
Joined February 2010
- Tweets 960
- Following 654
- Followers 58
- Likes 153
3 Photos and videos
Witold retweeted

They're not actually moving. Trippy.
25
50
368
49,856
Witold retweeted

1,743
25,774
186,890
4,044,248

A major additional factor should be considered.
Satellites with localized AI compute, where just the results are beamed back from low-latency, sun-synchronous orbit, will be the lowest cost way to generate AI bitstreams in <3 years.
And by far the fastest way to scale within 4 years, because easy sources of electrical power are already hard to find on Earth. 1 megaton/year of satellites with 100kW per satellite yields 100GW of AI added per year with no operating or maintenance cost, connecting via high-bandwidth lasers to the Starlink constellation.
The level beyond that is constructing satellite factories on the Moon and using a mass driver (electromagnetic railgun) to accelerate AI satellites to lunar escape velocity without the need for rockets. That scales to >100TW/year of AI and enables non-trivial progress towards becoming a Kardashev II civilization.
1,213
1,944
17,321
6,606,187
Witold retweeted

25 Oct 2025
💥Rozmowa z profesor Grażyną Cichosz - technologiem żywienia rozniosła się w sieci z prędkością kosmiczną - obejrzało ją już 1 milion 300 tysięcy osób !
💥Bardzo Państwu dziękuję za wszystkie opinie - zarówno te entuzjastyczne ( „Pani profesor, mądra, odważna, wspaniala kobieta i racjonalna, walczy o zdrowie Polaków” ), jak i te krytyczne ( „zbyt wiele badań stoi w kontrze do tego co głosi pani profesor, prawda nie leży po jej stronie”- wp.pl ).
💥Bardzo liczę na to, że ten wywiad rozpocznie prawdziwą debatę technologów żywienia, dietetyków i lekarzy na temat jakości tego co jemy - a na Rymanowski Live wkrótce kolejni goście w tym temacie 👇👇👇
625
898
6,109
1,359,529
Witold retweeted

24 Jun 2025
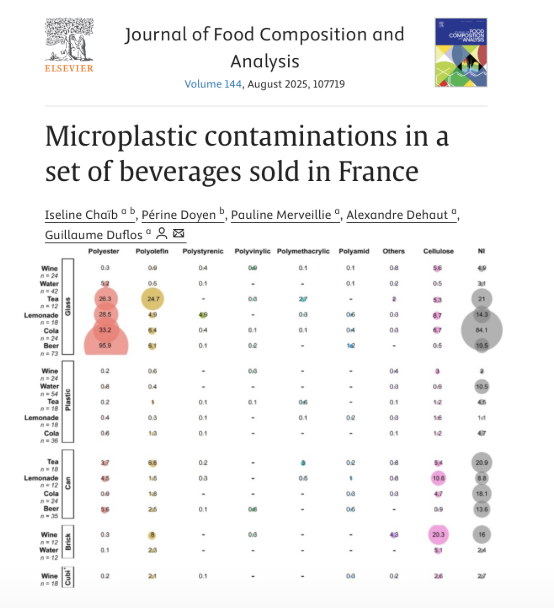
Glass had 5 – 50× higher plastic than plastic or cans
The French tested water, soda, beer, iced tea, lemonade, and wine sold nationwide and found that glass-bottled beverages carried far more plastic shrapnel than plastic bottles or cans.
🧵
398
747
8,384
1,575,182
Witold retweeted

6 Jun 2025
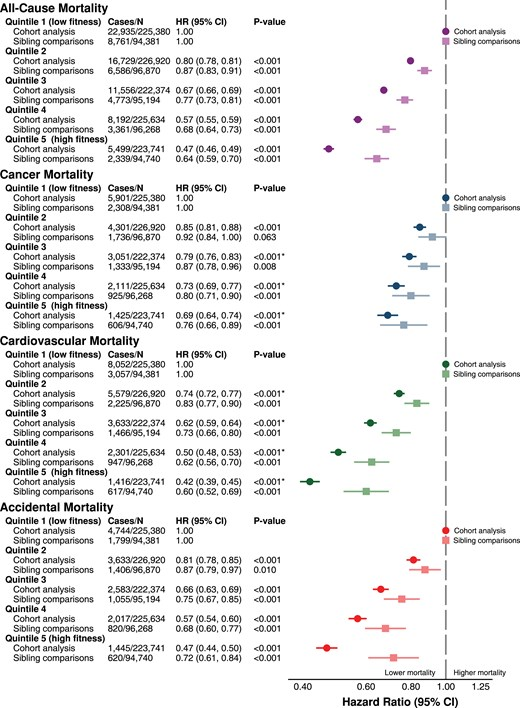
More evidence that the strong correlation between physical fitness and risk of death is heavily confounded by genetics and other factors.
This is a tough one for the preventive health community (including me)!
84
153
1,333
190,225

26 May 2025
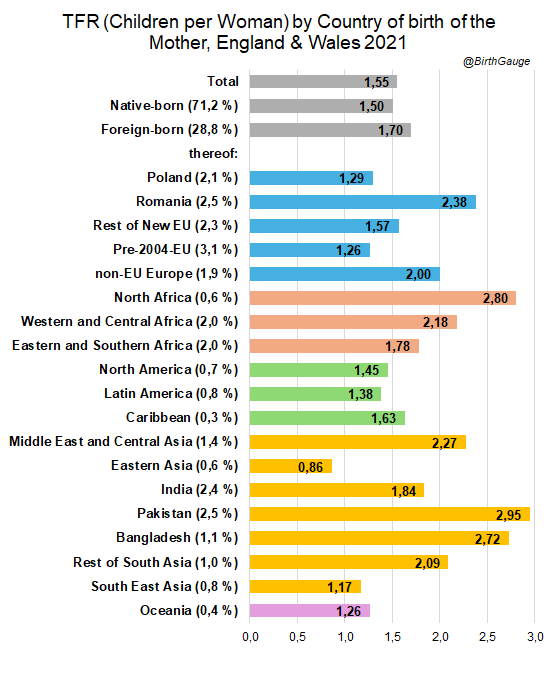
Dokładnie - Polki nie rodzą bo nie chcą.
26 May 2025

Czas skończyć z uporczywie pokutującym w przestrzeni publicznej poglądem, jakoby to Polki w UK rodziły niesłychanie duzo dzieci.
"Kultura się nie zmieniła, ale poprawiły warunki, to rodzą dzieci"
To ja mówię sprawdzam:
1
201
25 May 2025
Dlaczego Nawrocki jest 10 lat młodszy od Trzaskowskiego a wygląda na 10 lat starszego? Ktoś to zauważył? :)
80
Witold retweeted

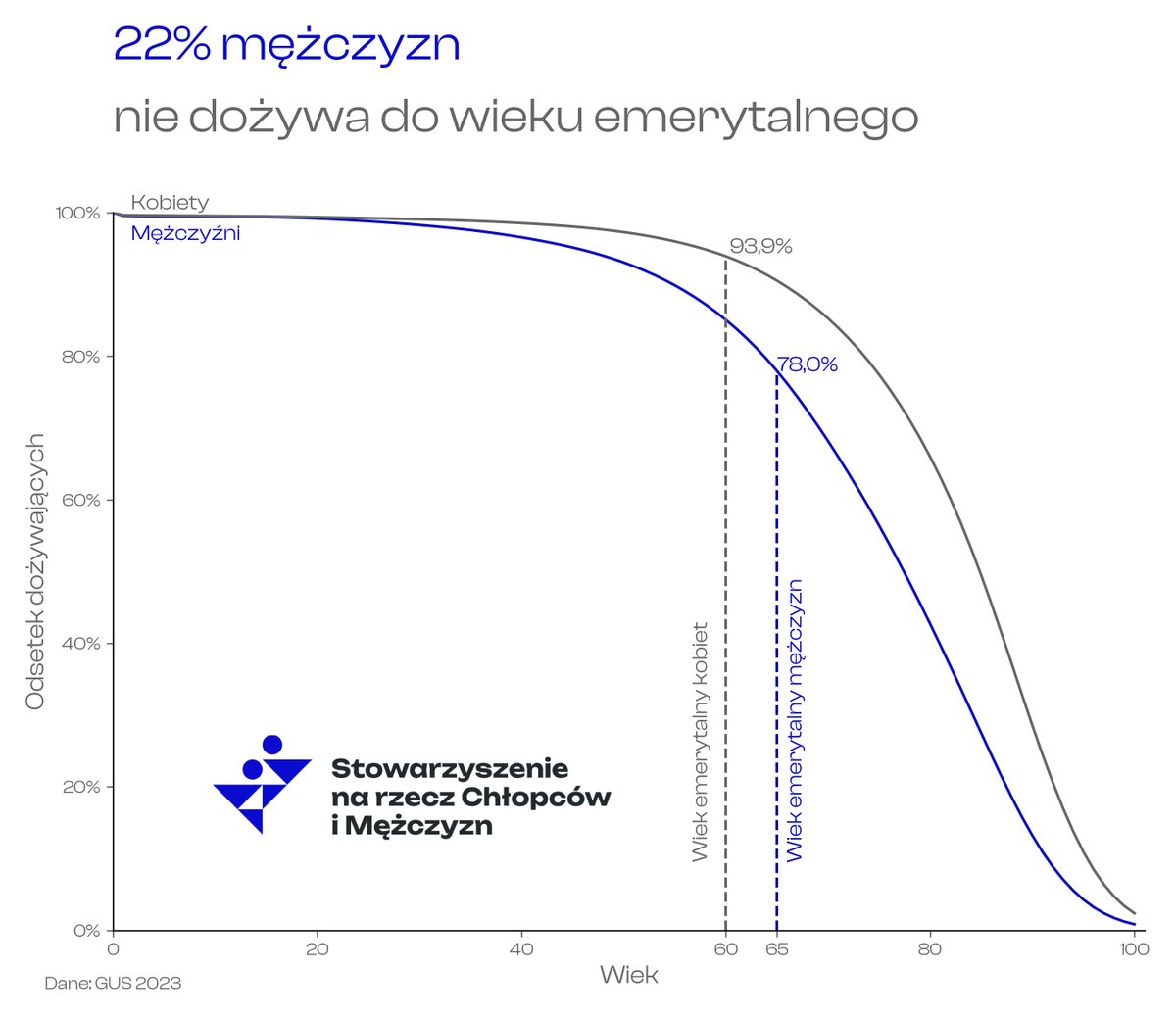
Na szczęście żyjemy co raz dłużej.
Ale wciąż 22% mężczyzn nie dożywa do wieku emerytalnego!
2
14
108
4,274
Witold retweeted

27 Apr 2025
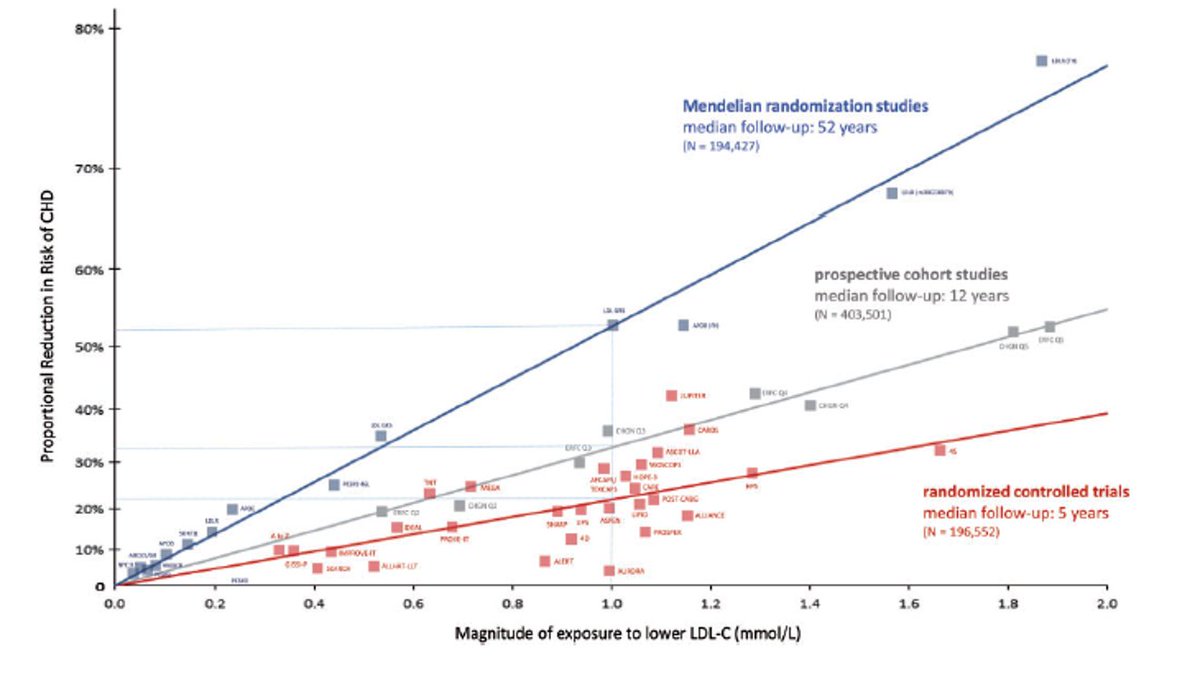
Mendelian Randomization is not appropriate for LDL-C. It fails the restrictions of the method.
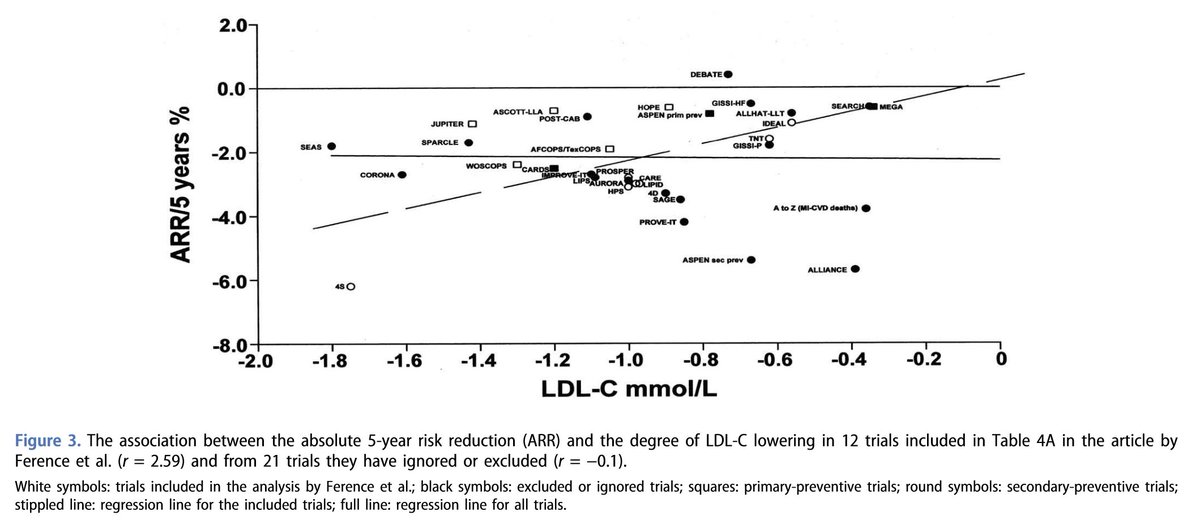
In Ference's figure 5a, they cherry-picked the papers so that they would have an association.
"According to Ference et al. [3], the most compelling clinical evidence for causality is provided by ‘the presence of more than 30 randomized cholesterol-lowering trials that consistently demonstrate that reducing LDL-C reduces the risk of CVD events proportional to the absolute reduction in LDL-C’. As previously noted, this is not true exposure–response. Furthermore, in their Figure 5(a), that illustrates the association, the authors have only included data from 12 of the 30 trials they refer to. If all of the trials in Table 1 are included, as we have done in Figure 3, there is no association between LDL-C lowering and coronary event rate."
Ravnskov, U., Lorgeril, M. de, Diamond, D. M., Hama, R., Hamazaki, T., Hammarskjöld, B., Hynes, N., Kendrick, M., Langsjoen, P. H., Mascitelli, L., McCully, K. S., Okuyama, H., Rosch, P. J., Schersten, T., Sultan, S., & Sundberg, R. (2018). LDL-C Does Not Cause Cardiovascular Disease: A Comprehensive Review of the Current Literature. Expert Review of Clinical Pharmacology, 11(10), 959–970. doi.org/10.1080/17512433.201…
26 Apr 2025

Here you go, this represents hundreds of thousands of study subjects in rigorous well designed trials. Ference et al Eur Heart J 2017. Everyone can plot their own "average" risk on this graph. 1 mmol/L = 38.67, so 2.5 mmol/L is about 100 mg/dL. Bottom line; risk for CVD at population level (not individual level per se) is proportional to "walking around" LDL-C, but risk is higher if you had a prior event. Of course the issue is one cant predict risk with certainty at individual level. If we could then we would not need to treat so many people. Maybe some day we will be better able to define risk at individual level to "personalize" therapies, but I suspect not in next 1-2 decades.
9
18
106
29,765
27 Apr 2025
Seems that keto is the only logical solution - fat and protein are difficult to overeat, and You gain the possibility to pee out calories and/or breathe out calories in the form of ketones...
27 Apr 2025

Just because weight loss comes down to a calorie deficit does not mean that obesity is a choice.
Appetite (biology) with our environment drives the behavior of eating.
1
140
Witold retweeted

3 Mar 2025
The Oval Office just turned into a battle arena! 🥊💥
Who’s winning this historic clash🤔
57
4
44
7,594
23 Mar 2025
Frankenstein diet not so effective it seems…
23 Mar 2025

Dear @bryan_johnson,
Do you have a response to this? I've questioned your testosterone levels in the past - 900 on a calorie restricted vegan diet with no TRT? I doubt it - asking you for LH/FSH levels to corroborate your claims about not being on androgen enhancement.
1
283
23 Mar 2025
And I guess it mentions veggies 0 times… simply because they were invented yet. :)
22 Mar 2025

The Bible mentions:
Lamb 200 times.
Raw Milk 50 times.
Cows 270 times.
Pomegranates 33 times.
Sourdough Bread 360 times.
Goats 88 times.
Figs 55 times.
Fish 40 times.
Raw Honey 61 times.
Butter 10 times.
Salt 40 times.
Olive Oil 191 times.
EAT BIBLICALLY.




1
215
22 Mar 2025
Tasty and healthy! :)
21 Mar 2025

This is how you save your health and the planet.
A plant-based steak made from a vegan cow.

1
130
Witold retweeted

13 Mar 2025
if this video reaches your timeline, everything will be okay ❤️
1,392
24,453
267,111
3,890,404
5 Mar 2025
Ciekawe…
4 Mar 2025

To nie są normalne wybory polityczne, to spór pokoleniowy. Jeszcze nigdy nie było takiej przepaści pomiędzy najmłodszymi i najstarszymi wyborcami w Polsce. Fakt, że ten spór nie istnieje w debacie publicznej pokazuje wszystkie problemy naszej demokracji.

203