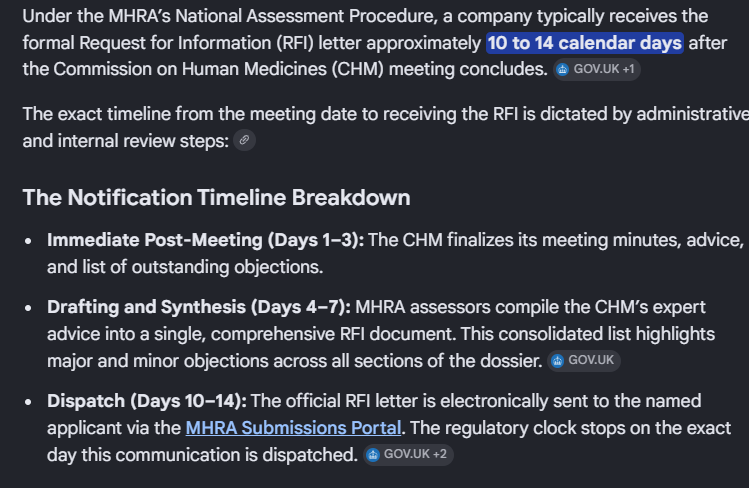
$NWBO Here is a question sent to MHRA regarding timelines for Marketing Authorisations. Based on this all and any specific clock stop on and off time lines etc can be thrown out the Window IMO. That would explain why we are at 870 days post Validation and counting, this is no real time clock to adhere to, other than target service standards which are never met as we can clearly contest. Who knows how many pauses, clock stops, precedural steps we have had along the way.
Question to MHRA:
From: xxxxxxxxxxxxxxxxxxxxxx Sent: 11 June 2026 17:00 To: MHRA Customer Services <MHRACustomerServices@mhra.gov.uk> Subject: CEC 258168 Guidance on the MHRA's national assessment procedure for marketing authorisation applications.
Hello
There is a MHRA marketing assessent now at 869 days Post Application Validation. I am trying to figure out based your own Guidance on the MHRA's national assessment procedure for marketing authorisation applications how a application could still be at 869 days even with possible 3 RFI's
Reference: CEC 258168
Dear xxxxx,
Thank you for your email.
MHRA does not publish assessment timelines for individual applications, and external parties cannot know how many clock‑stops, pauses, or procedural steps have occurred. The timelines in the national procedure guidance are target service standards, not maximum durations.
We hope you find this information helpful.
Kind regards,
Aaron
MHRA Customer Experience Centre
Communications and engagement team
gov.uk/guidance/national-ass…
8
1
48
5,409
Jun 10
DCVax-L has been under MHRA review for 868 calendar days since validation (Jan 24, 2024). Even assuming the maximum standard MHRA clock-stops (12 months total), the application appears to have accumulated roughly 500 active days—well beyond the 150-day accelerated review target. The reason for the extended timeline has not been publicly disclosed by MHRA or NWBO. $NWBO @MHRAgovuk
DCVax-L MHRA Timeline Analysis
📅 MAA submitted: Dec 20, 2023
📅 MHRA validation accepted: Jan 24, 2024
As of June 10, 2026:
• 868 calendar days have elapsed since validation.
MHRA's published National Assessment Procedure allows clock-stops for Requests for Information (RFIs):
• First RFI: up to 6 months
• Second RFI: up to 3 months
• Third RFI: up to 3 months
Even assuming the MAXIMUM standard clock-stops (~12 months total), DCVax-L would still appear to have accumulated roughly 500 active elapsed days since validation.
The timeline is significantly longer than a simple 150-day accelerated review. This suggests the process likely involved substantial clock-stops, manufacturing/GMP readiness activities, regulatory interactions, or other review elements not publicly disclosed.
Importantly, the length of review alone does NOT indicate approval or rejection. Publicly available information confirms the application was validated and remains under MHRA review.
9
3
59
3,141
Jun 12
There is extended clock stops past 3 months per MHRA in special cases, seems we must be very special then.
1
78
Jun 11
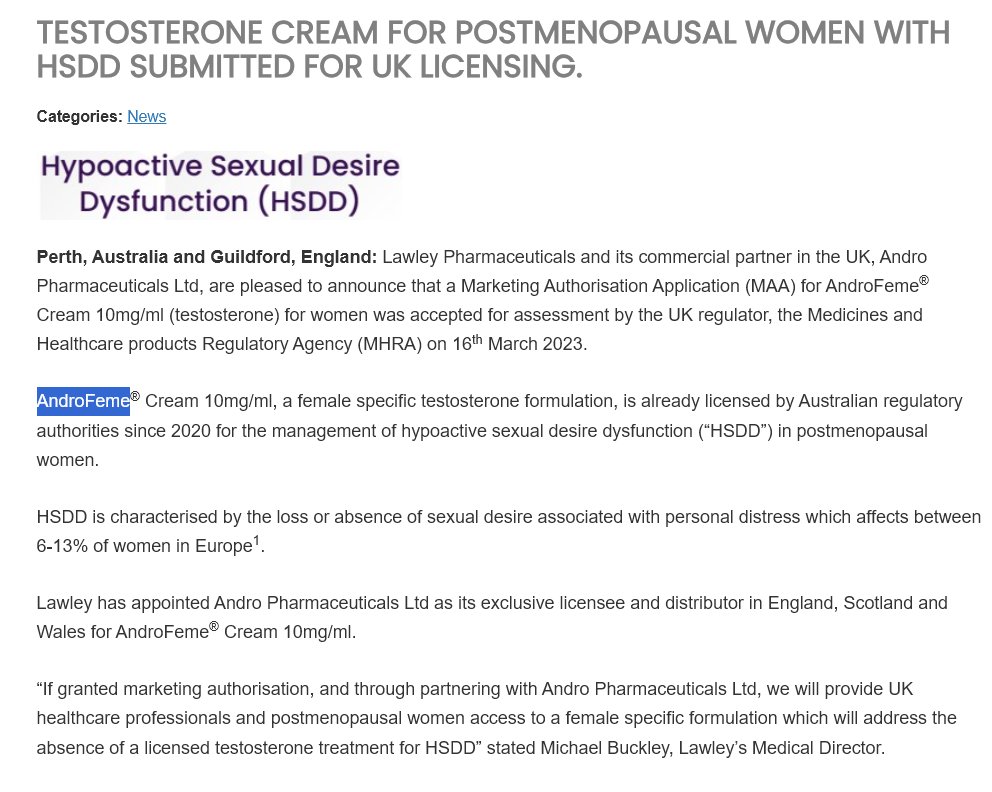
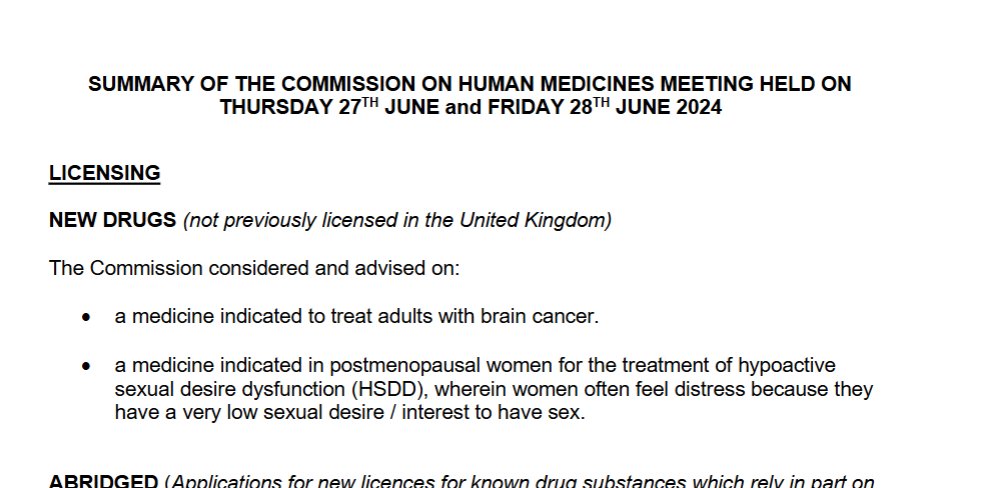
$NWBO Here is an example of MHRA approval, this drug was mentioned in June Licensing minutes in which we speculate DCVAX was too. This HSDD drug submitted there application March 2023, gets mentioned in CHM Minutes I speculate based on HSDD, then approved in late July of 2025, 2.3 years after submission. Plus this drug was already approved in other countries. So maybe its not crazy we are 869 days out post validation for MHRA, remember all the supposely backlogs especially during posg COVID etc.
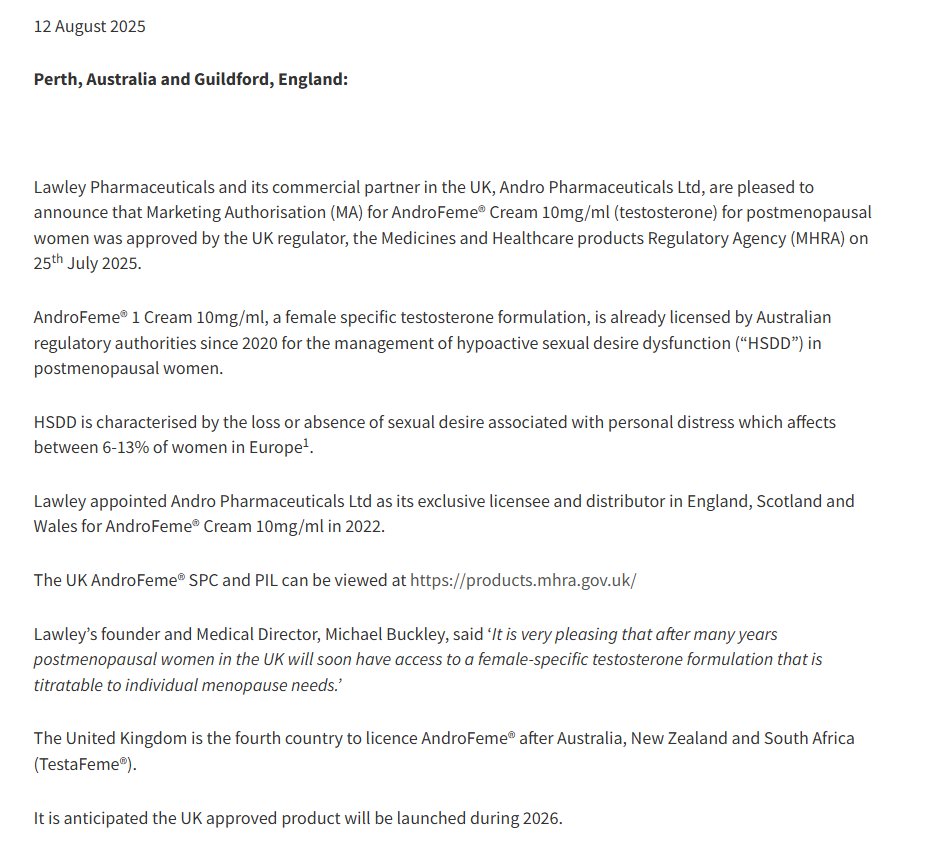
2
5
71
2,166
Jun 11
Take way the 90 days and that leaves June 26th, rechecking MHRA Guidance seems to indicate 210 days total.
Jun 11

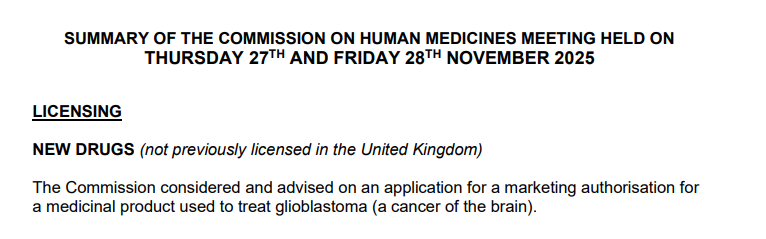
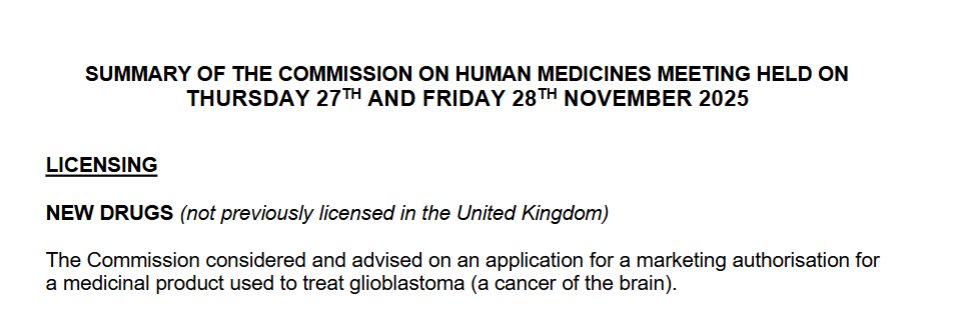
$NWBO Here is the two CHM Minutes where Licensing and Brain Cancer mentioned. Whether this the first and second RFI is my main focus point. If the second RFI was indeed 11/28/2026 NWBO had 3 months to respond at this time of clock stop, then MHRA has up 210 days to make the final decision on approval. (Total of 300 days, 3 months 210) If necessary a third RFI would be sent to resolve any final minor outstanding issues and switch off the clock again up to 3 months plus 210 days or 300 days max for approval decision.
If we did get an RFI Nov 28th of 2025, max decision with no 3rd RFI would be 09/24/2026. 90 days ended FEB 25th, 2026. So MHRA is in decision mode of either 3rd RFI or a final decision by end of September at the latest is my estimation assuming second RFI November 28th, 2025.
I have question in now about time frame in general to MHRA, I am not mentioning DCVAX by name, I want to know how an application can go 869 days without a decision based on their on guidance here. gov.uk/guidance/national-ass…
2
1
22
1,250
Jun 11
$NWBO Here is the two CHM Minutes where Licensing and Brain Cancer mentioned. Whether this the first and second RFI is my main focus point. If the second RFI was indeed 11/28/2026 NWBO had 3 months to respond at this time of clock stop, then MHRA has up 210 days to make the final decision on approval. (Total of 300 days, 3 months 210) If necessary a third RFI would be sent to resolve any final minor outstanding issues and switch off the clock again up to 3 months plus 210 days or 300 days max for approval decision.
If we did get an RFI Nov 28th of 2025, max decision with no 3rd RFI would be 09/24/2026. 90 days ended FEB 25th, 2026. So MHRA is in decision mode of either 3rd RFI or a final decision by end of September at the latest is my estimation assuming second RFI November 28th, 2025.
I have question in now about time frame in general to MHRA, I am not mentioning DCVAX by name, I want to know how an application can go 869 days without a decision based on their on guidance here. gov.uk/guidance/national-ass…
6
6
69
4,771
Jun 11
So after reading the guidance again it looks like 210 days total, not 210 plus the 90 days we have to respond, so take 90 days away from 9/24/2026 and that leaves JUNE 26th! assuming again 2nd RFI recieved in NOV of 2025 and no 3rd RFI recieved.
1
22
431
Jun 11
If June y26th comes and goes with nothing then no second RFI from CHM meeting minutes? Who knows at that point. Again I am just putting out there something to hang our hats on based on what information we uncover. Some say misinformation, its not misinformation if your statement begins with IF, I have no certainty on anything unless officially from a PR etc. unlike Court filings which are FACTS. We could all just shutup and take beating be okay with it, I have to much invested to do that.
1
1
14
407
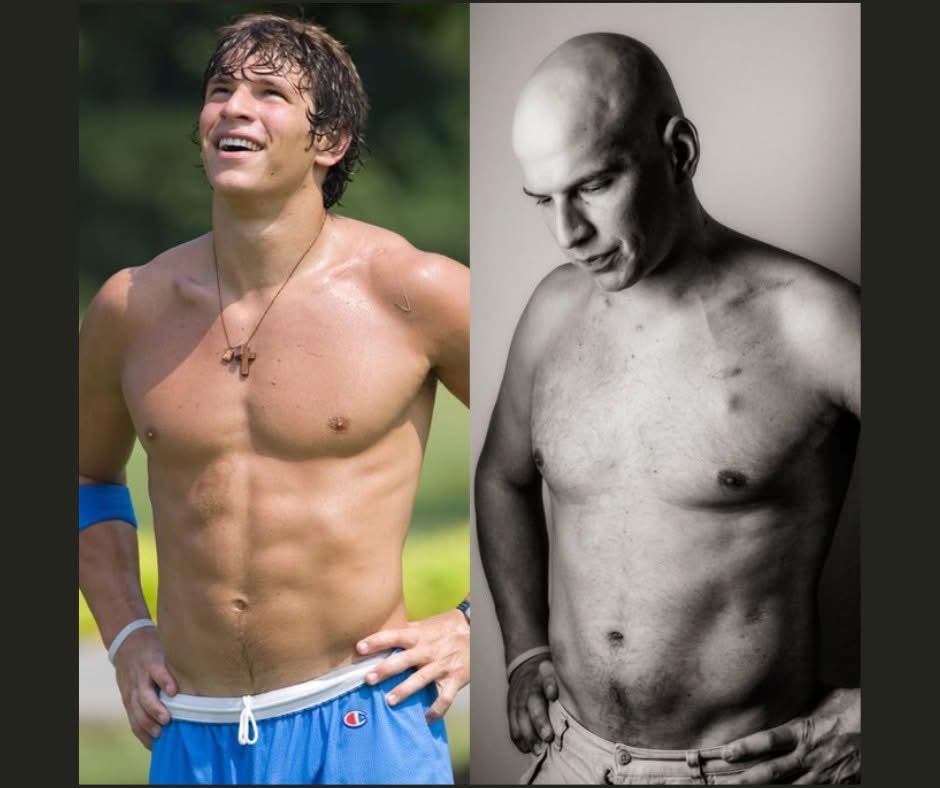
What a story, curing his own disease with a drug approved for something entirely different.

In the summer of 2010, David Fajgenbaum was everything a young man could hope to be.
He had been a Division I college quarterback. He spoke multiple languages. He was in his third year at one of America's top medical schools, the University of Pennsylvania. He had his whole life mapped out in front of him.
Then his body turned on him.
Almost overnight, his organs began failing. His lymph nodes swelled. He was exhausted beyond anything he had ever felt. Within days, he was rushed to the emergency room. Weeks of testing followed. Finally, doctors gave it a name: Castleman disease — a rare and catastrophic condition where the immune system attacks the body's own organs.
There was no cure. There was barely a treatment.
A priest came to his hospital room and read his last rites.
David said goodbye to his family.
Then, somehow, an aggressive round of chemotherapy pulled him back from the edge.
But it didn't hold. Within three years, he collapsed again. And again. And again. Five times in total, he came to the edge of death. Five times, chemotherapy bought him a little more time.
After the fifth collapse, his doctors sat with him and said the words no patient wants to hear: his body had received the maximum amount of chemotherapy a human being can survive. If he relapsed again, there would be nothing left to give him.
He would die.
Most people, hearing that, would have spent whatever time remained saying goodbye.
David Fajgenbaum picked up a medical journal.
From his hospital bed, between treatments, he began doing something no patient had ever done before — systematically studying his own disease with the full knowledge of a trained physician. He analyzed thousands of pages of his own medical records. He tested his own blood samples, looking for patterns invisible to everyone else because no one else had both the data and the desperate motivation to find them.
And he found something.
In his lymph node samples, a specific protein signaling pathway called mTOR was firing at abnormally high levels — essentially sending the immune system into a frenzy that destroyed his own organs. It was a clue no one had spotted because no one had looked in quite that way before.
Then he searched for something that could stop it.
He found it in an unlikely place: a medication called sirolimus, already approved and available, commonly used to prevent organ rejection after kidney transplants. No one had ever tried it for Castleman disease. But on paper, its mechanism was a near-perfect match for what David had found in his own blood.
Under his doctor's supervision, he began taking it.
Within days, his symptoms vanished.
Not improved. Vanished.
The man doctors had given up on walked out of the hospital. He finished medical school. He married his girlfriend Caitlin. He became a father. He became one of the youngest faculty members ever to receive tenure at Penn Medicine.
And then he turned around to face everyone still waiting in the dark.
He founded the Castleman Disease Collaborative Network, building the first global research effort for a disease that had none. He launched Every Cure — an organization that uses artificial intelligence to search all existing approved drugs for hidden matches with diseases that currently have no treatment. The idea is simple and revolutionary: there are over 1,500 approved drugs in the world and over 7,000 diseases with no treatment. The cures may already exist. They just haven't been matched yet.
Over 15 years, Fajgenbaum and his partners have helped advance 28 repurposed drugs — 14 directly led by him. MedicalXpress
A priest once came to read him his last rites.
Today, David Fajgenbaum has authored over 100 scientific papers, appeared on TIME's list of the world's most influential people in health, and continues to take his small sirolimus tablet every single morning the pill he found himself, in the darkest room of his life, when no one else was looking.
He didn't wait to be saved.
5
446
$NWBO Here is further evidence from MHRA on CTBVEAG Minutes and any reference to licensing.
I asked to further clarification regarding Licensing statements in the CTBVEAG minutes, this should close the door now on this subject and will be the last I reference it.
"To clarify, CTBVEAG does not provide advice on Marketing Authorisation (MA) or new product licensing. Its role is confined to reviewing scientific and clinical trial matters. When the minutes refer to “licensing”, this reflects only the fact that data generated from a clinical trial may ultimately form part of a future MA submission. This type of contextual reference is not an assessment of approvability, nor is it advice on licensing requirements or regulatory outcomes"
3
5
77
3,456
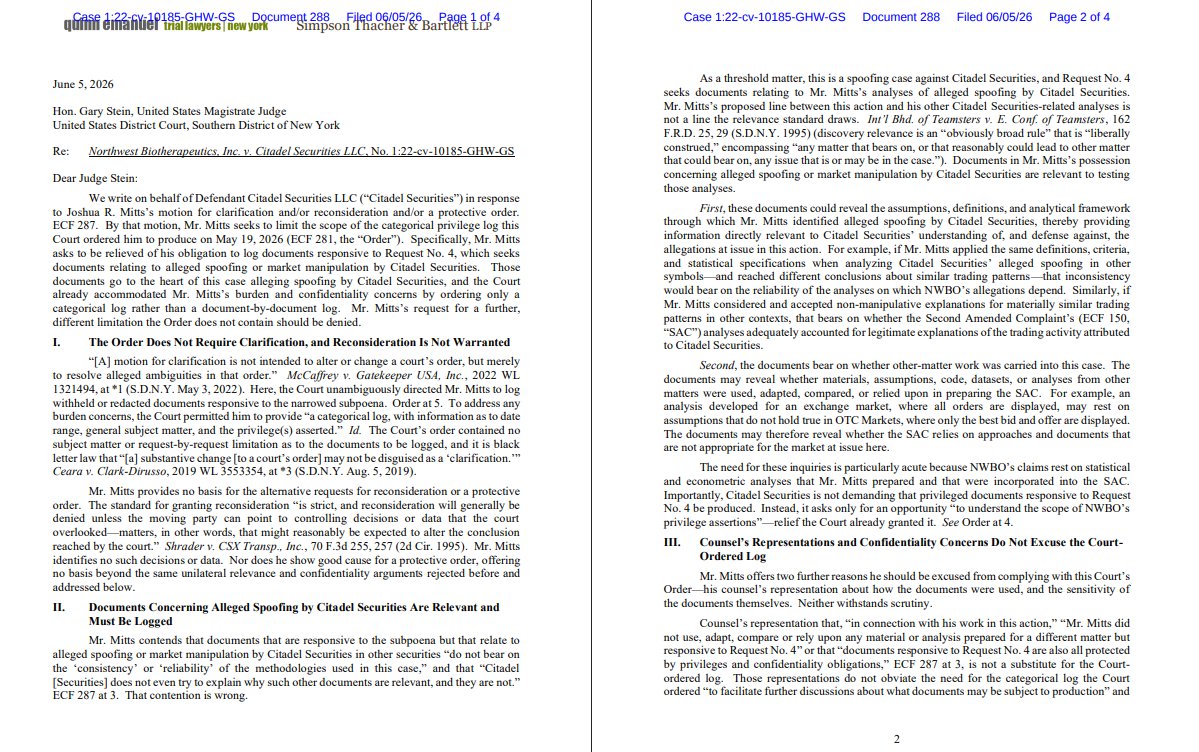
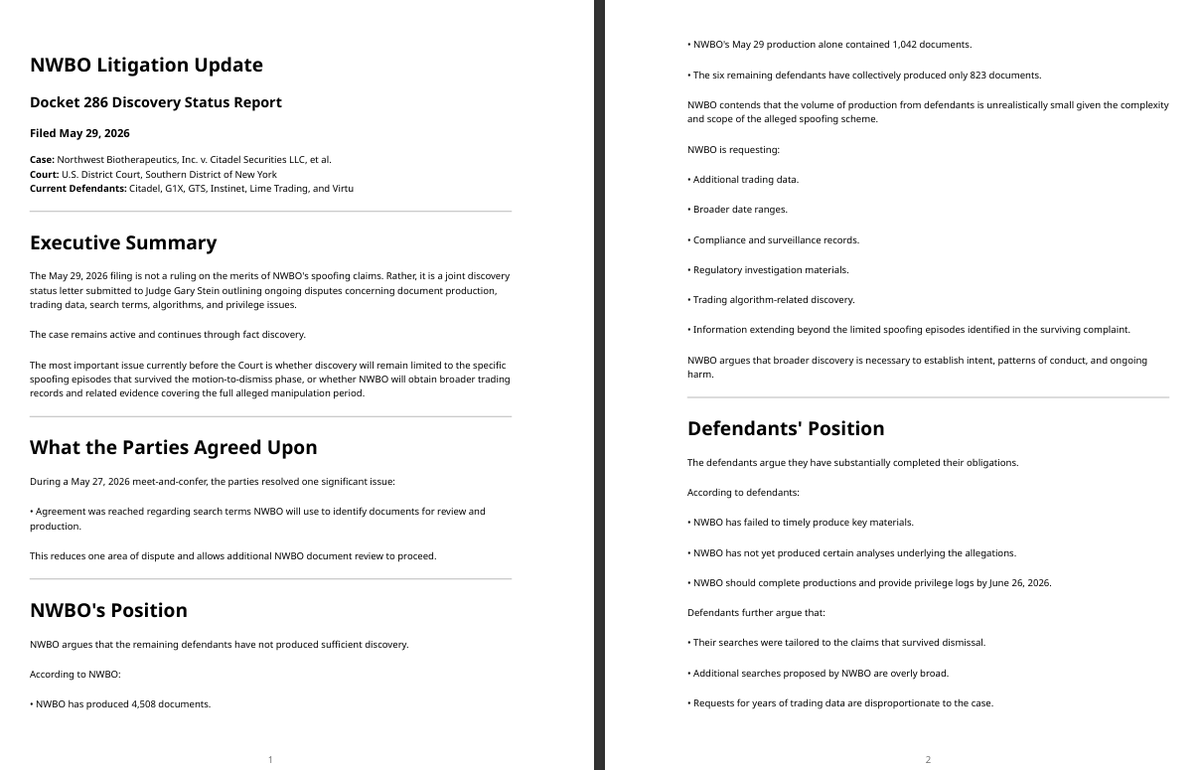
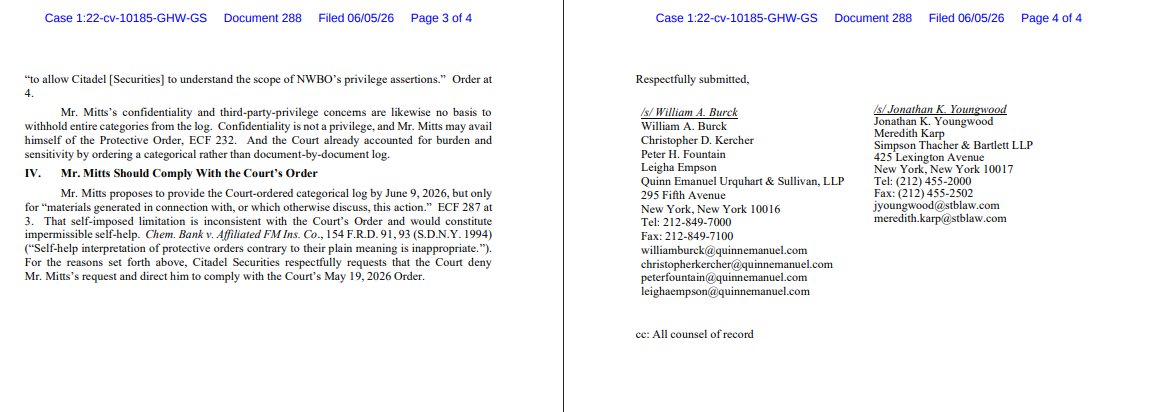
$NWBO LETTER addressed to Magistrate Judge Gary Stein from William A. Burck dated June 5, 2026 re: Response to Joshua R. Mitts's Letter at ECF 287 . Document filed by Citadel Securities LLC..(Burck, William) (Entered: 06/05/2026)
The key question now is whether Judge Stein:
Orders Mitts to provide the broader categorical log sought by Citadel; or Accepts Mitts's narrower interpretation.
6
1
56
3,698
$NWBO Okay, I have new information from MHRA regarding all the November 2025 CTBVEAG and CHM discussion. Based on this email I got today my thoughts now changed since the Licensing section of CTBVEAG according to "MHRA CTBVEAG provides expert advice on clinical trials only. They do not advise on licensing decisions, approval likelihood, or pre‑CHM positions. Any references to licensing in their discussions relate only to the context of clinical development, not to Marketing Authorisation assessment." My initial bias was all based on Licensing and CTA as two different processes within the meeting minutes, now that has been cleared up it seems only the CHM minutues was possibly relevent to DCVAX. I have no issue going back on my initial discussion if I find out additional details to warrant so. Hope this helps investors with that long discussion over last few weeks.
10
9
123
7,734
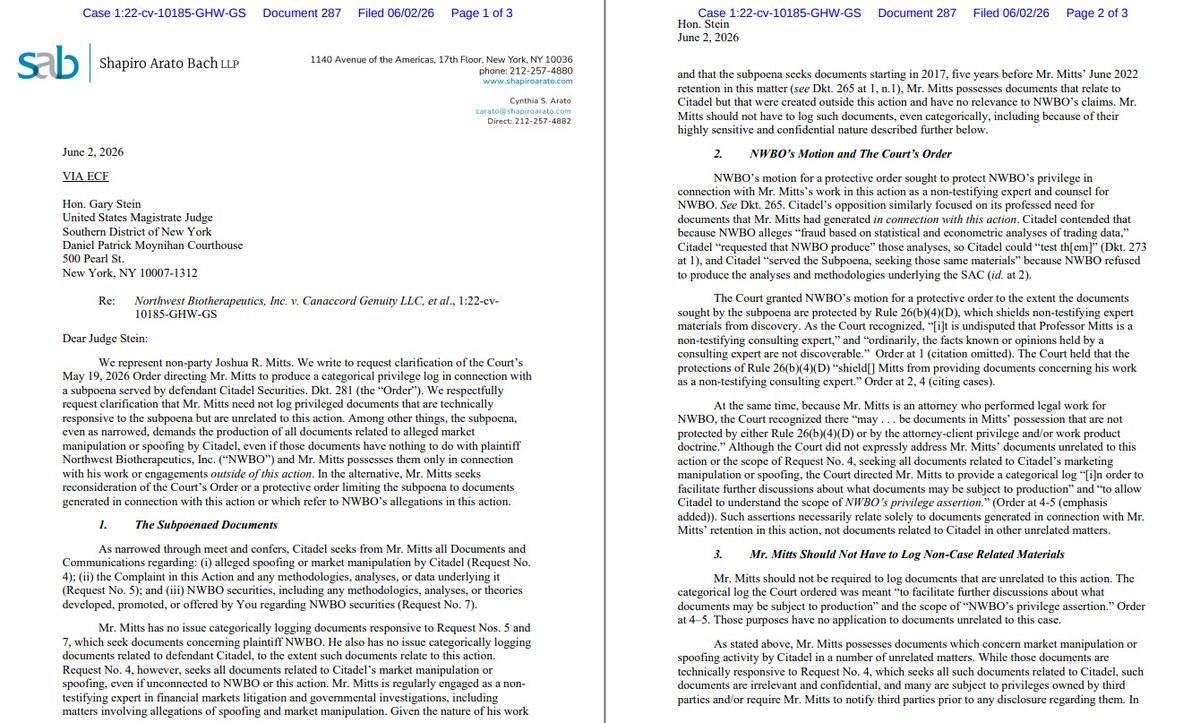
$NWBO New Dockets on Mr Mitts. Docket 287 is essentially Mitts telling Judge Stein:
"I will log NWBO-related materials as ordered, but I should not have to identify or disclose privileged documents from completely unrelated cases involving Citadel."
Mitts explicitly tells the Court:
He did not use, adapt, compare, or rely upon analyses from other matters when performing work related to NWBO.
3
4
83
2,459
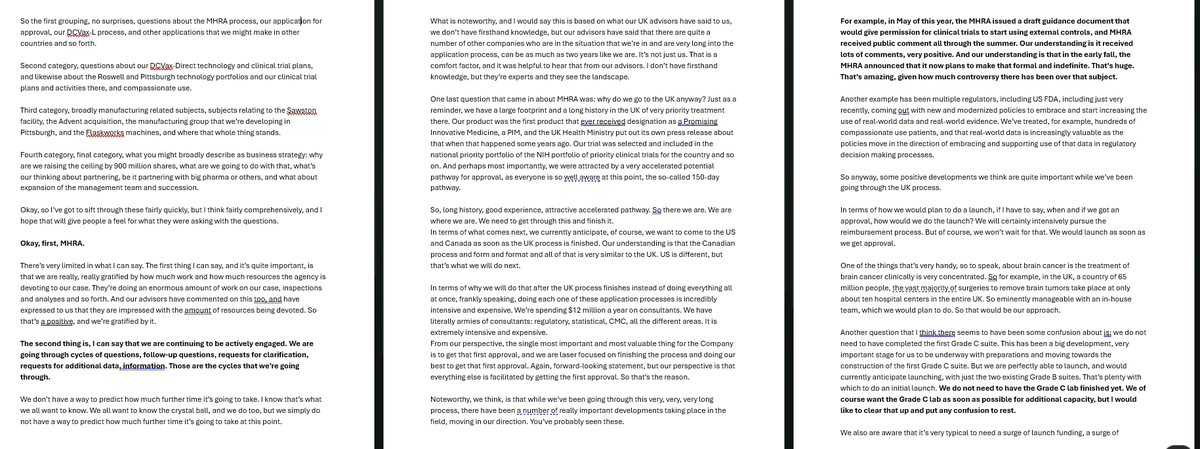
$NWBO Here is the annual shareholders meeting transcript which I thought I would go through again since this was after the CTVBEAG/CHM Meeting at the End of November 2025. I Highlighted some points of my own interest. So NWBO would have known at this point any items they needed to address from the meetings. I removed beginning conversations about proxy and legal stuff.....
2
2
56
3,122