
The website Team-ACL.com helps connecting ACL patients and ACL professionals 🔎 Find your team 📝 Join TeamACL #️⃣ @teamacl_ | #TeamACL 🌐Worldwide
Joined June 2020
- Tweets 672
- Following 458
- Followers 696
- Likes 892
29 Photos and videos








Did you rupture your ACL?
🔎 Find your ACL Team
🦵Create your own ACL treatment team to ensure optimal recovery
🤝 One of the biggest steps in your ACL rehabilitation is gathering the best team around you
📈 Compare your options on team-acl.com.


4
7
Team ACL retweeted

22 Oct 2024
Dolphins WR Braxton Berrios tore his ACL against the Colts.
NFL ACL count = 19

3
30
11,999
Team ACL retweeted

3 Jul 2024
🚨 New Paper🚨
👀 Check out our latest article on PNM for managing AMI after ACLR.
🚀 PNM shows promising results in enhancing quadriceps strength and accelerating recovery! 💪🦵
📚Read more: sportperfsci.com/percutaneou…
1
16
70
8,756
Team ACL retweeted

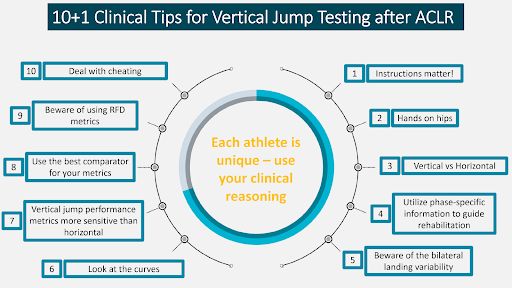
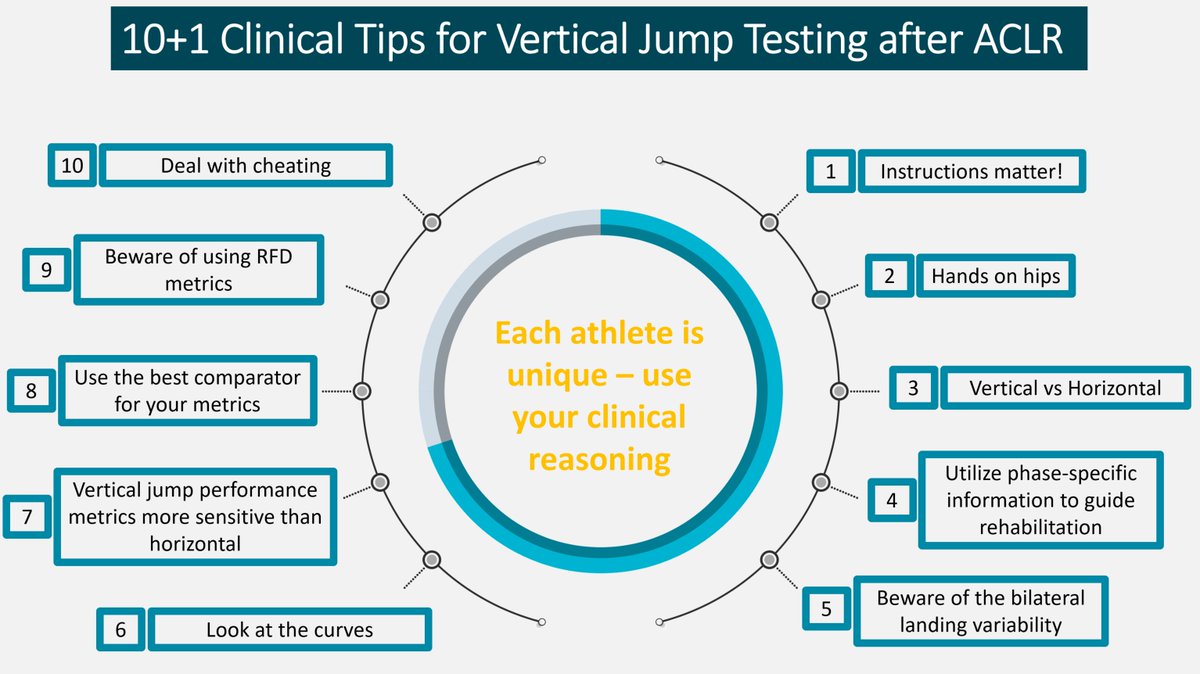
🚨 10 1 #ClinicalTips for vertical jump testing after ACLR
It's about more than just conducting the test:
✅ Selecting the right tests
✅ Adhering to relevant metrics
✅ Understanding the purpose behind the testing
#BJSMBlog ➡️ bit.ly/3TNvLgD
23
76
14,708
Team ACL retweeted

28 Apr 2024
Can an ACL heal without surgery?
I discuss this and findings from our @BJSM_BMJ study with the ABC
abc.net.au/news/2024-04-28/s…
Full paper: bjsm.bmj.com/content/57/2/91
@dr_englund @ewa_roos @FrankRoemer1 @LohmanderStefan
35
105
26,719

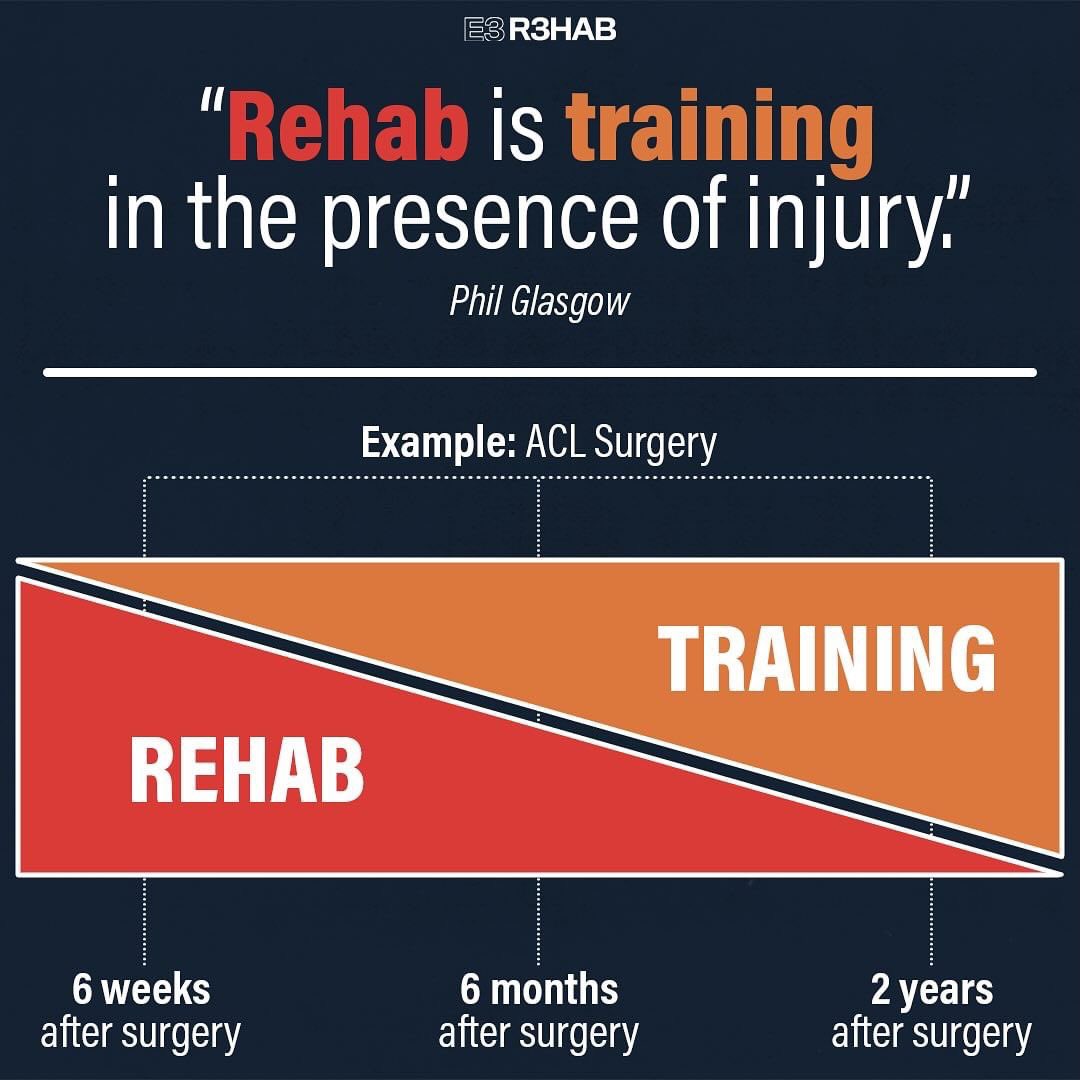
Rehab is often thought of as someone doing something to you – massage, cupping, needling, etc. While you might consider these helpful adjuncts, the foundation for successful rehab is actually built upon learning what you can do for yourself (oftentimes with the guidance of a clinician or coach).
Rehab and training should be represented along the same continuum. If your training looks significantly different from your rehab or your rehab looks significantly different from your training, you may want to re-evaluate your approach to one or both.
This is where exercise modifications can help. These are not to provide cheap gimmicks, quick fixes, or “corrective” exercises. Instead, they are intended to help you find an appropriate entry point to training, while reducing the risk of pain progressing into something more debilitating or long-lasting.
Learn more: youtu.be/fF_wN3nF8Zc
2
27
98
7,163
Team ACL retweeted
🚨 NEW Original Research:
TENDINopathy Severity assessment–Achilles (TENDINS-A) 🦵⚡️
➡️ Evaluation of reliability and validity in accordance with COSMIN
READ HERE ➡️ bit.ly/3PLqncz
34
72
8,043
Team ACL retweeted

5 Apr 2024
10 1 Clinical Tips for Vertical Jump Testing after ACLR
▶️ Tip #1: Instructions matter!
▶️Tip #2: Hands on hips
▶️ Tip #3: Vertical vs Horizontal
▶️ Tip #4: Use bilateral vertical jumps to check for compensatory strategies
▶️ Tip #5: Landing of vertical jumps
▶️ Tip #6: Look at the curves
▶️ Tip #7: Performance metrics
▶️Tip #8: Choose your comparator
▶️Tip #9: Rate of Force Development (RFD)
▶️ Tip #10: Dealing with cheating
▶️ Tip #11: Every athlete is unique
👉👉More ➡️ bit.ly/3xw9M6k
👉 👉 Paper ➡️ bjsm.bmj.com/content/57/20/1…
✍️ : @RoaldBahr @enda_king @RoulaKotsifaki
@vas_sideris @RodWhiteley

26
70
7,439
Team ACL retweeted
4 Apr 2024
The Use Of Blood Flow Restriction In Early Stage Rehabilitation Following ACL Injury.
Using BFR training during rehabilitation post ACLR appears to be safe and practically feasible. No adverse effects on knee laxity have been found with BFR training compared to heavy load training.
It has also been shown both acutely and chronically that patients experience less knee pain during and for up to 24 hours post-exercise with BFR training, with a greater overall reduction in pain following 8 weeks of training.
Moreover, the perceived exertion and muscle pain responses to BFR training appears not to limit application or adherence to training.
How To Implement BFR Training
So how do we go about using BFR in a practical setting? Recent research supports individualisation of BFR application, where BFR is prescribed as a percentage of ‘arterial limb occlusion pressure’ (LOP), which represents the minimum pressure required for total arterial occlusion. Manipulation of BFR protocols has been shown to influence the perceptual, hemodynamic, and neuromuscular responses to BFR exercise.
How BFR Can Enhance The Return To Sport Process
When to return to sport following ACLR is a controversial issue. It is common for patients to be at a higher risk of re-injury compared to healthy controls.
Strength and conditioning coaches, rehabilitation specialists and surgeons utilize a range of assessments to determine an athlete’s readiness to return to sport, including:subjective rating scales, knee laxity testing, isokinetic testing, functional hop testing, balance testing, and movement assessment. Whilst this has improved over recent years, several studies have demonstrated deficits in muscular strength, kinaestheticsense, balance, and force attenuation 6 months to 2 years following reconstruction.
With this in mind, the return to sport following ACLR should not be rushed. Furthermore, we suggest BFR be used to mitigate some of these residual deficits that athletes experience.
By using BFR earlier in the rehabilitation to offset atrophy and strength loss (phase 1) and improve strength and hypertrophy (phase 2), practitioners can spend more time focussing on neuromuscular control, functional strength, rate of force development, and psychological readiness which are necessary for a successful return to competition and reducing the risk of re-injury
BFR provides a low-load safe and efficacious treatment modality for athletes following ACLR.
As it gains more acceptance in clinical settings and more robust clinical trials are published, there has been a shift in the acuity of its usage and adoption across clinical conditions.
Clinical trials have advanced to not just explore the ability of BFR to preserve and restore lost muscle mass and strength, data are now available which report its ability to preserve bone loss after ACLR, provide a reduction in pain, swelling and function.
More recent advancements have also advocated its use in prehabilitation prior to ACLR where a reduction of muscle fibrosis and upregulation of satellite cells have been shown along with accelerated return to play.
Thus, we propose that these findings provide an important message for clinicians and athletes alike - train hard, train smart and start early!
🔗 Read More 👉 journal.aspetar.com/en/journ…
✍️ Written by Stephen D Patterson, Johnny Owens and Luke Hughes.

49
130
11,182
Team ACL retweeted

5 Apr 2024
🆕@BJSM_BMJ Blog
Vertical Jump Testing after #ACLR - 11 Clinical Tips!
Blog ➡️ bit.ly/3xw9M6k
Paper ➡️ bit.ly/3WHWlch
3
36
115
10,175
Team ACL retweeted

3 Mar 2024
AMAZING TEAM EFFORT 🤩 🤩 🤩 !!!
3 Mar 2024

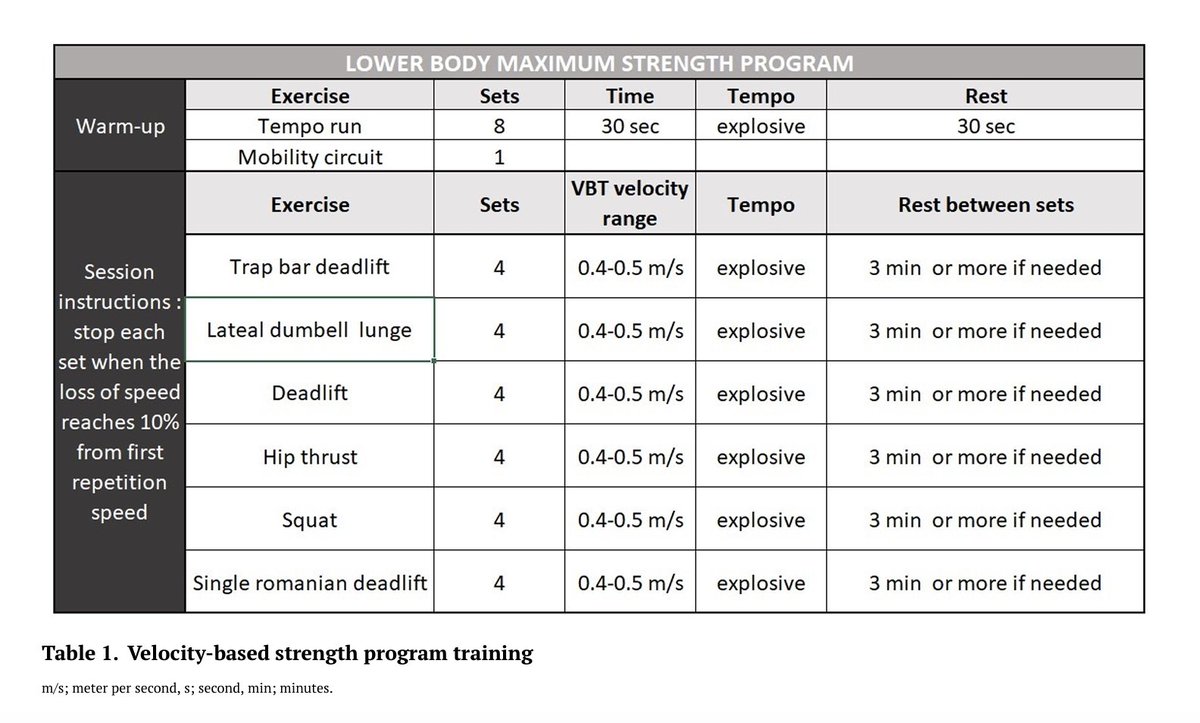
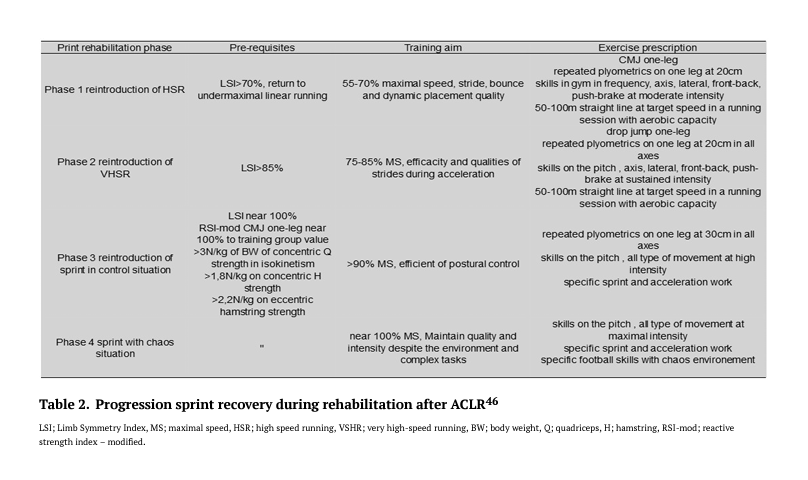
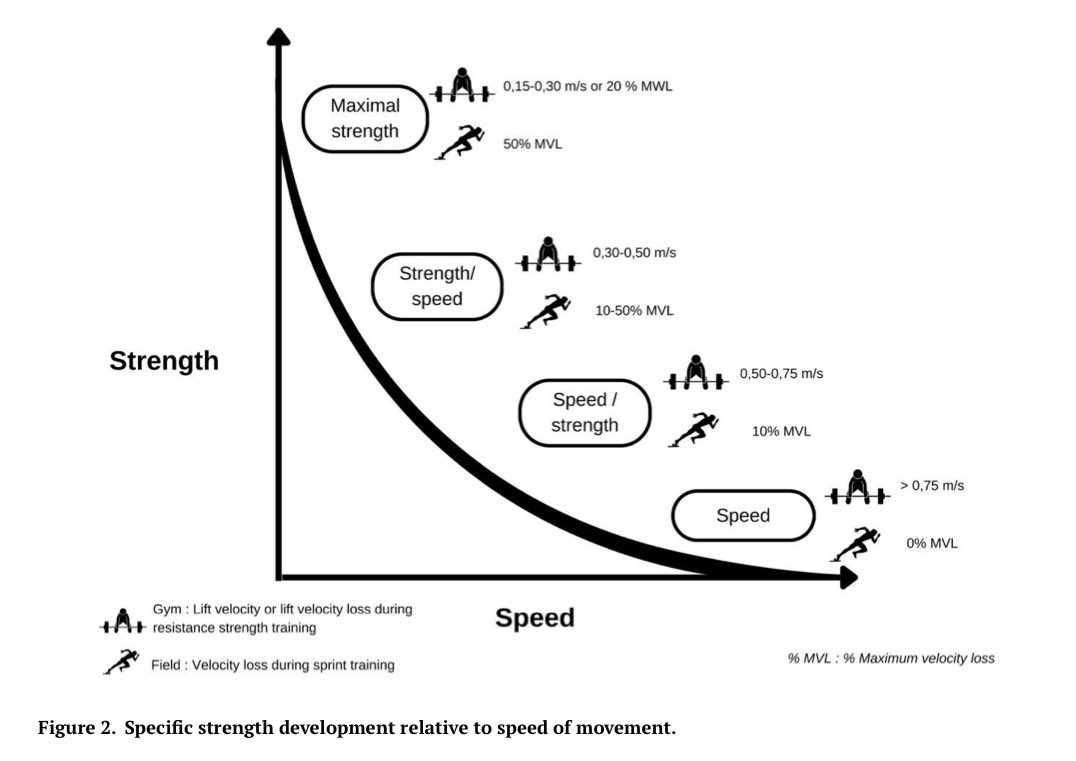
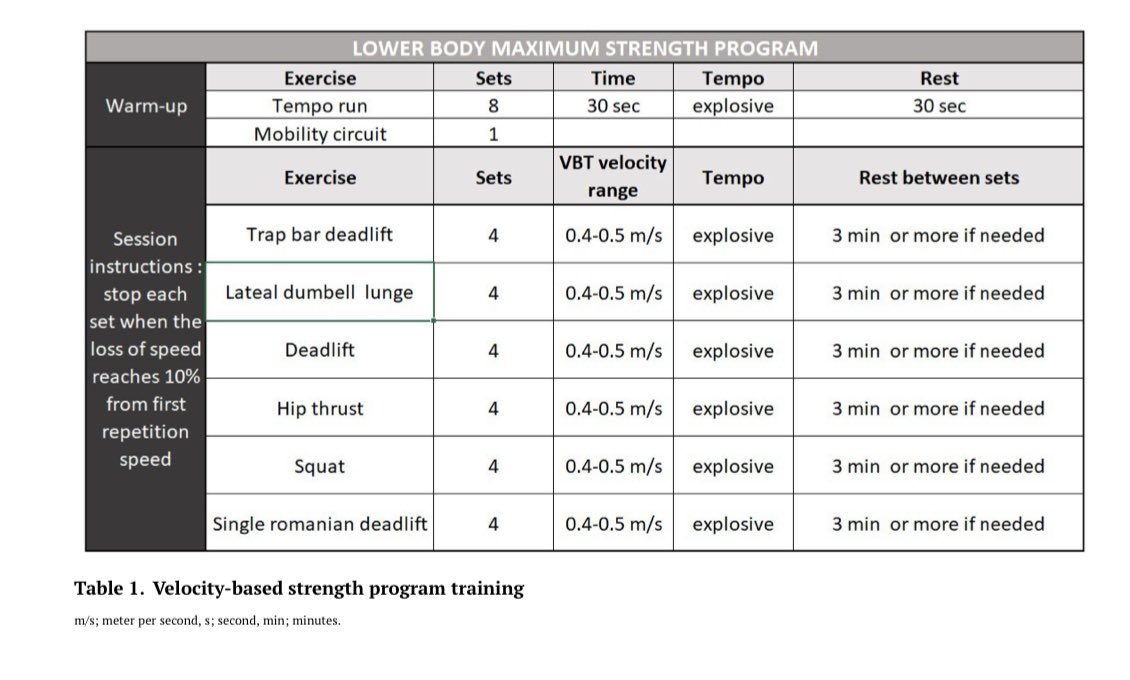
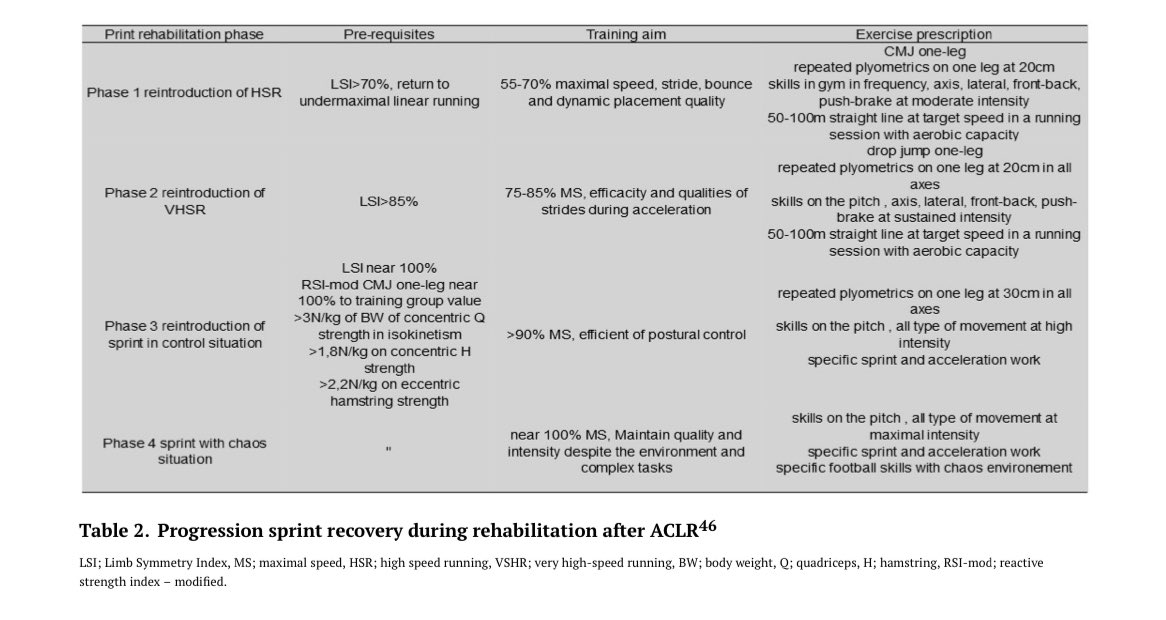
🆕"ACLR & Progression to Sprint Return in Soccer Players"
▶️ Velocity-based return to sprint program which can be used during ACLR rehabilitation ⚽️
👉@ForelliFlorian @Hewett1Tim et al., 2024
📂 Open Access: ijspt.org/implementing-veloc…

2
5
31
3,965
Team ACL retweeted
1 Mar 2024
💥𝗡𝗘𝗪 𝗣𝗔𝗣𝗘𝗥💥
ℹ️ ACLR & Return to Sprint 🏃♂️in @IJSPT 🗞️
☝️Requirements for sprint performance
⚡️Force-Velocity & Acceleration-Speed Profiles
🧨VBT & sprint specific strength
📈Progression sprint recovery during rehab
Free Access 🔓 ijspt.org/implementing-veloc…

1
65
245
22,210
Team ACL retweeted
2 Jan 2024
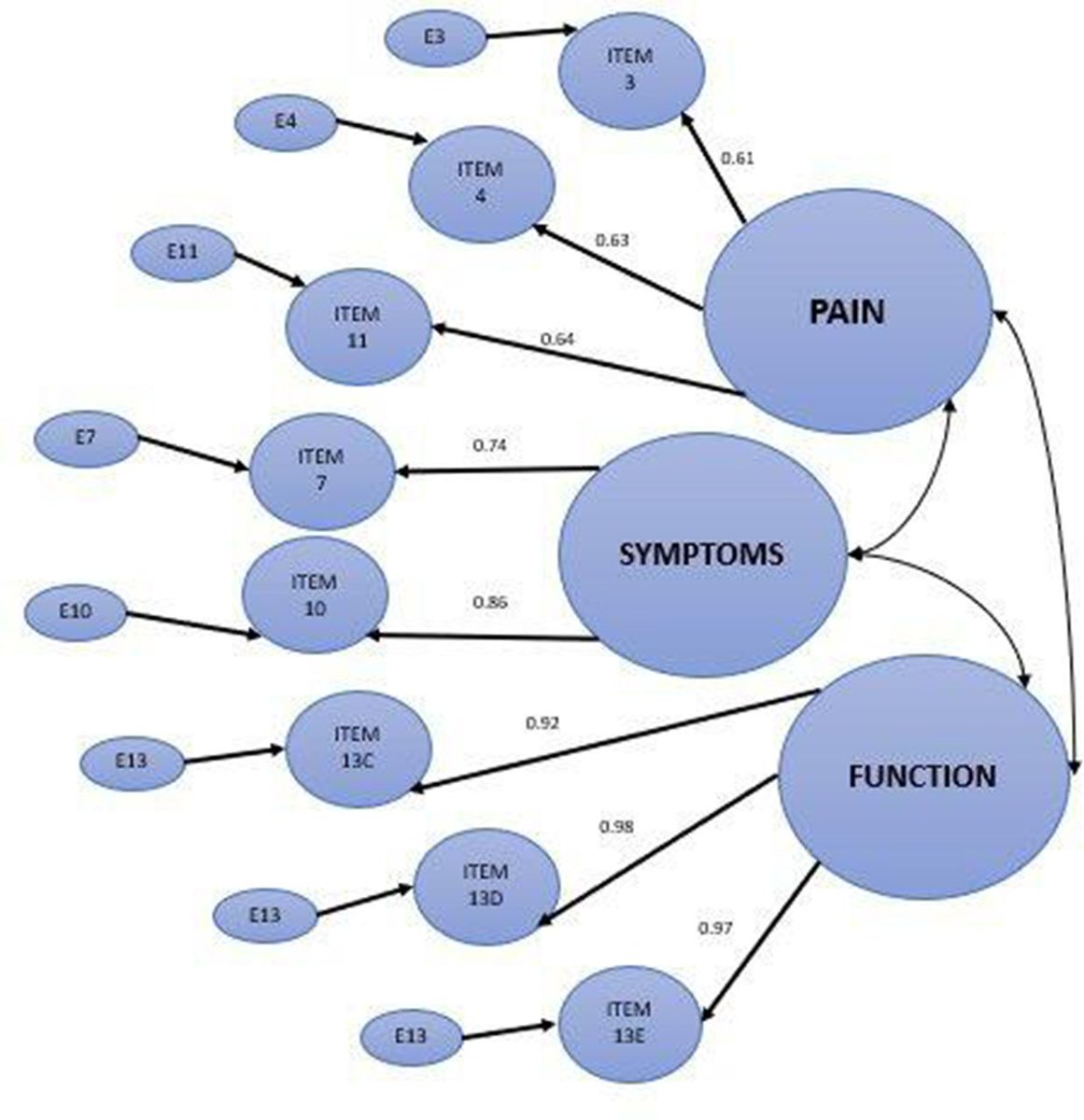
Quadriceps activation ⚡️ after ACL reconstruction or injury💥 🧵: the early bird gets the worm ! 🐤🐛
Congrats @Sonnerycottet & team 🎉
@TeamACL_

5
25
2,308
Team ACL retweeted
2 Jan 2024
Dolphins LB Bradley Chubb did in fact tear his ACL.
NFL ACL count = 35

3
4
40
17,080
Team ACL retweeted
31 Dec 2023
There have been 528 torn ACL’s in the NFL since 2013. We’ve see 33 so far this year. Here’s the totals by season:
2023 - 33 and counting…
2022 - 51
2021 - 56
2020 - 42
2019 - 34
2018 - 53
2017 - 52
2016 - 49
2015 - 50
2014 - 45
2013 - 63
9
15
116
31,848
Team ACL retweeted

24 Dec 2023
x.com/thefarazzl18622/status…
The 3 commonly used clinical tests for an ACL deficient knee demonstration beautifully here during examination under anaesthesia:
1. The Pivot Shift Test
2. The Lachmans Test
3. The Anterior Drawer Test
@Hewett1Tim @TimHewett5
7
102
390
39,824
Team ACL retweeted
23 Dec 2023
BUILDING BETTER BRAKES… @TimothyHewett1 @TimHewett5 @PoweredByTRAZER @ChadLavenderMD @MUHealthOrtho @Herd_SportsMed @MUSOMWV @HerdZone @MJofMWV @marshallu
23 Dec 2023

8
26
7,967
Team ACL retweeted

24 Dec 2023
Quad strength assessment - no excuses anymore!! 💪
23 Dec 2023

Open access 🔑
authors.elsevier.com/sd/arti…
practical means of testing quads strength after ACL reconstruction with
⬆️ reliability
⬆️ concurrent validity
❌ fixed or proportional bias
✅ safe
✅ time efficient
✅ affordable
✅ normative values

6
26
3,865
Team ACL retweeted

18 Dec 2023
Step by Step | Episode one 🎬
Follow @bmeado9 and @viviannemiedema as they recover from ACL injuries and explore why this issue remains so prevalent in the women’s game.
Now live on Arsenal.com for free 👇
50
325
3,172
290,747

Team ACL retweeted
18 Dec 2023
Checkmate my friend ⚡️🦵🏻
📚 pubmed.ncbi.nlm.nih.gov/3256…
17 Dec 2023


4
18
3,242