
Thunder Bay ED Ornge MD, luv Airway CRM MedEd Tech 3D OpinionsOwn TweetsNotMedicalAdvice RetweetsNotEndorsing airwayNaUT airwayNautics.com
Joined November 2012
- Tweets 32,605
- Following 491
- Followers 3,659
- Likes 14,270
4,559 Photos and videos







Pinned Tweet

28 May 2023
I keep trying to remember (but paranoid I might forget) to talk directly to patient (same as when they might be awake), when they present with what seems to be GCS 3 especially when I am stressed/distracted by them being critically ill or injured
1
4
1,724

11 Nov 2025
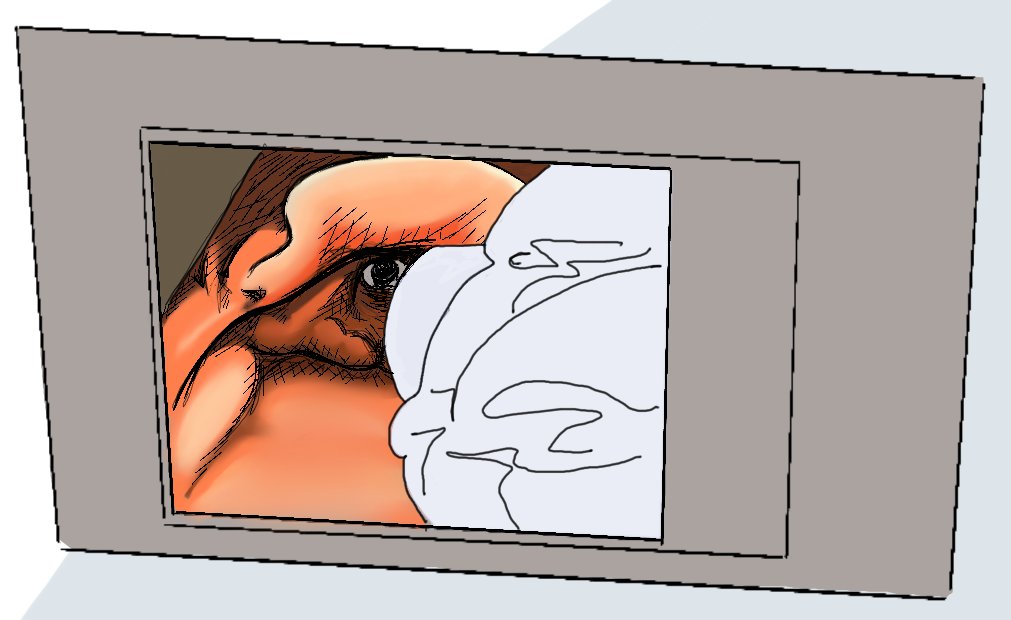
Lighten up Vader!
Keep your laryngoscope hold fingertip light, low with inward elbow
patreon.com/posts/53118288
1
80
11 Nov 2025
Start with light fingertip laryngoscopy, holding VL or DL SG or HA blade with a choked up grip and just deploy whatever blade length is needed. More precision to blade tip movement with your fingertips holding base of blade versus being high up on handle.
2
1
243
11 Nov 2025
11 Nov 2025

Start with light fingertip laryngoscopy, holding VL or DL SG or HA blade with a choked up grip and just deploy whatever blade length is needed. More precision to blade tip movement with your fingertips holding base of blade versus being high up on handle.
1
128
11 Nov 2025
Less force and strength is required so the intubator's hand does not fatigue. Also only moving a few pounds of tongue and soft tissue. Light exploratory force allows one to find sweet spot, see how tissue responds. Is a technique of millimeters and degrees of gentle exploration.
1
98
11 Nov 2025
Too much force locks tissue in place and does not allow sweeping and clearing for view or tube delivery space. Force applied in the wrong direction and spot will not improve things no matter how much strength is used and only serves to traumatize airway and panic operator.
1
44
Yen Chow retweeted

8 Nov 2025
Occasional intubators also sadly intubate the oesophagus too often
- I recently reviewed a paper describing occasional intubators in a high resource setting, with a >10% oesophageal intubation rate (many unrecognised).
1
1
2
140
Yen Chow retweeted
8 Nov 2025
I’ll gently push back
VL is an intrinsically better technique
It improves laryngeal view, first pass success, reduces failure, force, trauma and complications (26,000 patients in Cochrane r/v with another 20,000 waiting to be added)
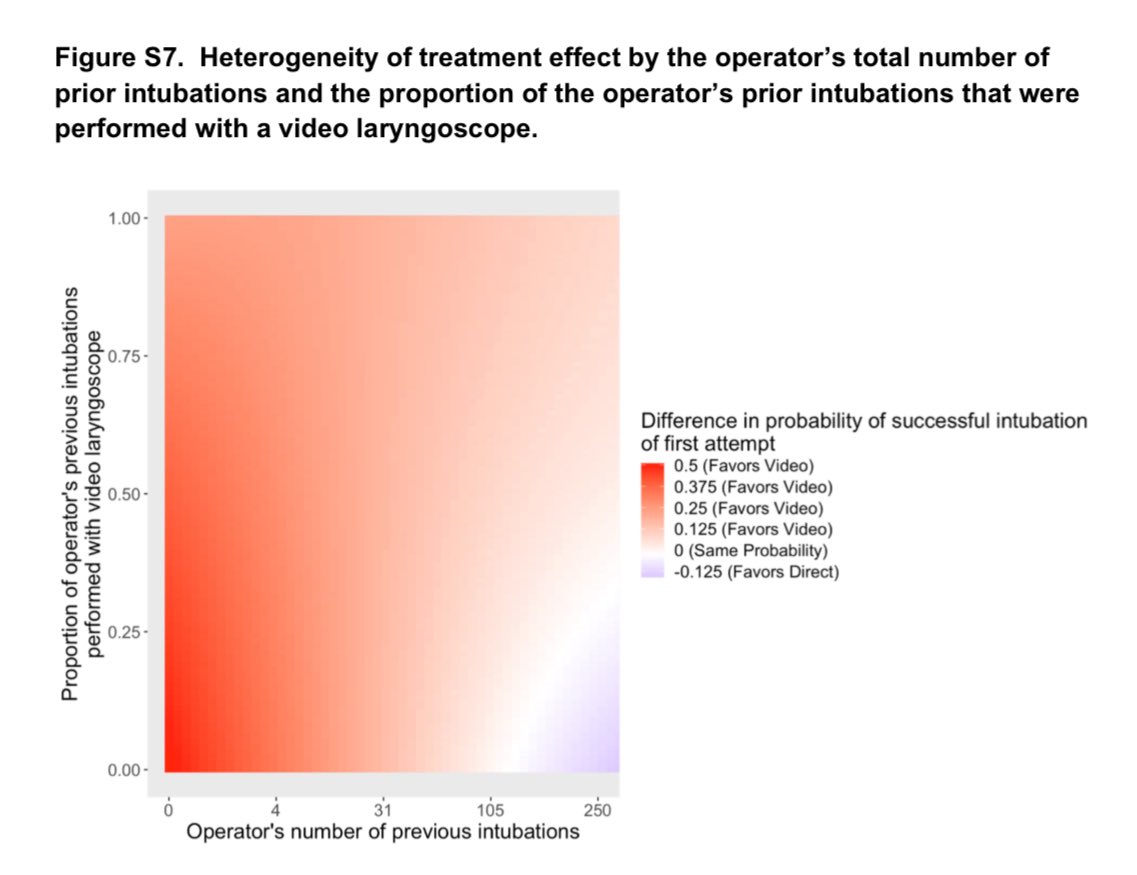
In Prekker’s DEVICE study this nice supplementary graph showed how VL benefited every intubator except those with lots of experience with DL but little or no VL experience (who one might characterise as “laggards” in terms of adoption)
nejm.org/doi/suppl/10.1056/N…
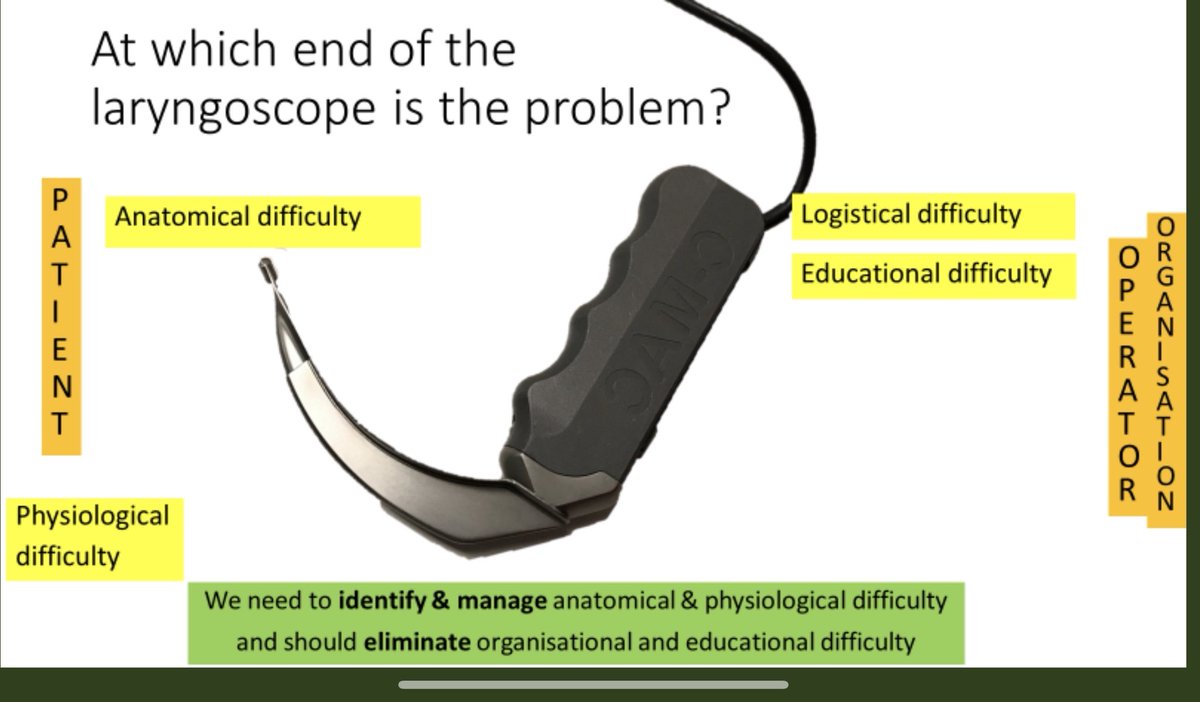
That said - clinicians should not be undertaking high risk procedures (intubation fails dangerously) without appropriate training…..which brings us back to “the educationally difficult intubation”*
Yes I’m resisting talking about tools with tools 😊
1
1
3
133
Yen Chow retweeted
8 Nov 2025
Anaesthetise
Paralyse
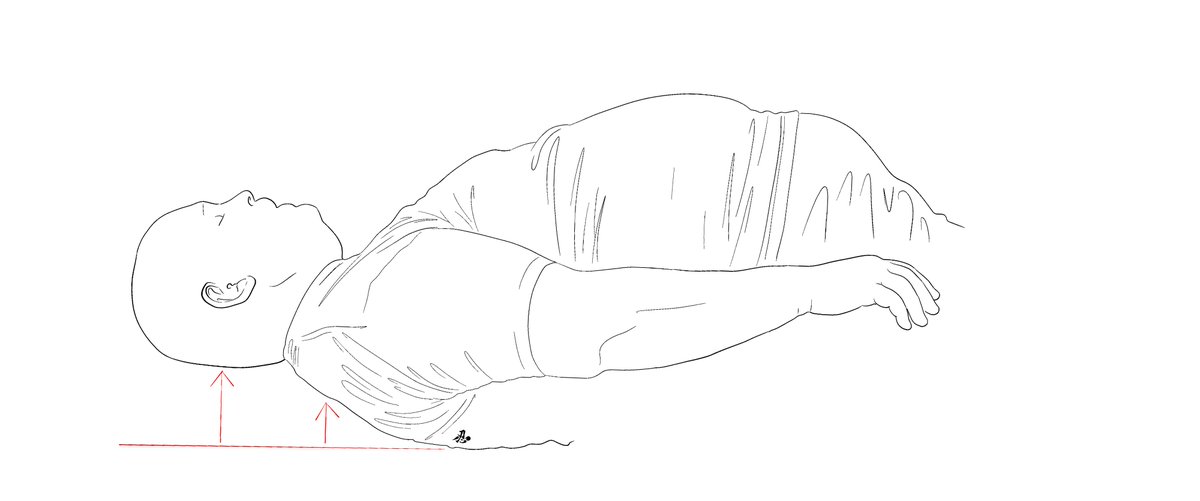
Put the head and neck in the sniffing position (flextension)
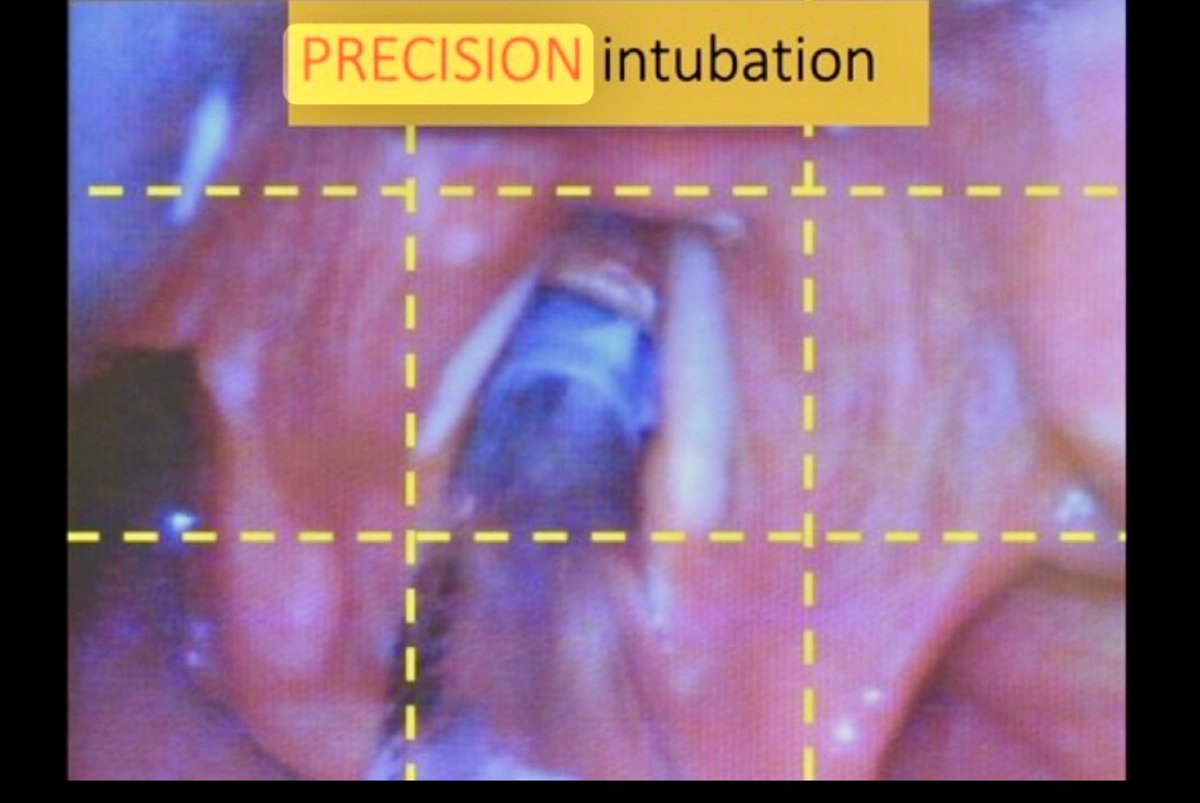
Get a good view (middle of the middle)
Slide a suitably small tube (6.0-6.5 mm ID for adults) along the blade into the trachea
And along the trachea (which is correctly aligned by flextension)
It’s not too tricky
2
1
3
251
Yen Chow retweeted

8 Nov 2025
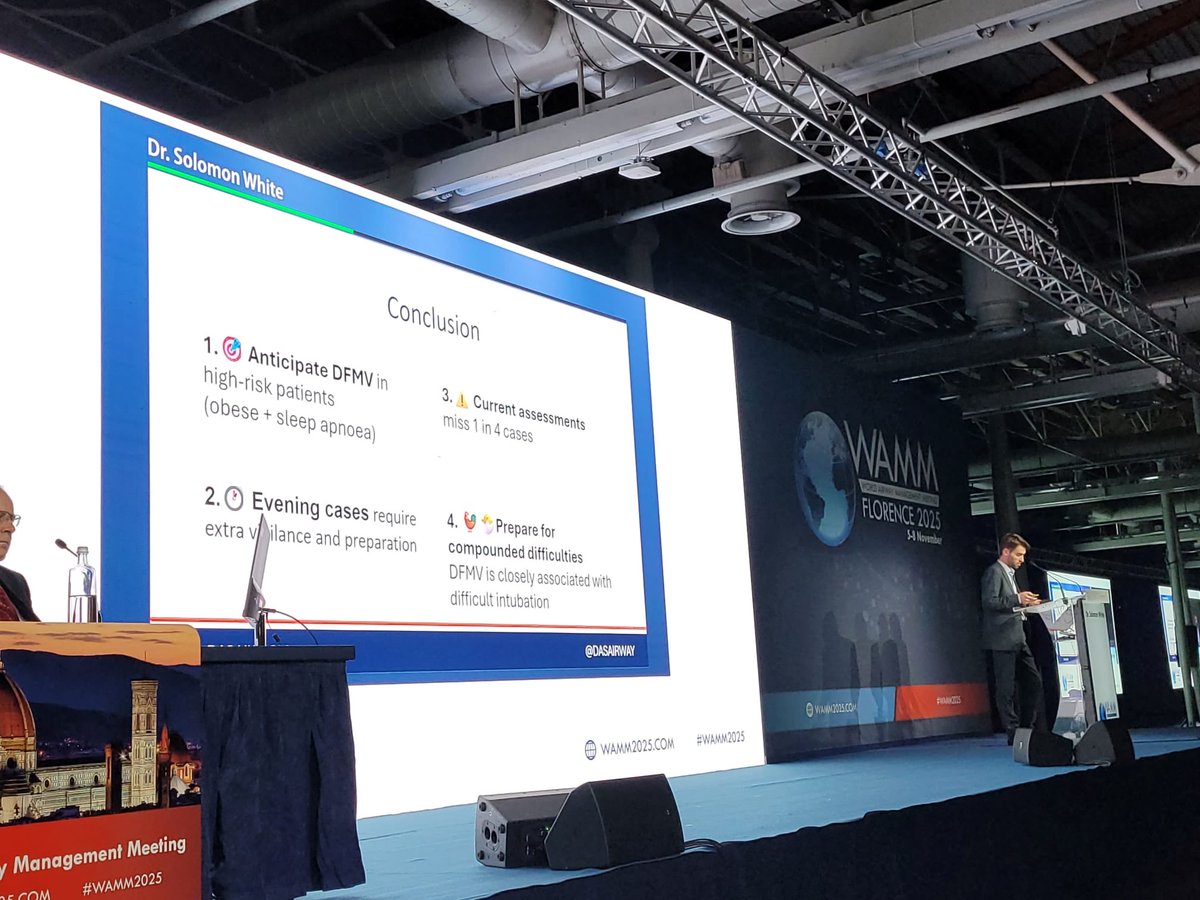
Difficult Face Mask Ventilation! An excellent presentation by Dr Solomon White (WSOA) @WAMM2025 #WAMM2025 #DAS #DASRegistry

1
6
471
Yen Chow retweeted

8 Nov 2025
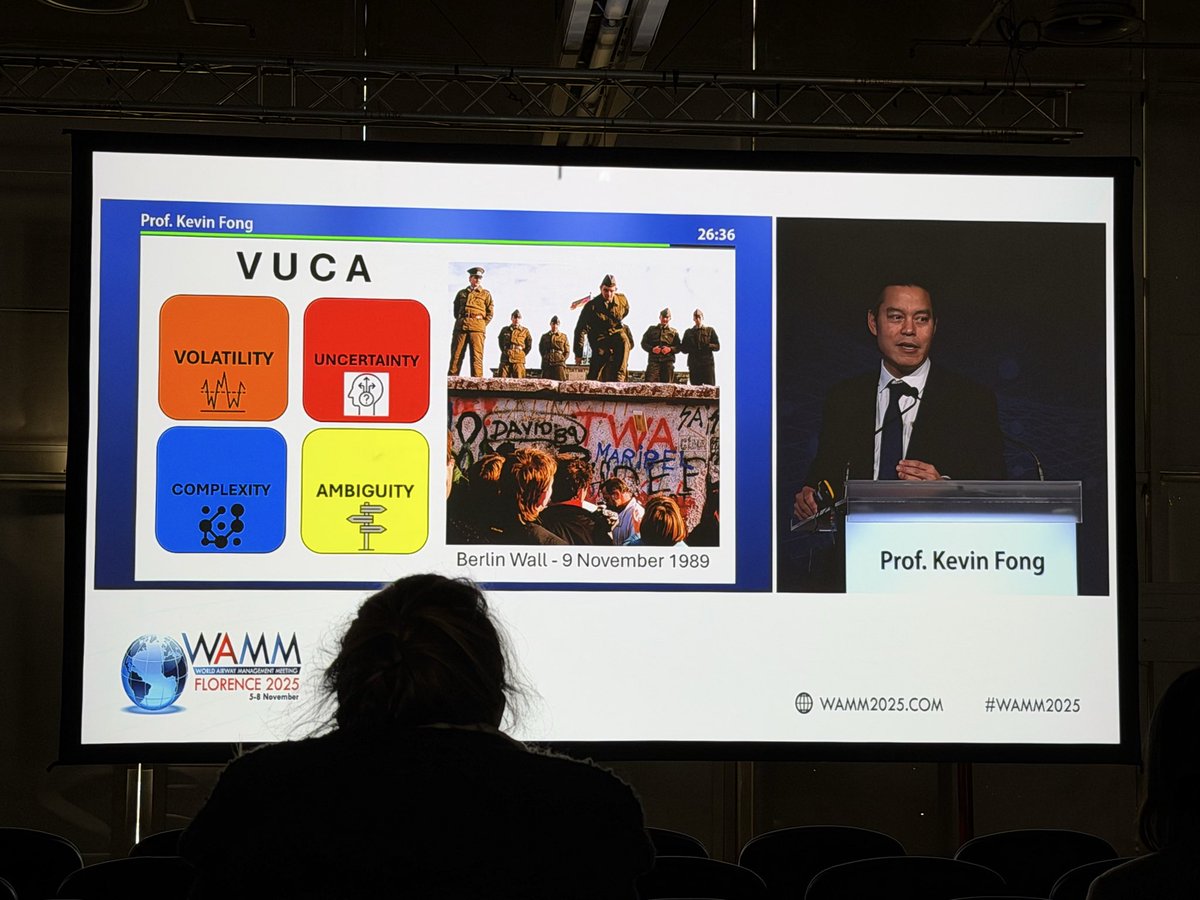
Kevin Fong as always, delivered a wonderful talk on AI.
It always fascinates me the huge carbon footprint of a medium we just think comes out of our computers.
Complex systems require people focussed solutions.
#WAMM2025



5
2
14
914
Yen Chow retweeted

7 Nov 2025
@Admckdoc discussing the airway management in patients living with obesity: best practice recommendations from the Society for Obesity and Bariatric Anaesthesia
associationofanaesthetists-p…
#WAMM2025

2
5
213
Yen Chow retweeted
7 Nov 2025
7 key recommendations from SOBA
- detailed airway Mx
- preO2 in ramped, >30 degrees head up position (pref in theatre)
- consider HFNO
- Intubation in theatre on table
- VL 1st line
- prior to extubation, preoxygenation & adequate reversal of NMB
- suitable equipment
#WAMM2025
11
12
927