Gastroenterologist. Shining a light on bowel cancer. Inspector of endoscopy units, stomachs & bile ducts too. Some tweets my own.
Joined December 2014
- Tweets 2,700
- Following 1,191
- Followers 1,637
- Likes 2,654
520 Photos and videos


Dr John O'Donohue retweeted

14 Apr 2025
🧵1/6
🚨 New from the British Society of Gastroenterology:
We analysed all UK colonoscopies from the National Endoscopy Database (2019–2020). That’s over 592,000 procedures. Findings below 👇
(📄 Free article link (limited time): authors.elsevier.com/c/1ktHw…)
1
15
29
5,817

13 Aug 2024
Well, what sort of farewell cake did you expect at an upper GI surgeon’s retirement party? @LG_NHS
Saying happy retirement to Mr Alek Uzkalnis!
4
10
677
20 May 2024
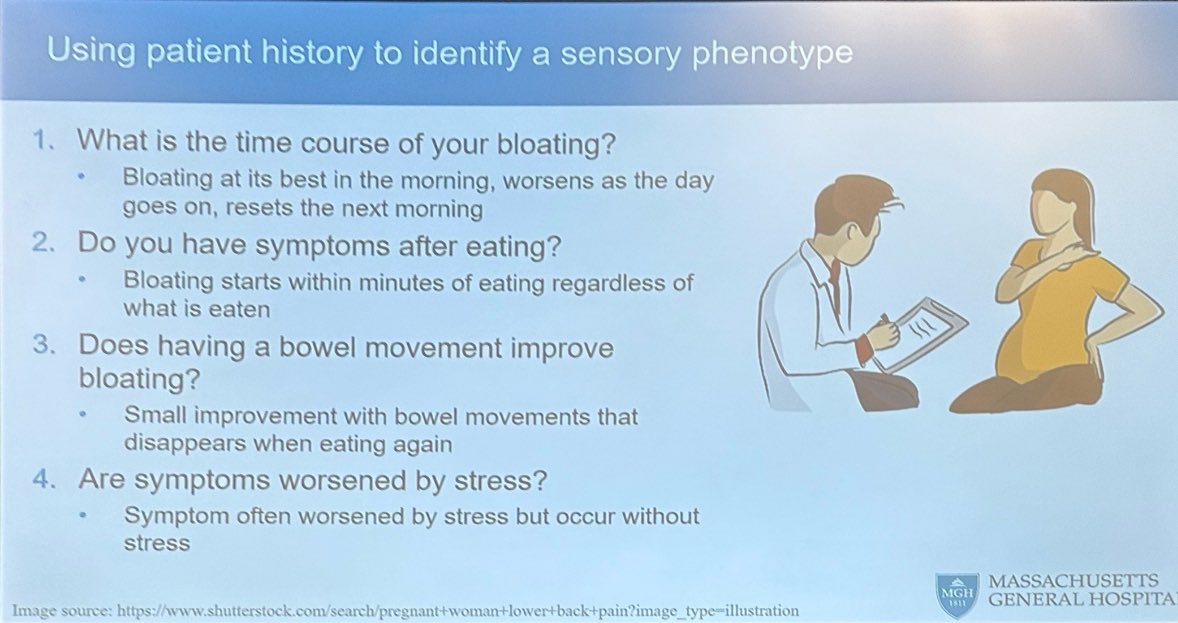
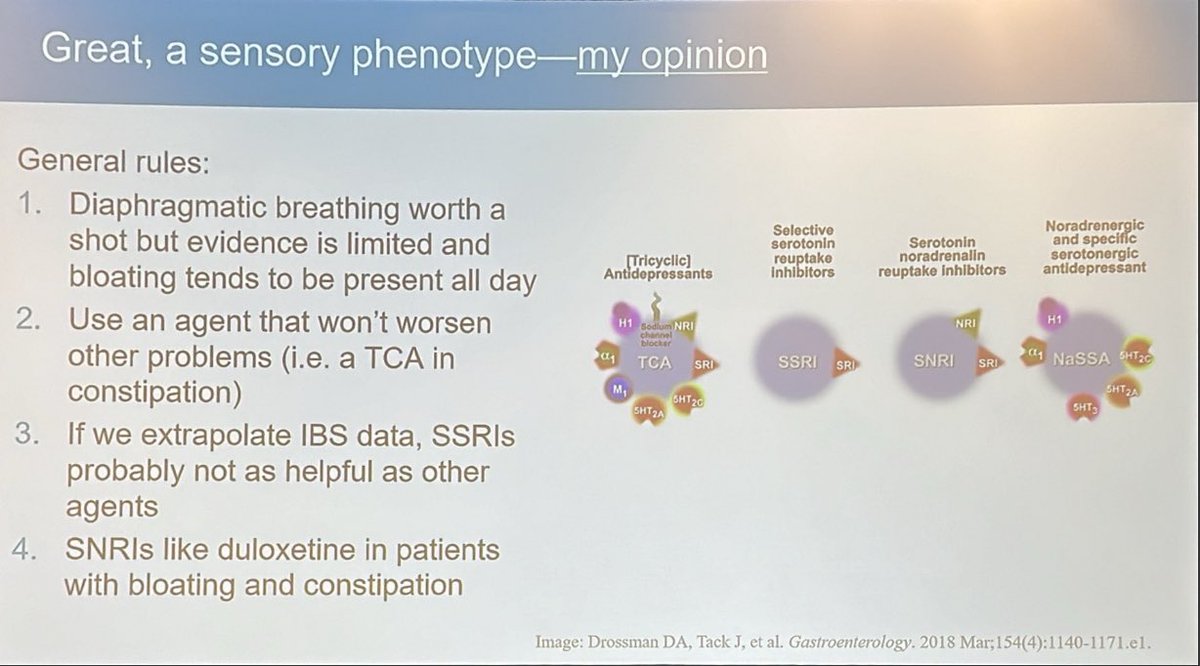
How to identify the ‘sensory phenotype’ in bloating, and how to treat it:
Duloxetine, not SSRI, is best if diet and diaphragmatic breathing isn’t enough and pharmaceutical treatment needed
Kyle Staller, Mass General @DDWMeeting
2
452
20 May 2024
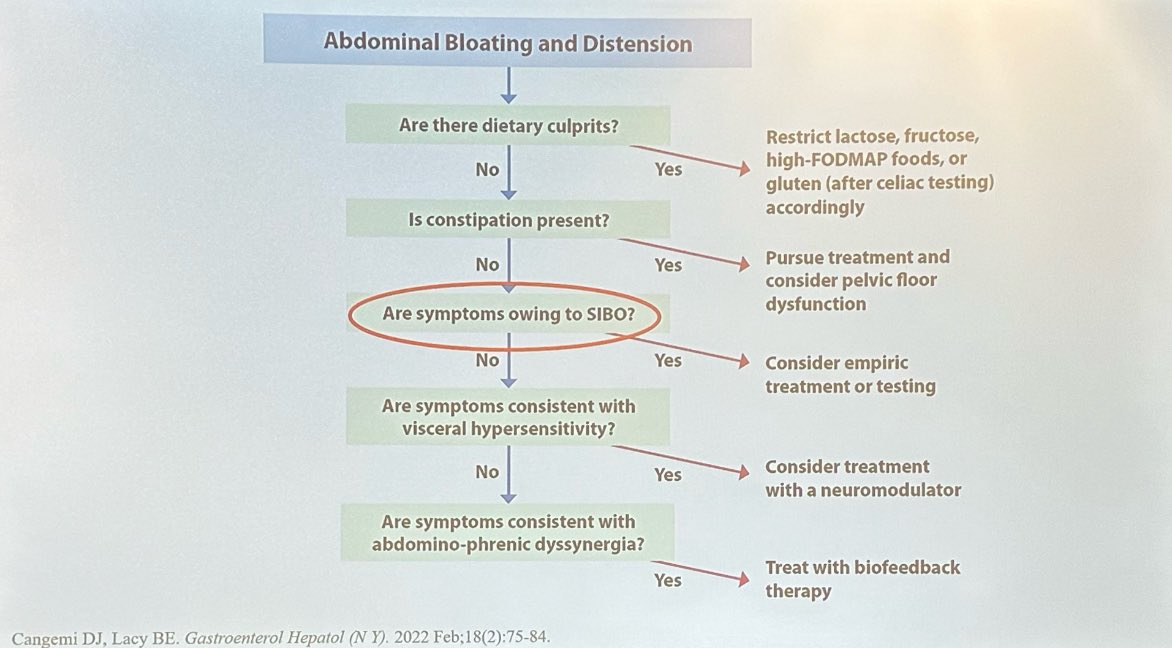
Practical guide to management of bloating - all in one slide
- Kyle Staller, Mass General Hosptial @DDWMeeting
1
4
457
20 May 2024
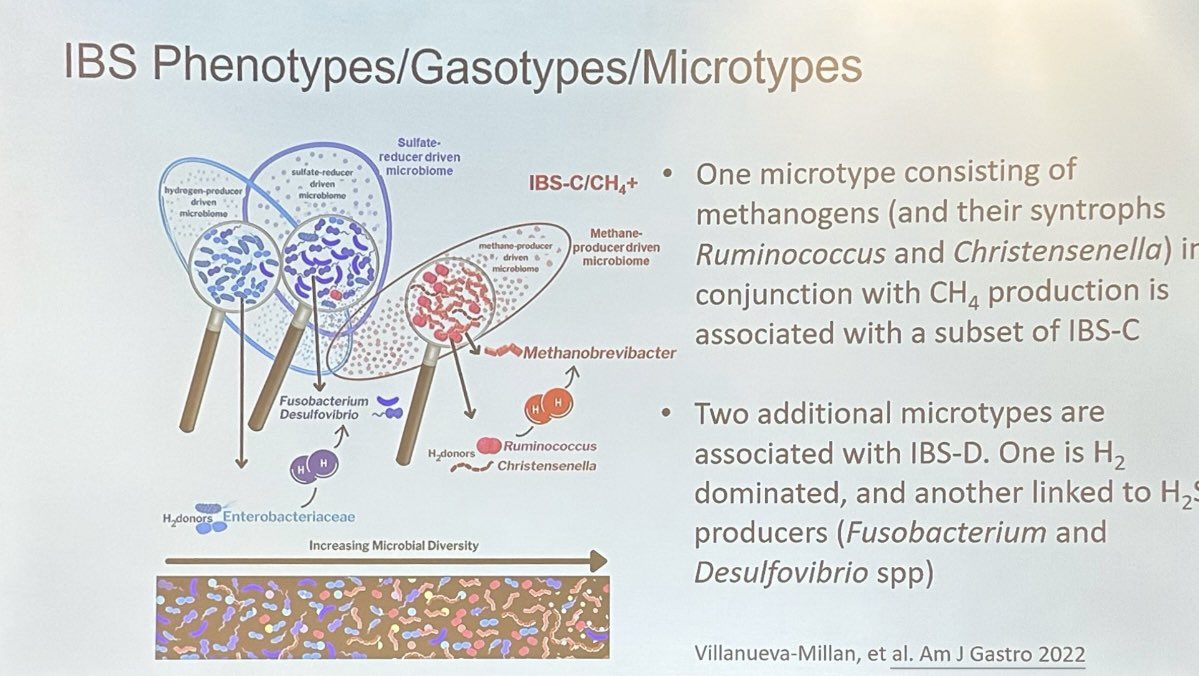
IBS microbiome subtypes in types of IBS:
Mike Pimentel, Cedars-Sina @DDWMeeting
IBS-C: methanogens
IBS-D: hydrogen sulfide
1
1
195
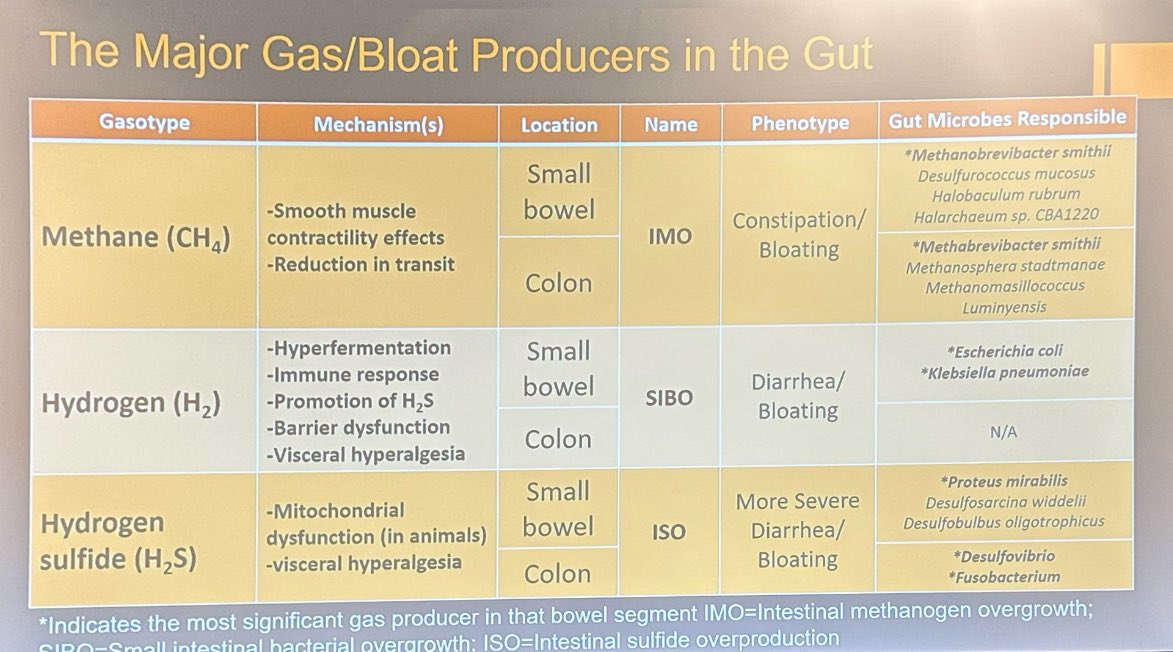
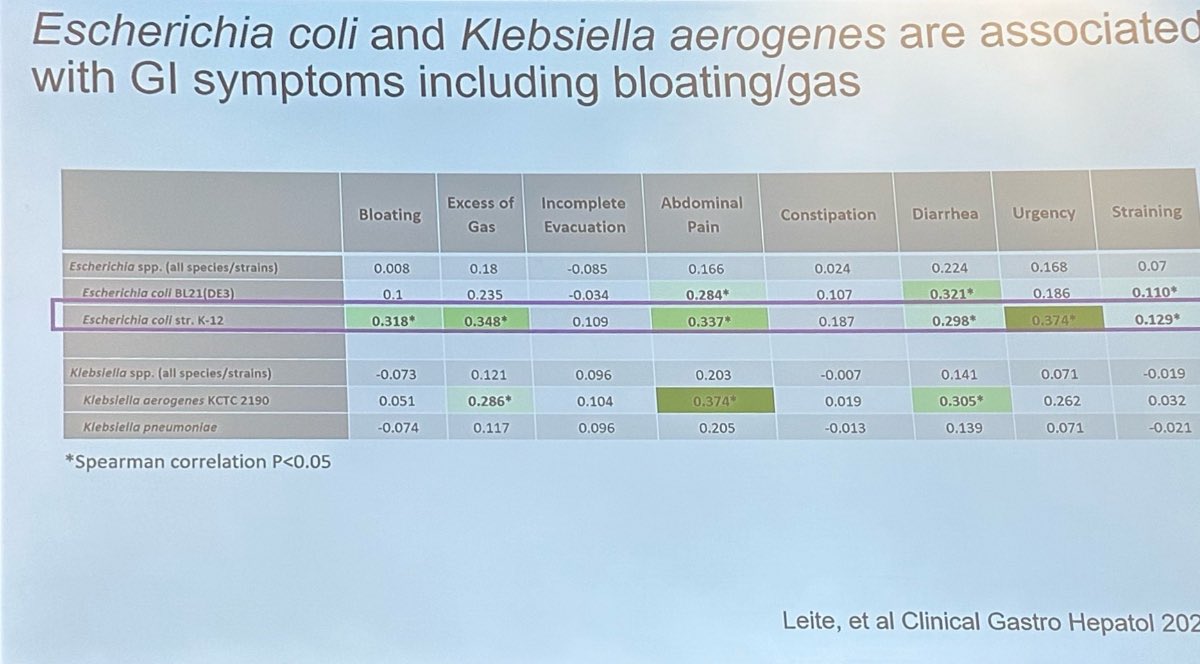
20 May 2024
SIBO due to just two bacteria: E. coli and klebsiella
1
1
163
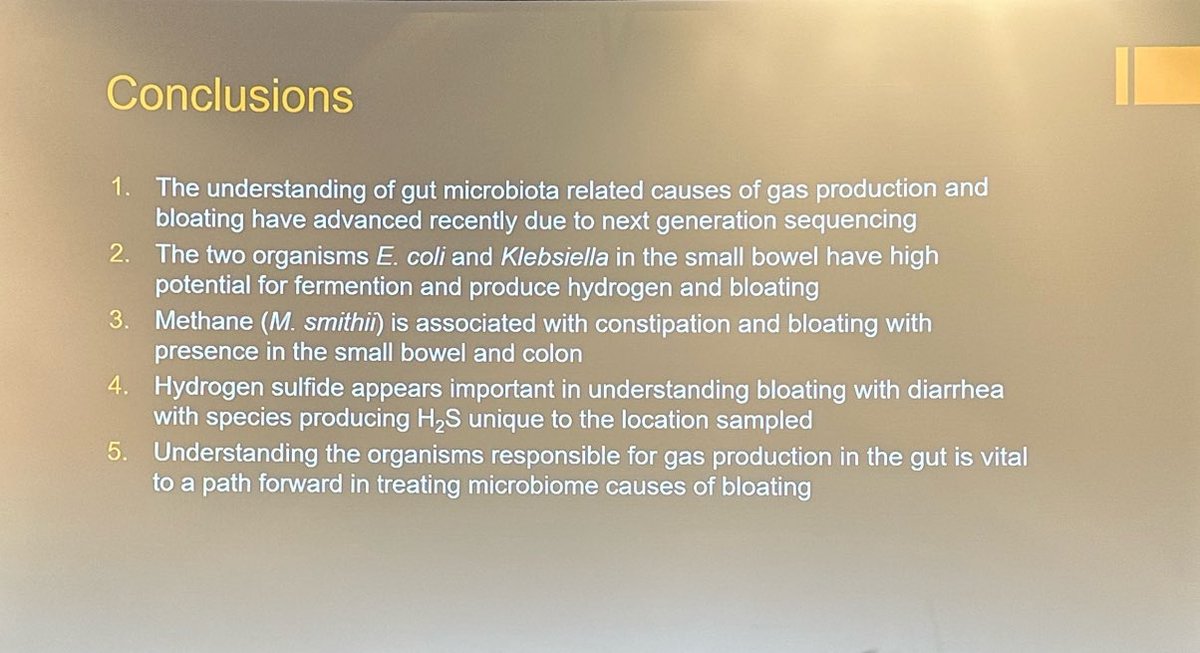
20 May 2024
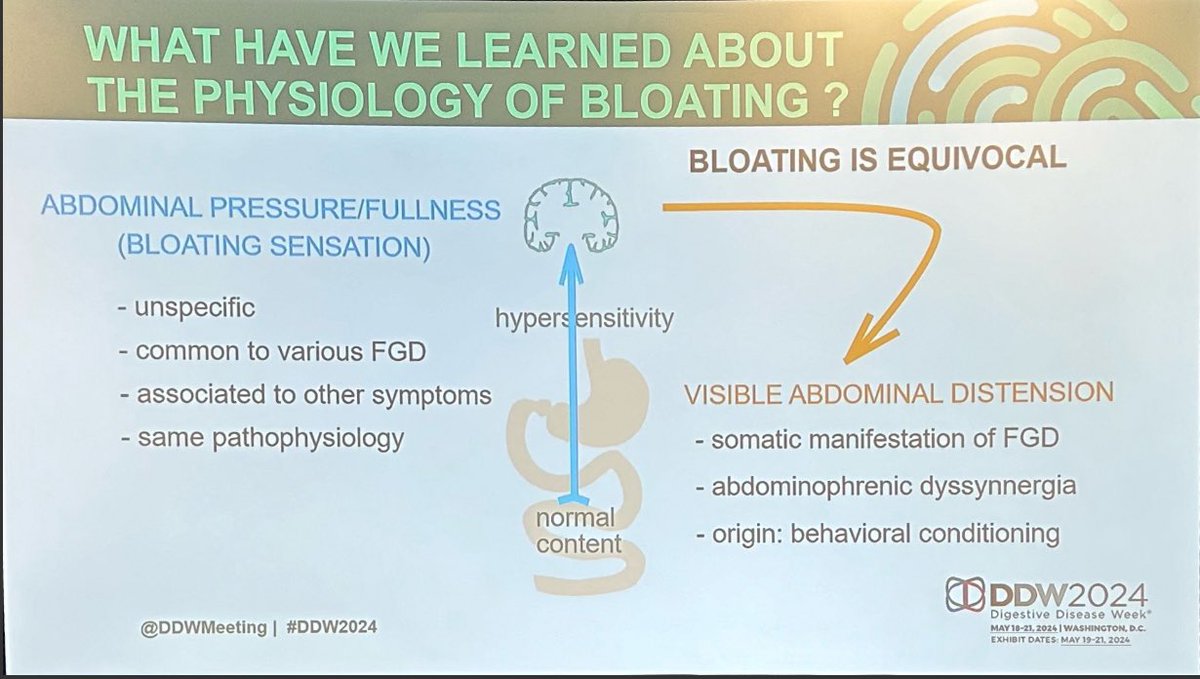
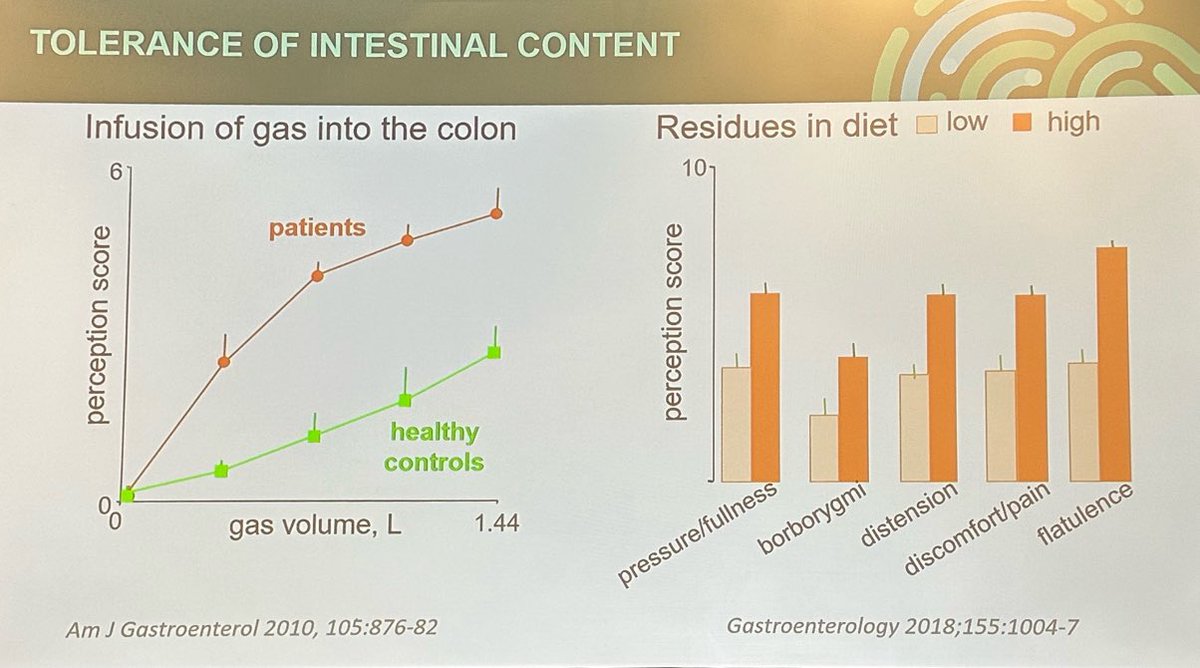
What’s different between patients with bloating & normal controls?
Fernando Azpiroz, Hspital Val d’Hebron @DDWMeeting
Not amount of gas, or biomass.
It’s sensitivity to distension.
Perceived distension can be obesity, or descent of diaphragm (abdominophrenic dyssynergia)
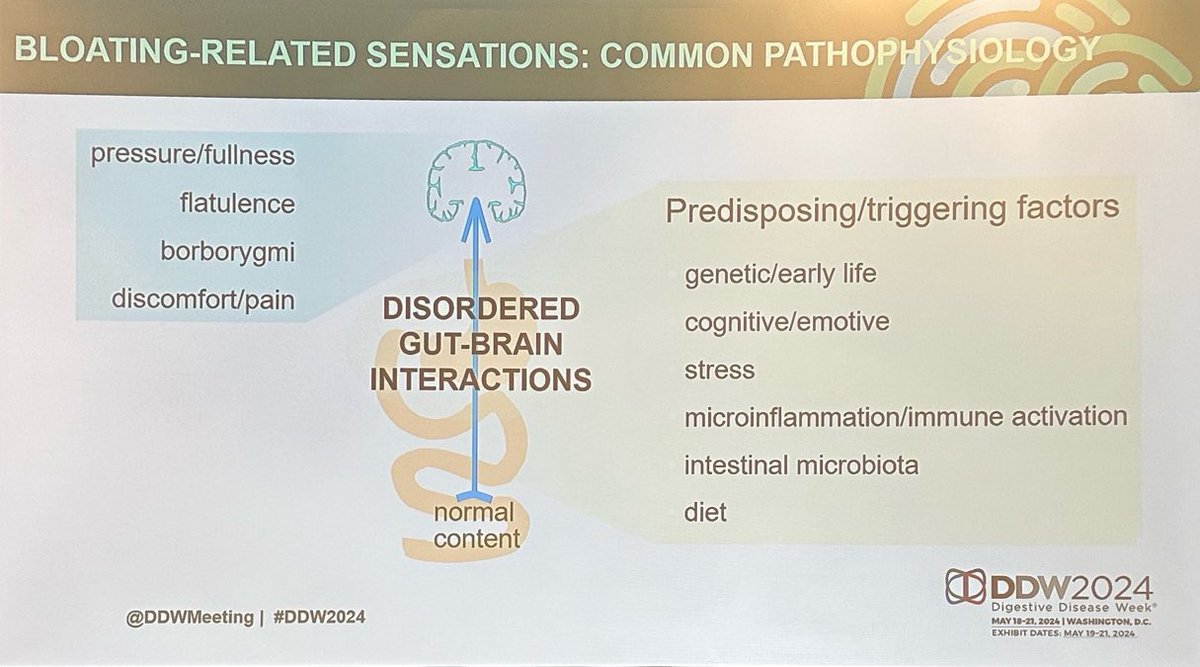
1
209
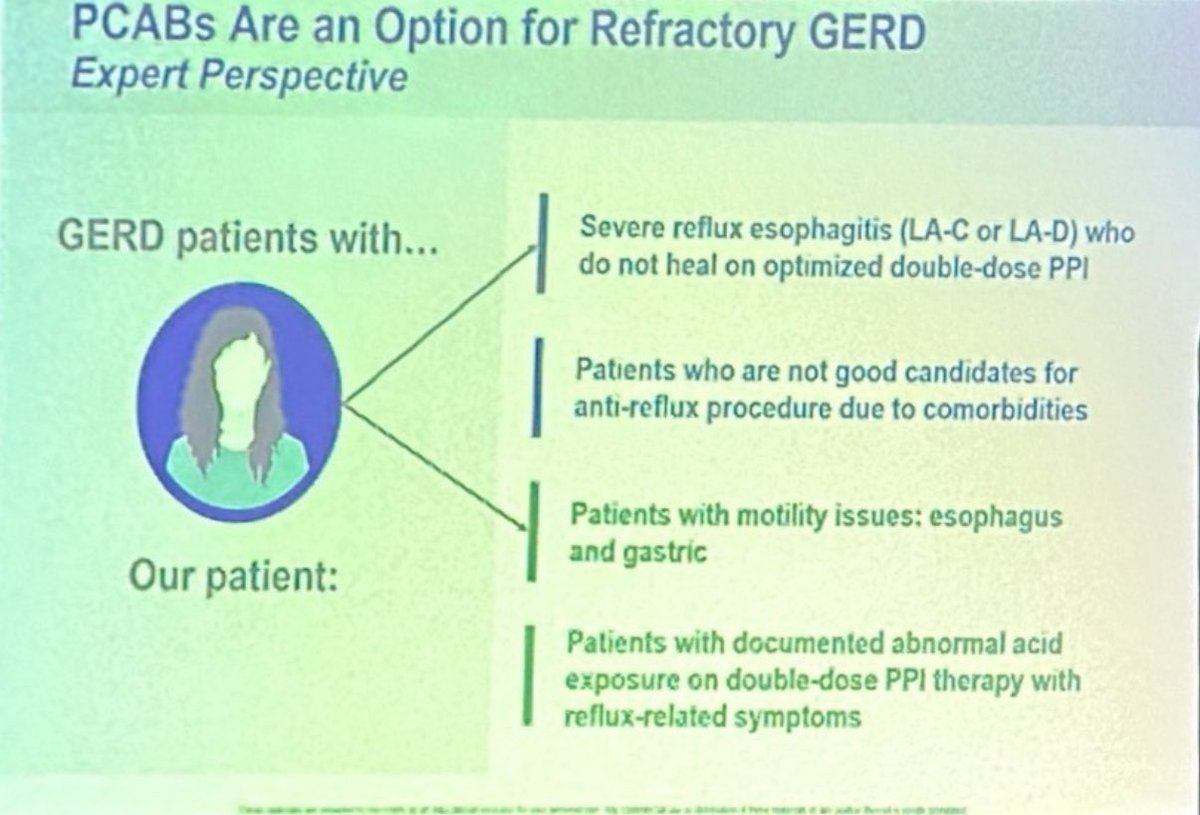
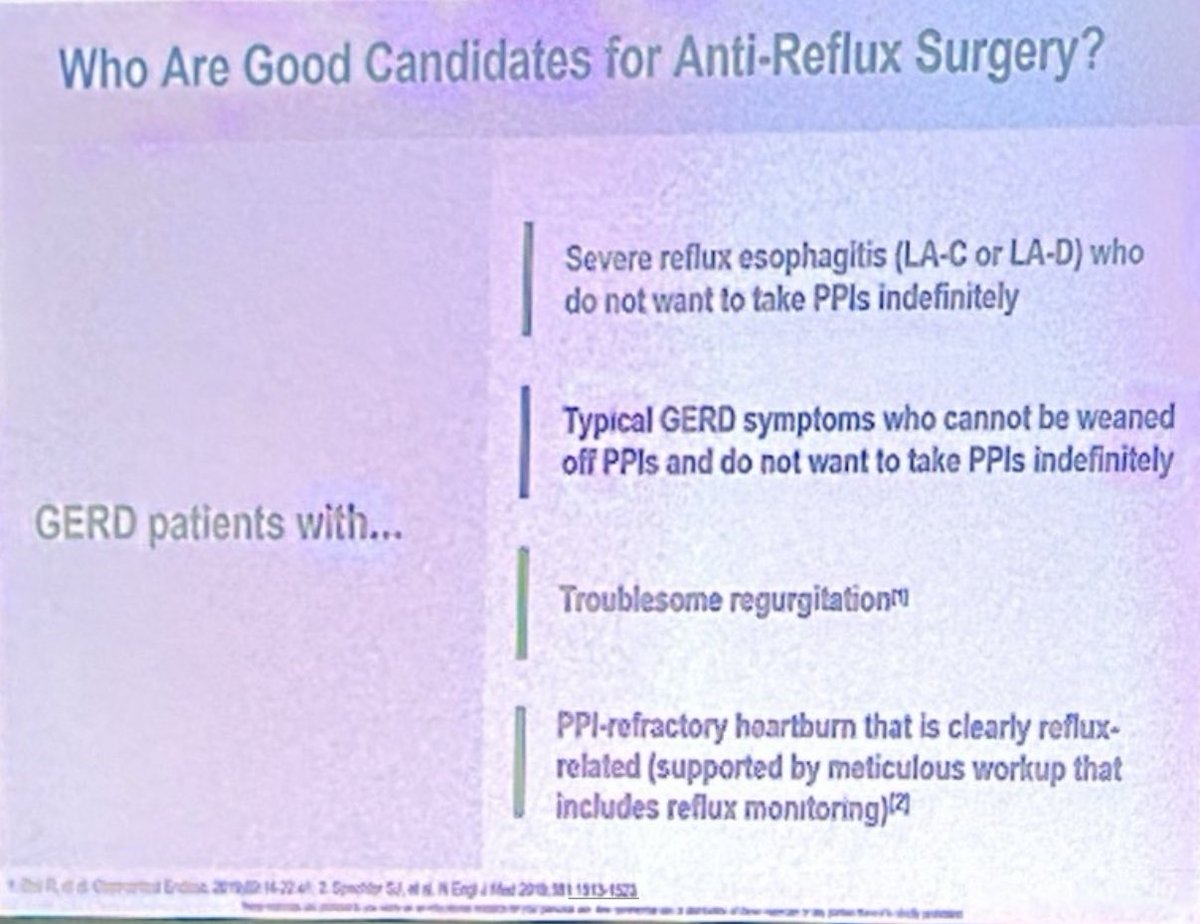
20 May 2024
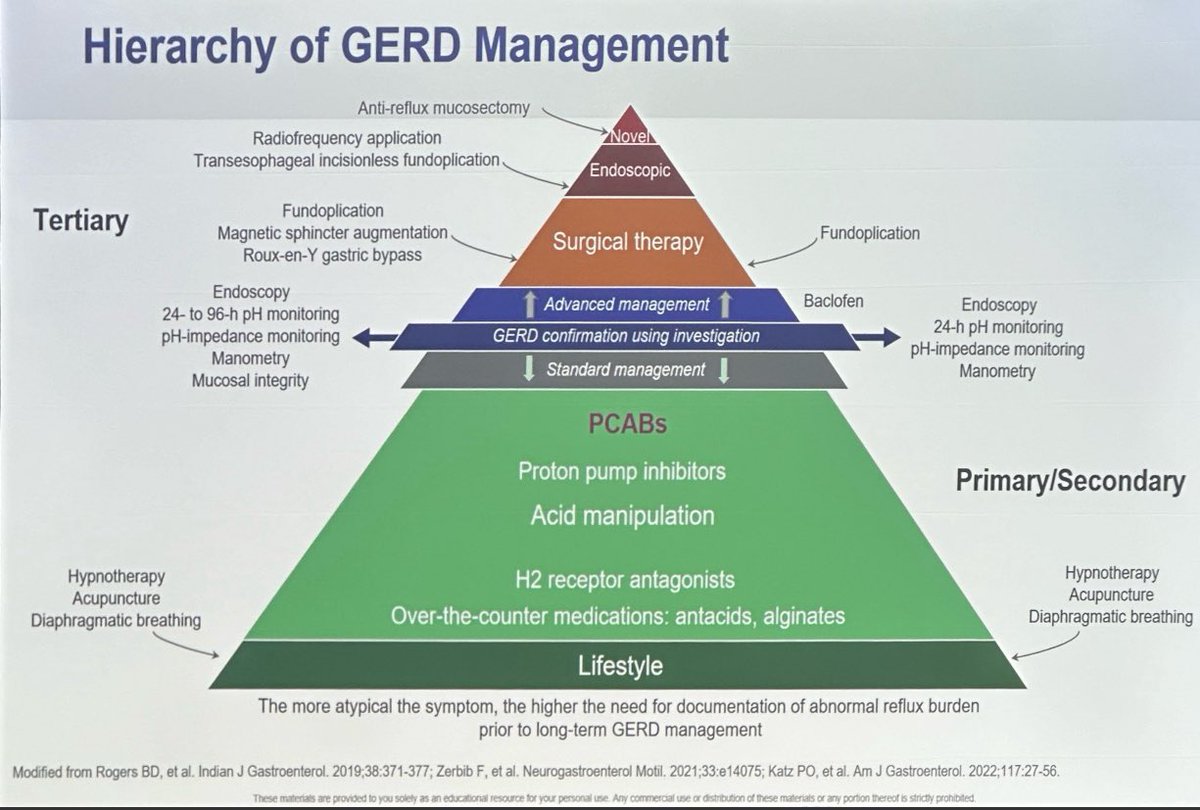
Management of reflux @DDWMeeting
- hierarchy of management
- where to use PCABS for PPI-refractory reflux
-who are good candidates for an anti-reflux procedure
2
2
302
19 May 2024
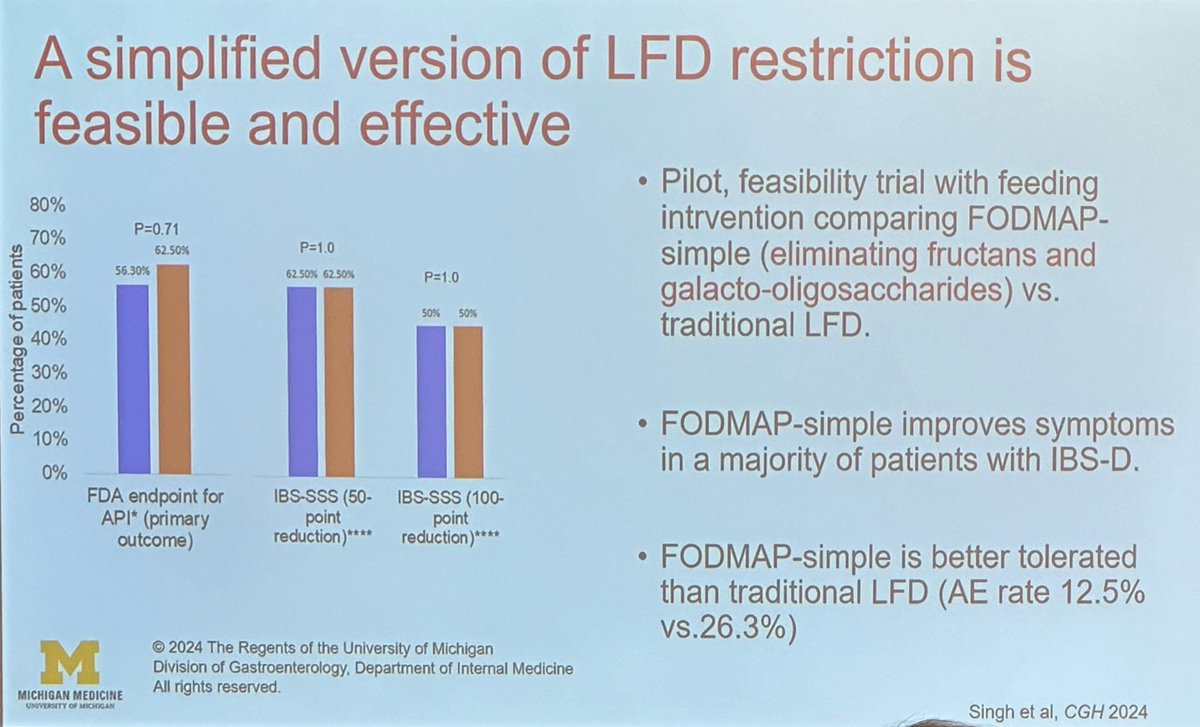
Not all FODMAPs are equal! Can we simplify FODMAP restriction in IBS-D?
Prashant Singh, Un of Michigan @DDWMeeting
FODMAP restriction difficult and can result in micronutrient malnutrition
In reintroduction phase, most symptoms due to fructans & galacto-oligosaccharides
1
1
253
18 May 2024
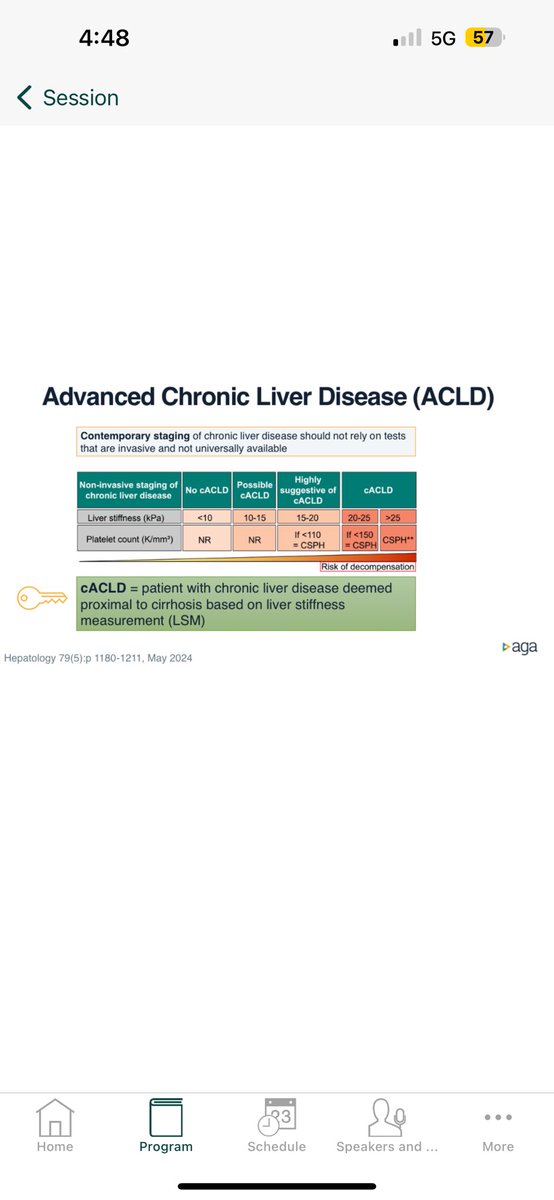
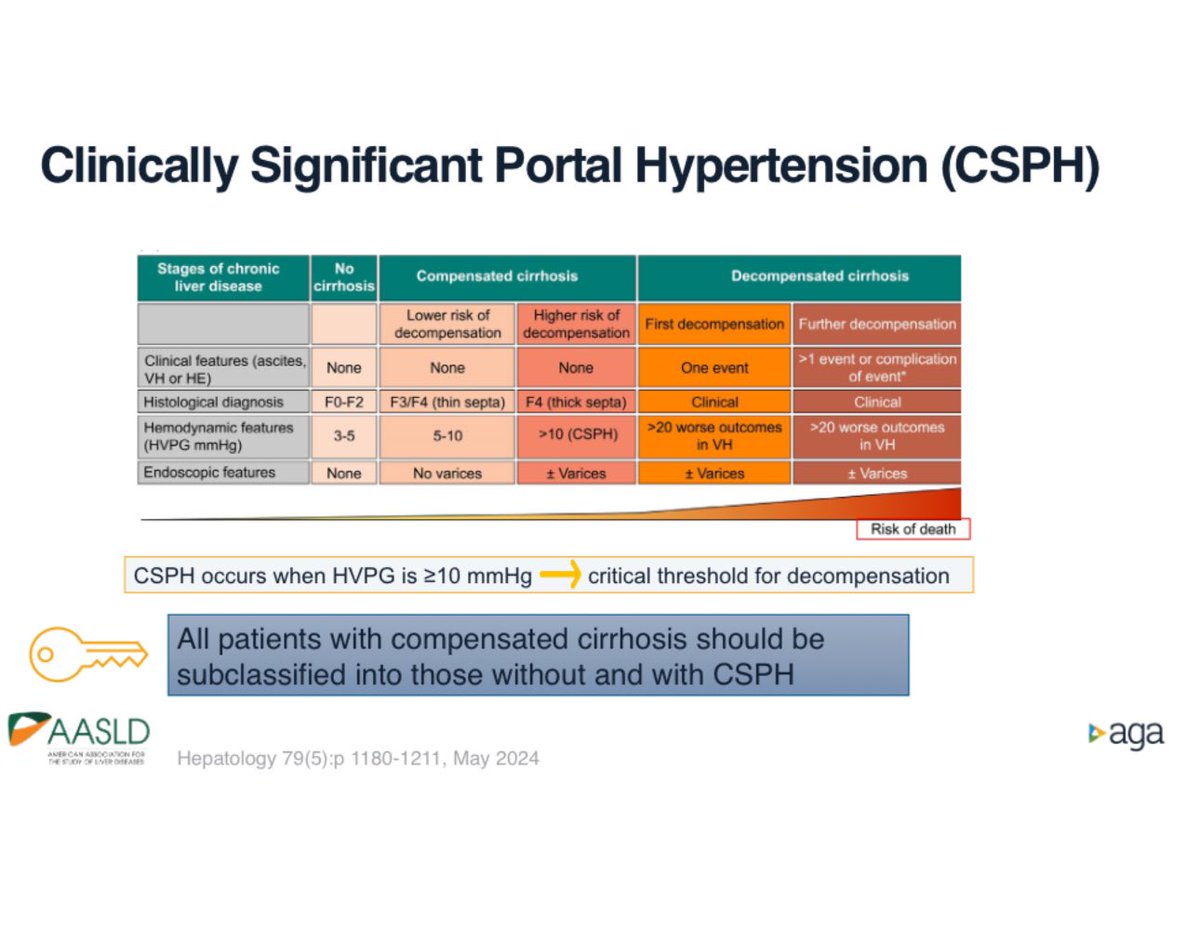
Heather Patton, VA San Diego, CA @DDWMeeting
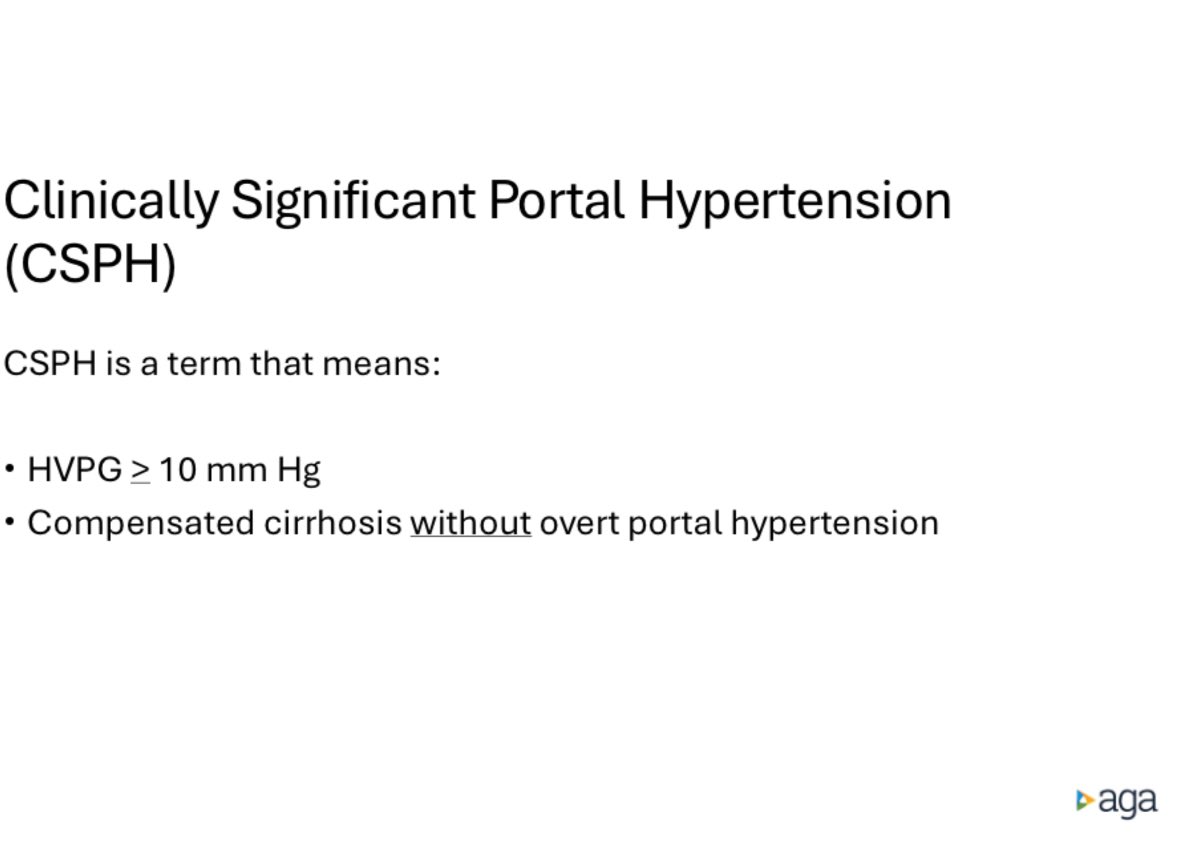
All patients with compensated cirrhosis should be subclassified as with or without Clinically Significant Portal Hypertension (CSPH)
- and pharmacotherapy used (eg carvedilol) to lower portal pressure
Note NEW terminology!
1
181
18 May 2024
New treatment paradigm for PBC (Primary Biliary Cholangitis) - Dr Willscott Naugler, Portland, Oregon
1
192
18 May 2024
However, 40% of patients do not respond adequately to UDCA. Pruritus can be exacerbated by Obeticholic Acid - which can’t be used with decompensated cirrhosis. Elafibrinor, a PPAR agonist, shows promise and improves pruritus.
96
18 May 2024
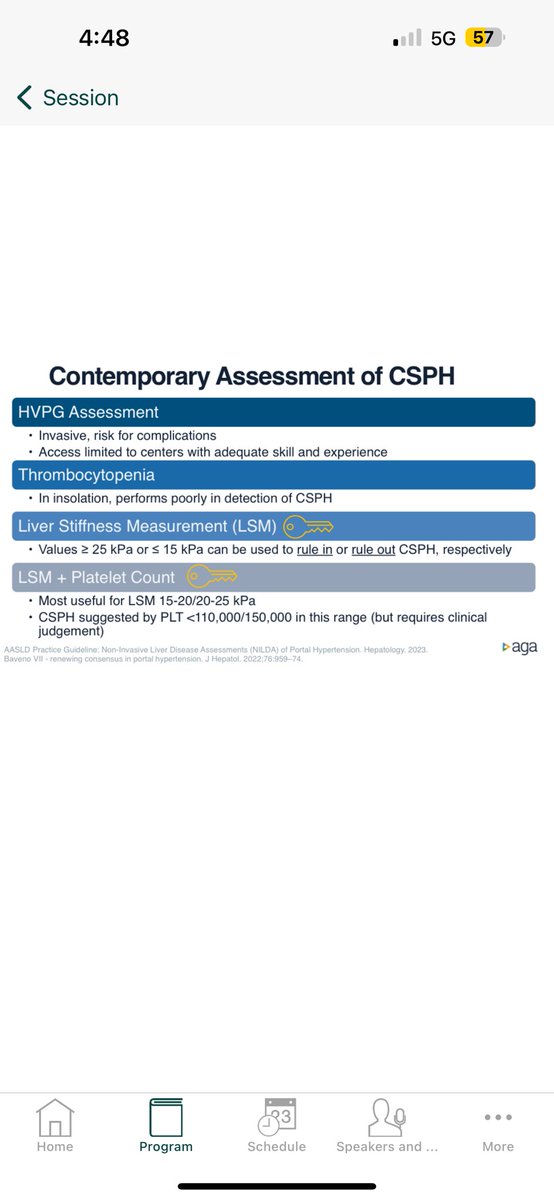
Don’t need endoscopy to screen for varices in patients with cirrhosis any more - Dr Willscott Naugler, Portland, ON @DDWMeeting
Concept of ‘Clinically significant Portal Hypertension’ - if > 10 mm Hg elevation is present, start on beta blockers to prevent varices, ascites
1
165
18 May 2024
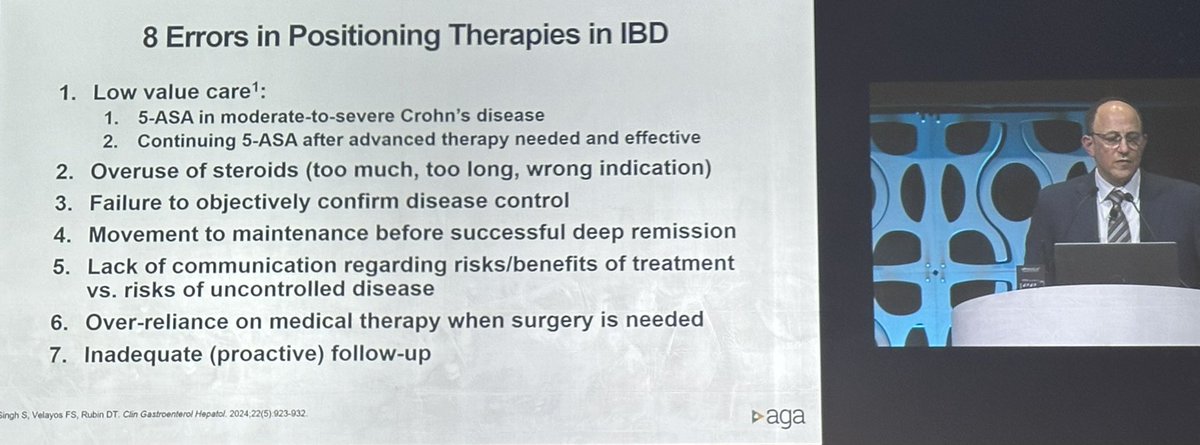
EIGHT mistakes doctors make in treating IBD - AVOID THESE!
David T Rubin, University of Chicago @DDWMeeting
138
18 May 2024
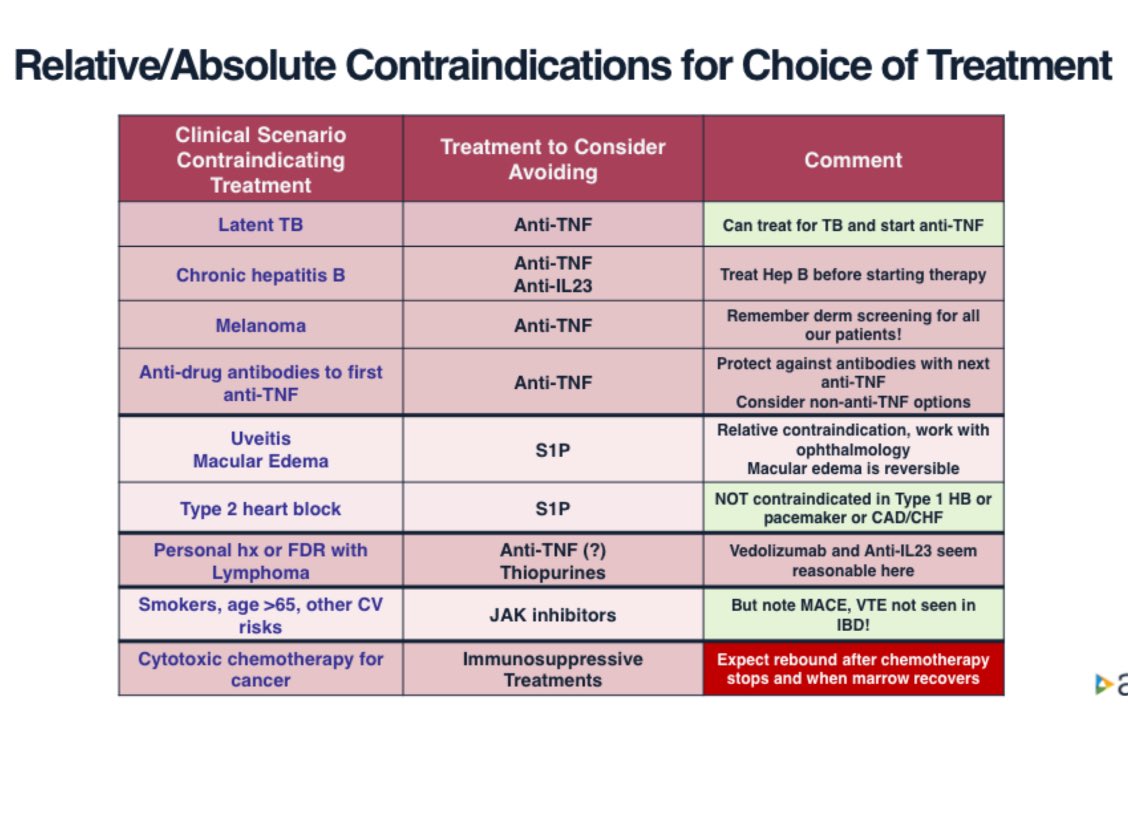
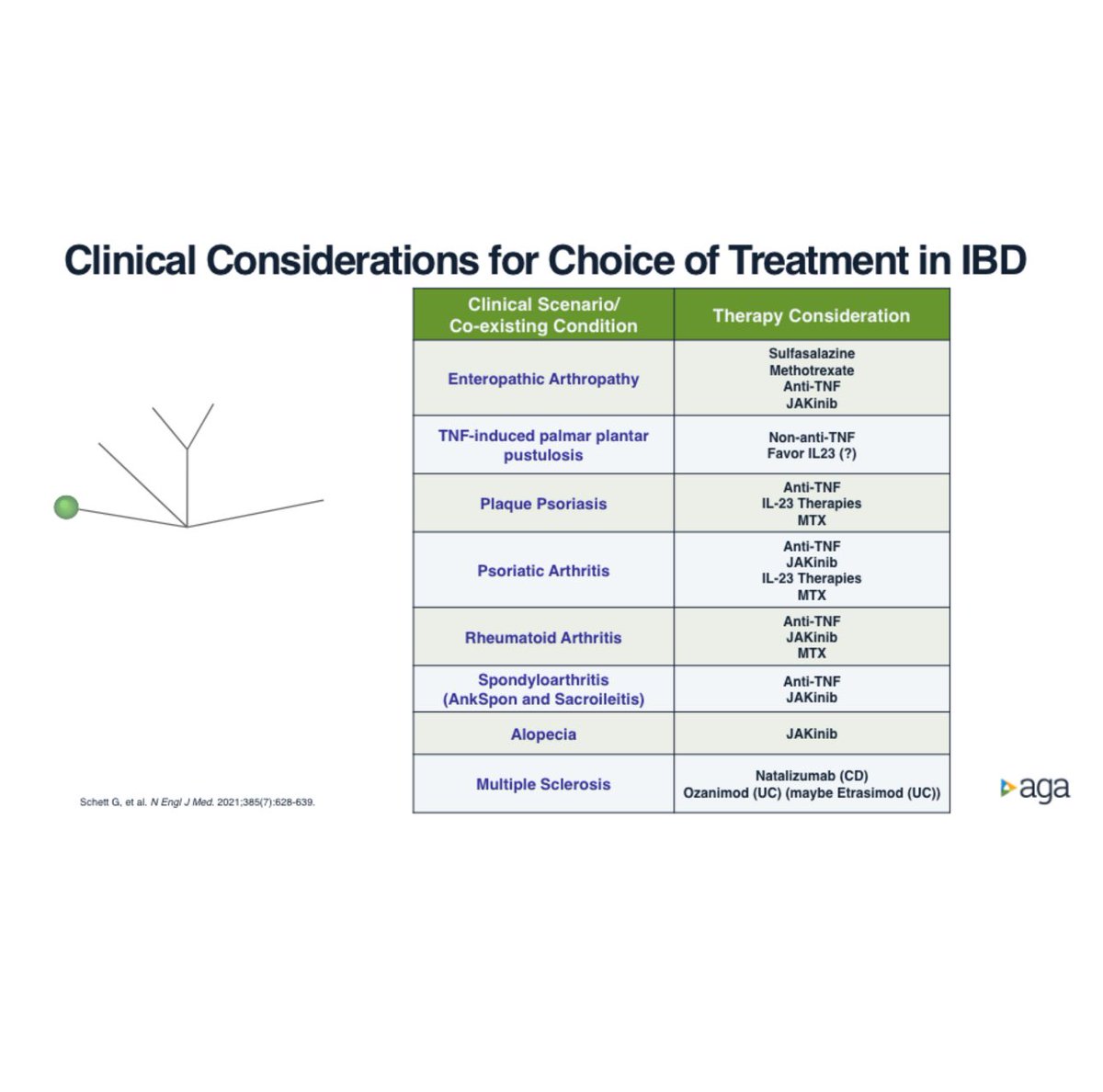
Choice of immunomodulatory therapies in IBD:
The story in 2024, summarised in just three slides
David T Rubin (University of Chicago) @DDWMeeting


1
2
6
308
18 May 2024
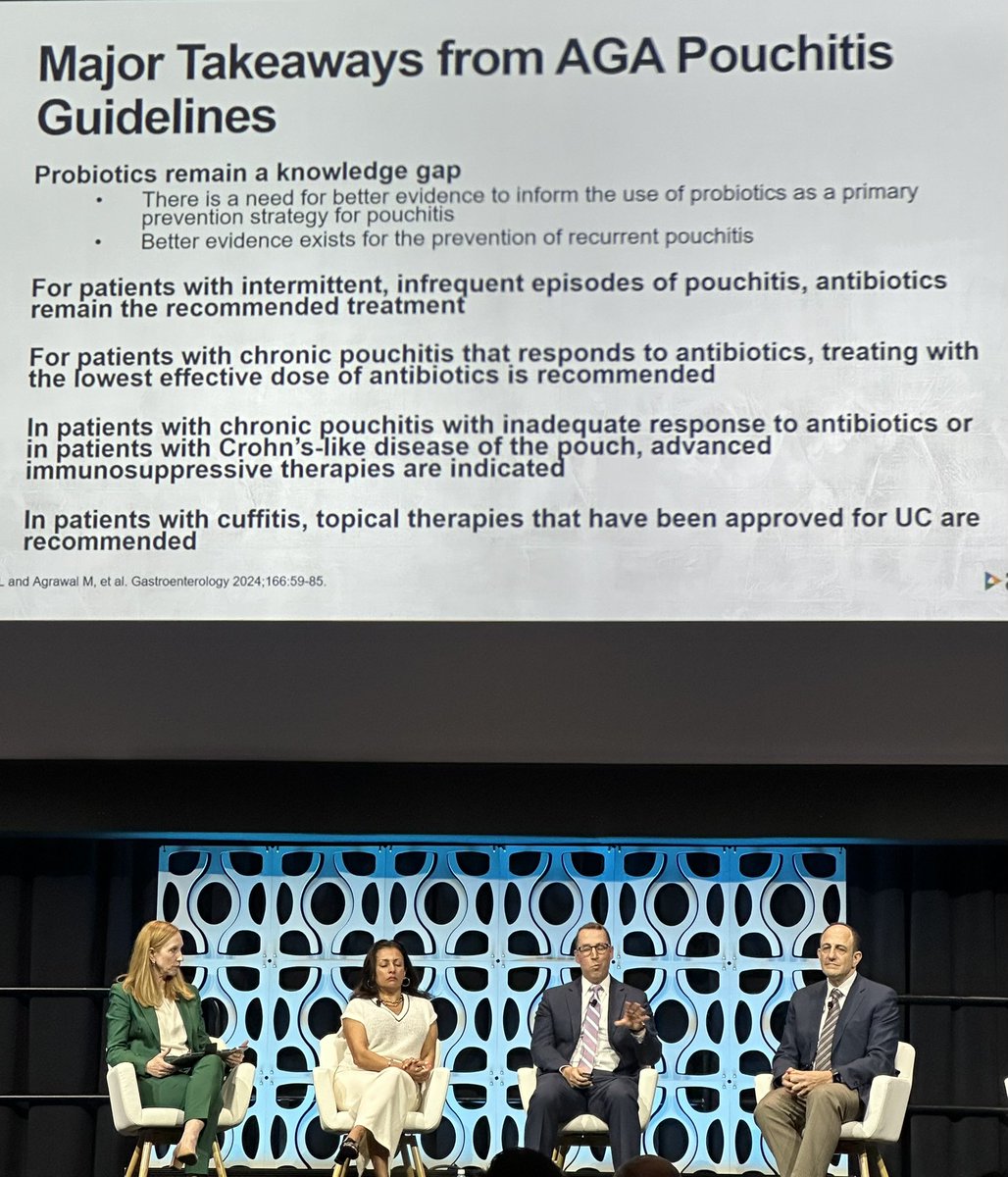
Pouchitis @DDWMeeting
Major Takeaways from @AGA_Gastro Pouchitis Guidelines - Ed Barnes, Chapel Hill
Probiotics, antibiotics, or immunomodulation for ‘Crohn’s’?
172